
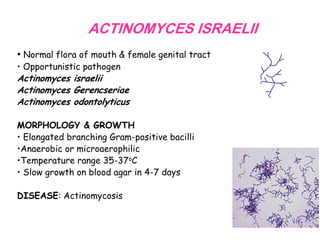
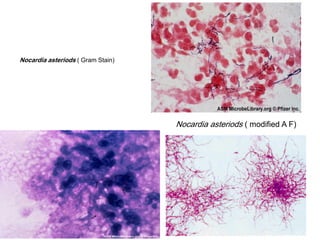

This document discusses Actinomyces and Nocardia infections. Actinomyces israelii is normal flora that can cause actinomycosis, a chronic infection presenting with hard swellings that drain pus through sinuses. Diagnosis involves finding sulfur granules or filamentous bacteria on smears and cultures. Treatment is surgical drainage and penicillin. Nocardia species like N. asteroides are environmental bacteria that can cause pulmonary or skin infections. Diagnosis involves identifying thin, branching, weakly acid-fast filaments on smears and cultures. Treatment involves drainage and antibiotics like TMP-SMX.


















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

