Download as PDF, PPTX





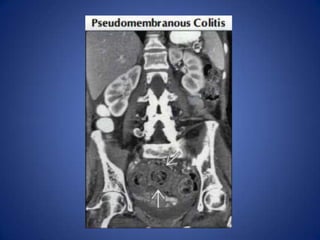











The document discusses the differential diagnosis for acute left lower quadrant pain, highlighting common and less common causes, including diverticulitis, colon carcinoma, and gynecologic issues. It emphasizes the importance of imaging, specifically CECT, and provides detailed descriptions of conditions like epiploic appendagitis and pseudomembranous colitis. Additionally, the document covers less common causes such as ischemic colitis and abdominal abscess, offering clues for diagnosis.























































































