Downloaded 1,457 times
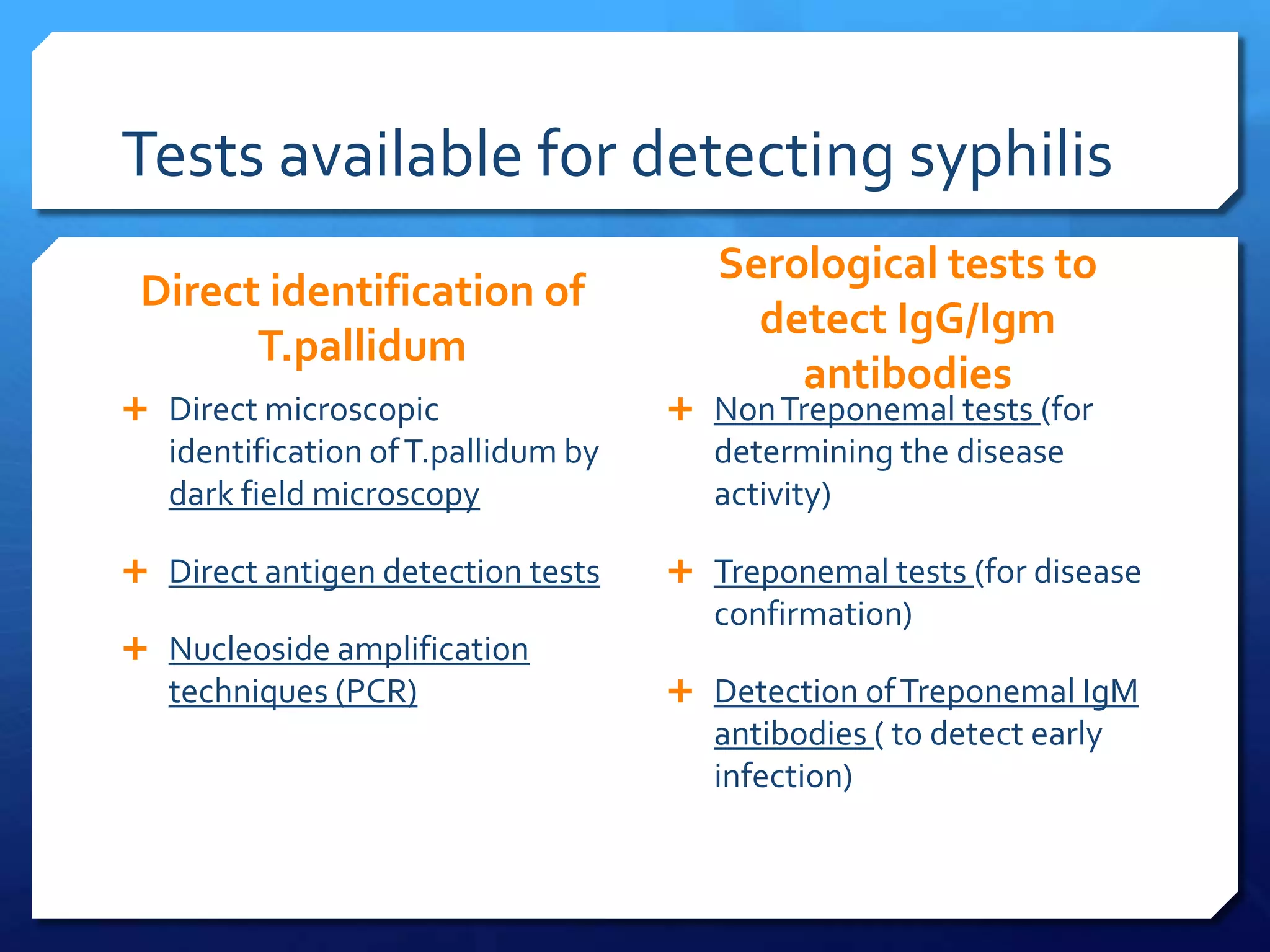
