
















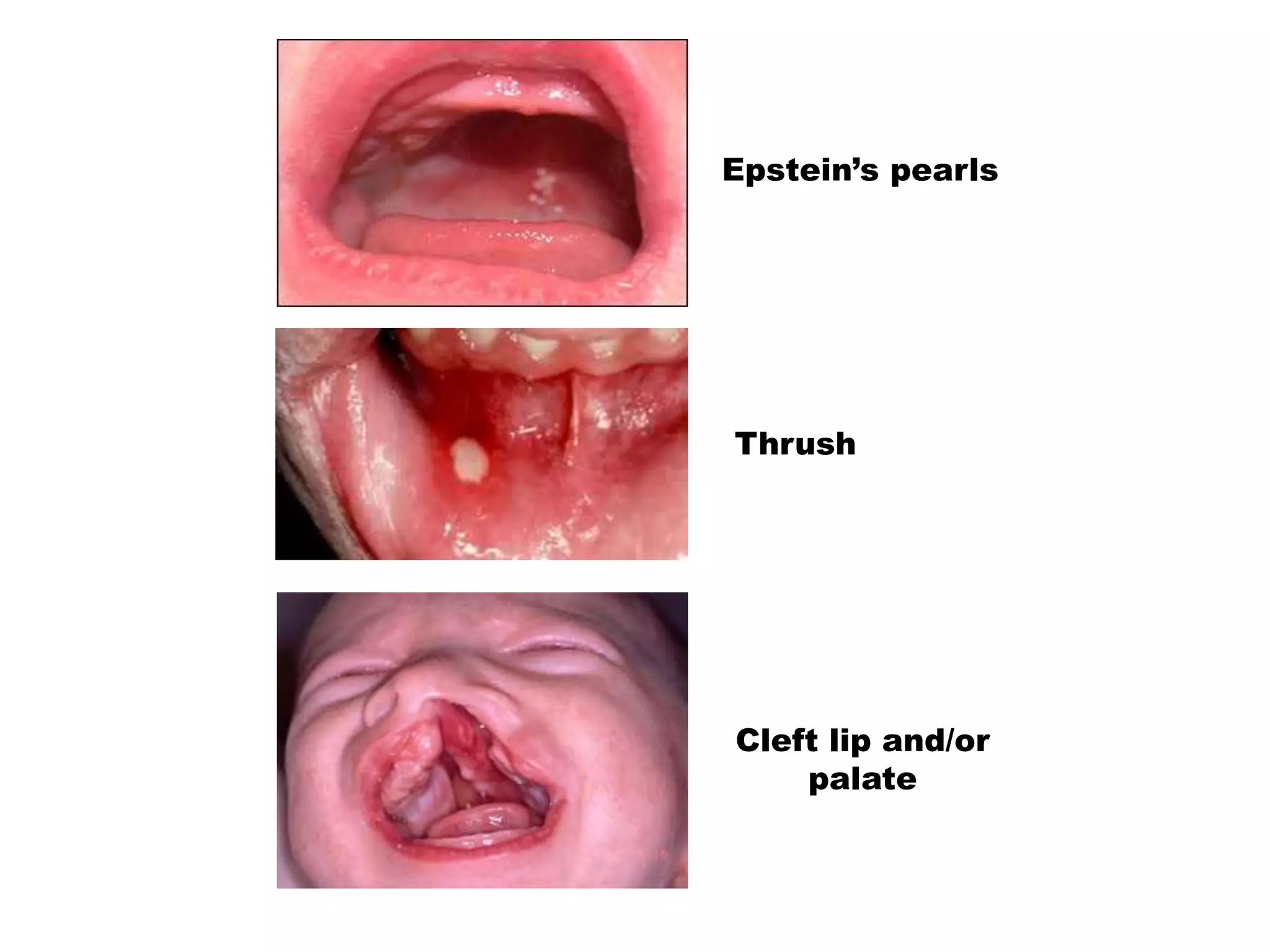












































The document describes normal findings and abnormalities that may be seen during a physical examination of the eyes, ears, nose, mouth, throat, heart, lungs, abdomen, and other body systems in infants and children. Key points include normal eye alignment and pupil appearance/reaction, typical ear canal findings, common oral structures in newborns, normal breath and heart sounds, expected abdominal exam findings, and signs that warrant further evaluation such as eye misalignment, ear discharge, oral lesions or thrush, respiratory distress, murmurs, or abdominal tenderness.















































