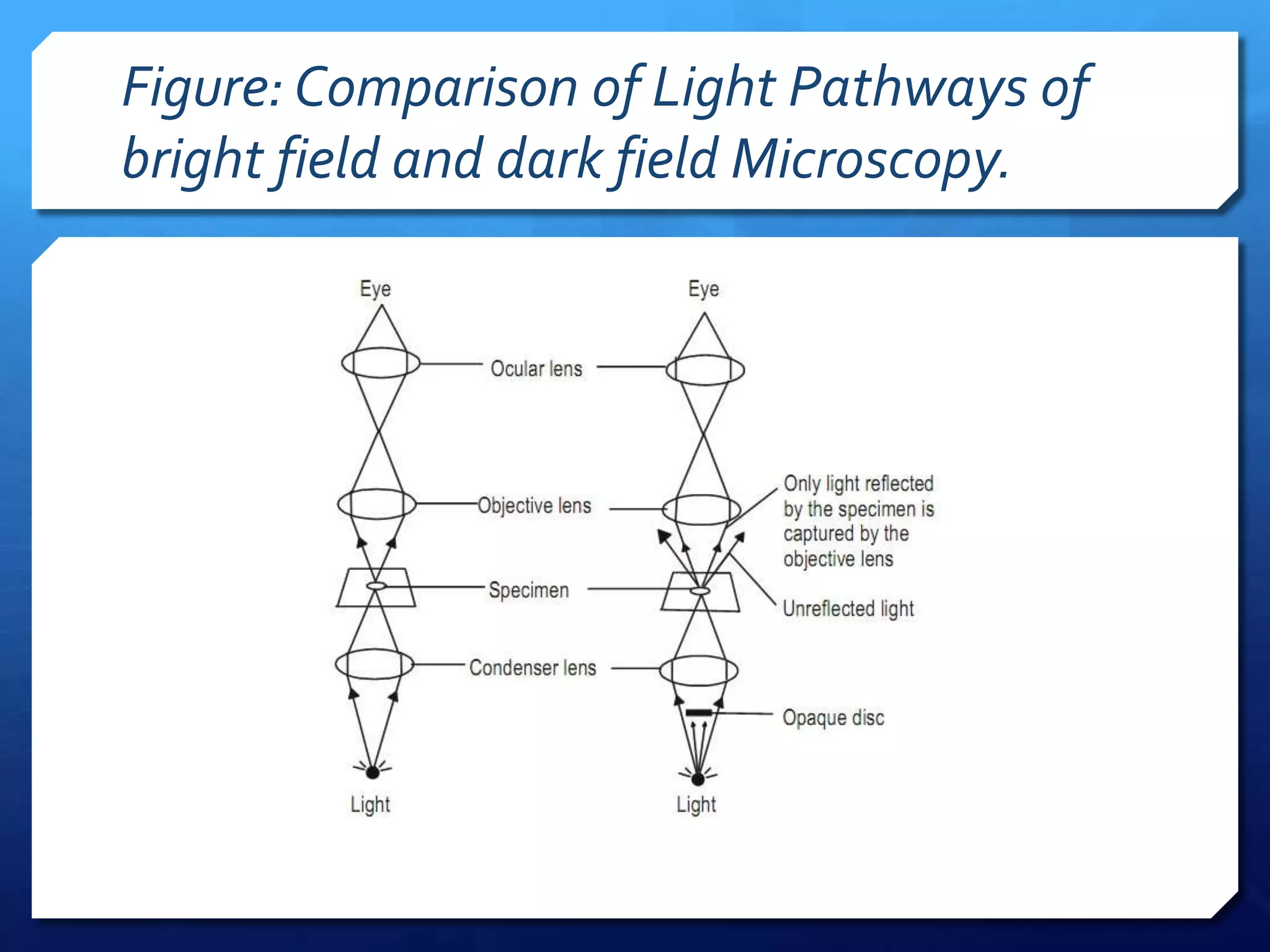
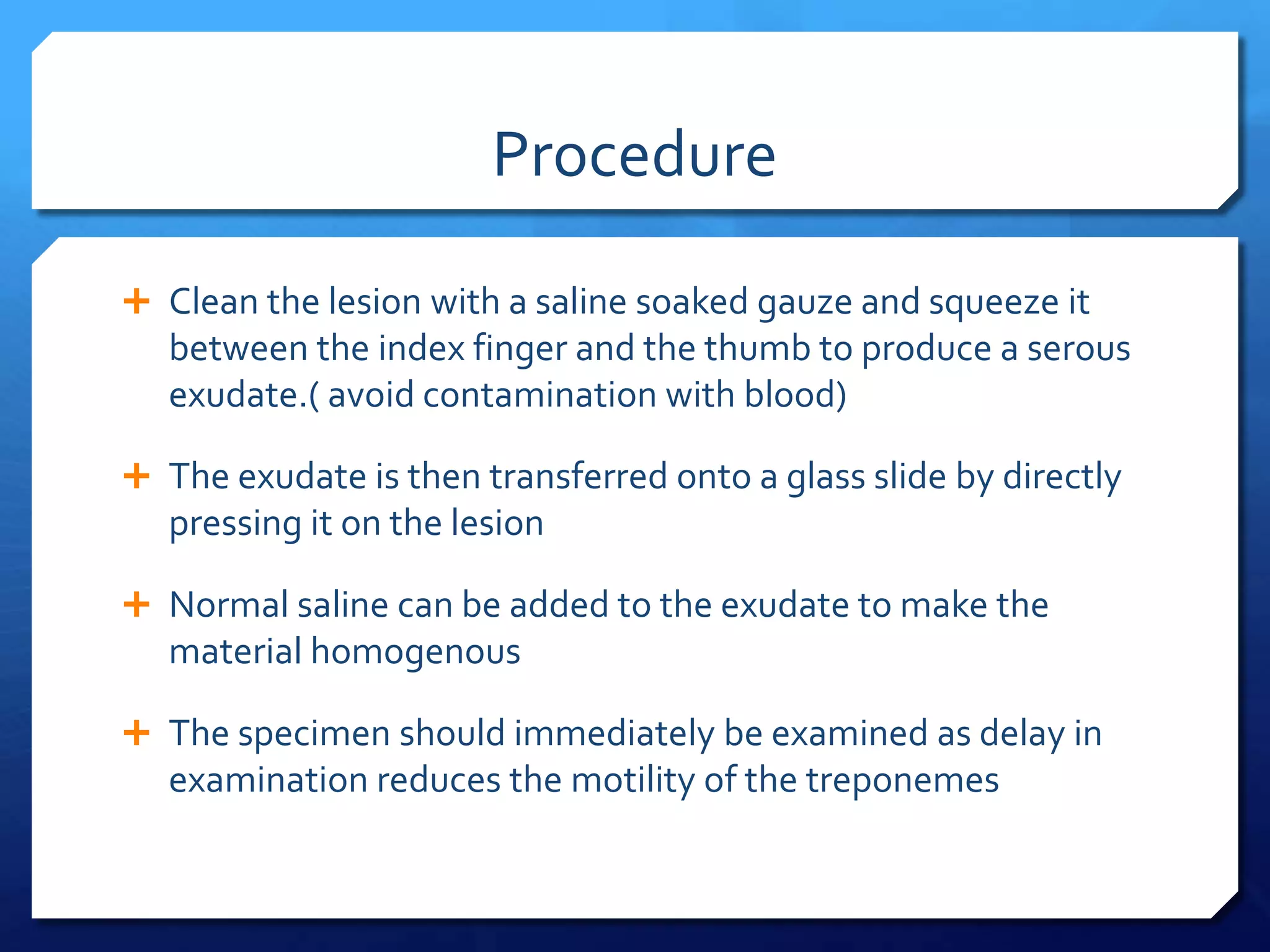
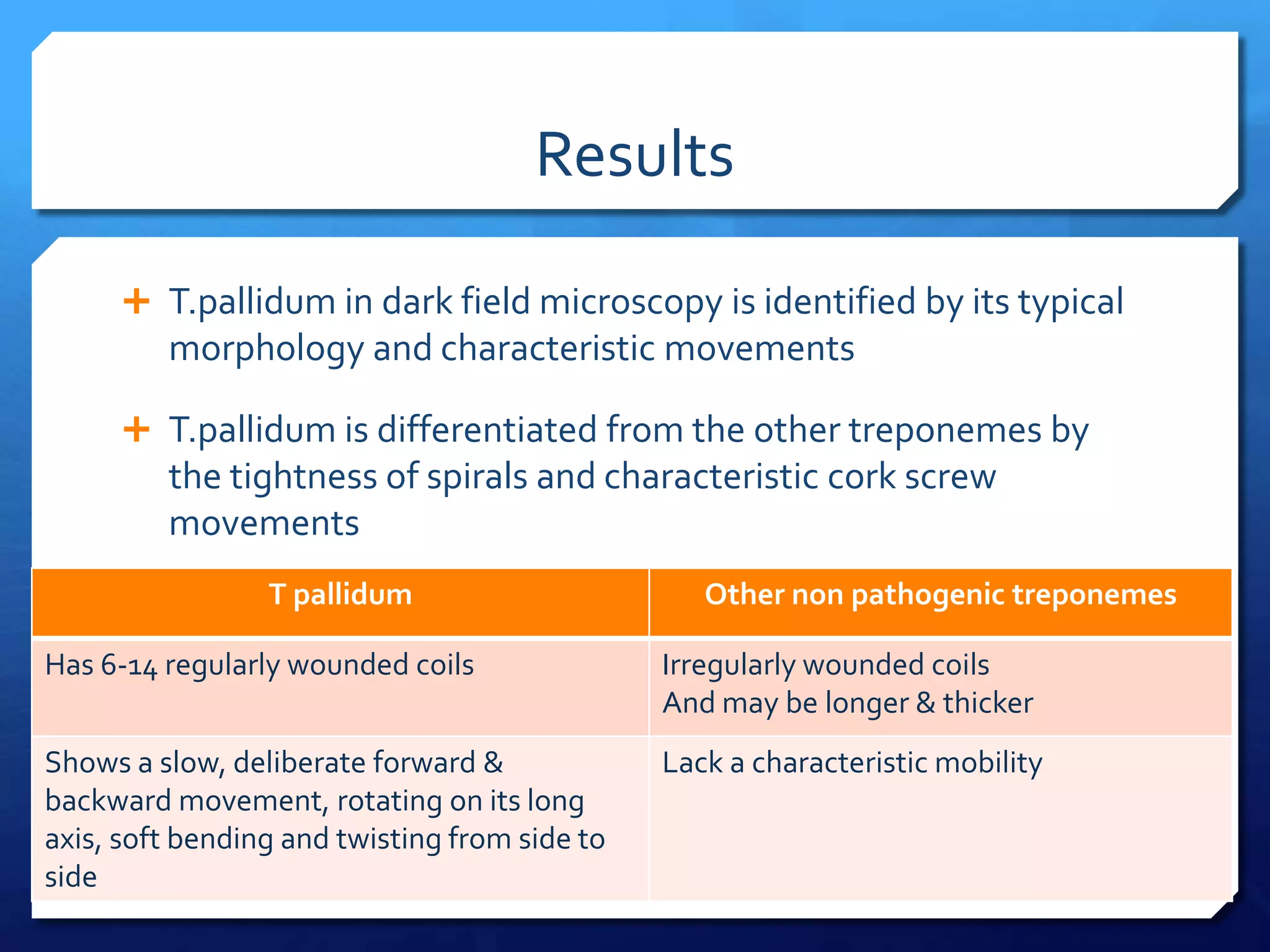
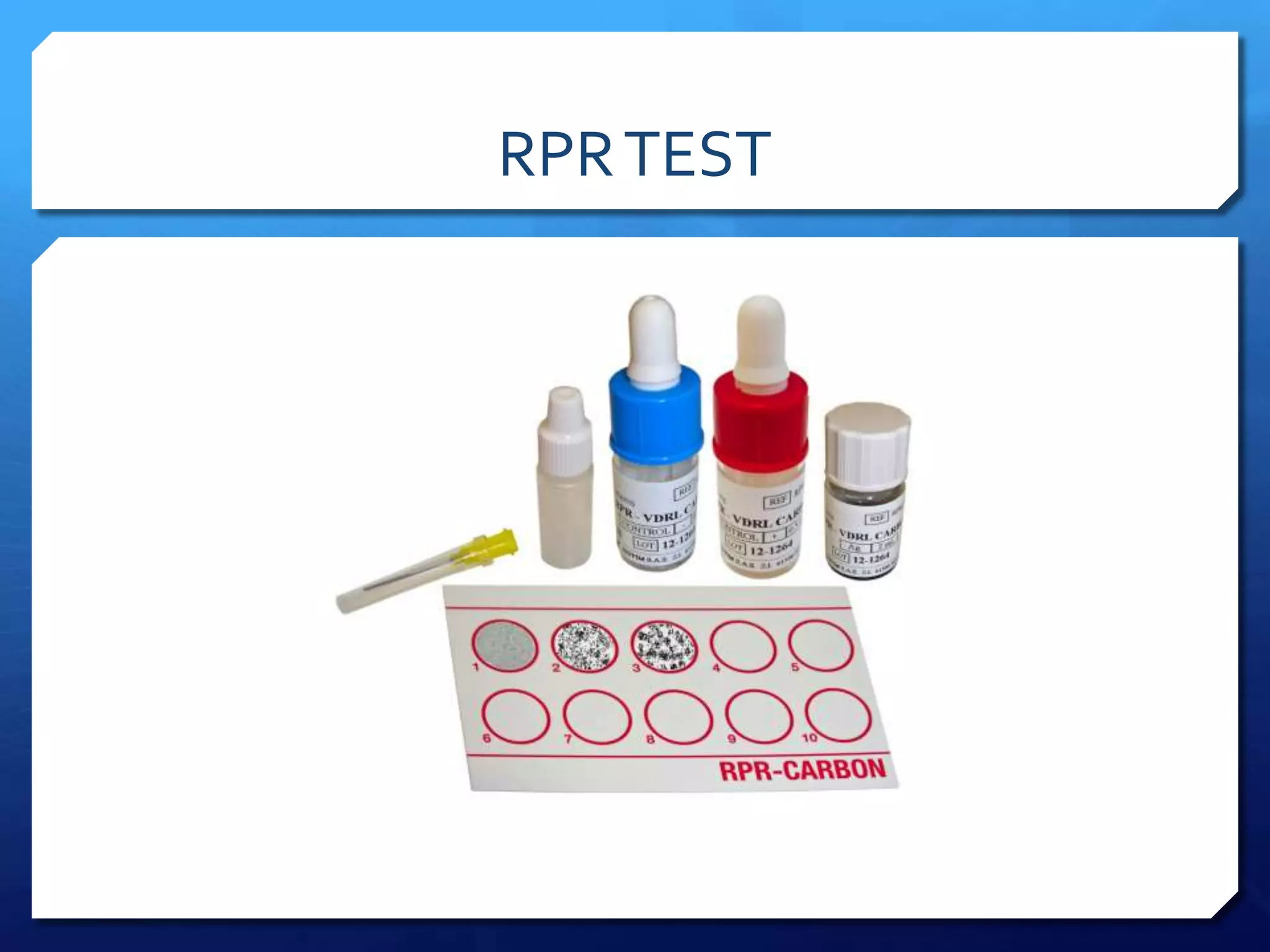
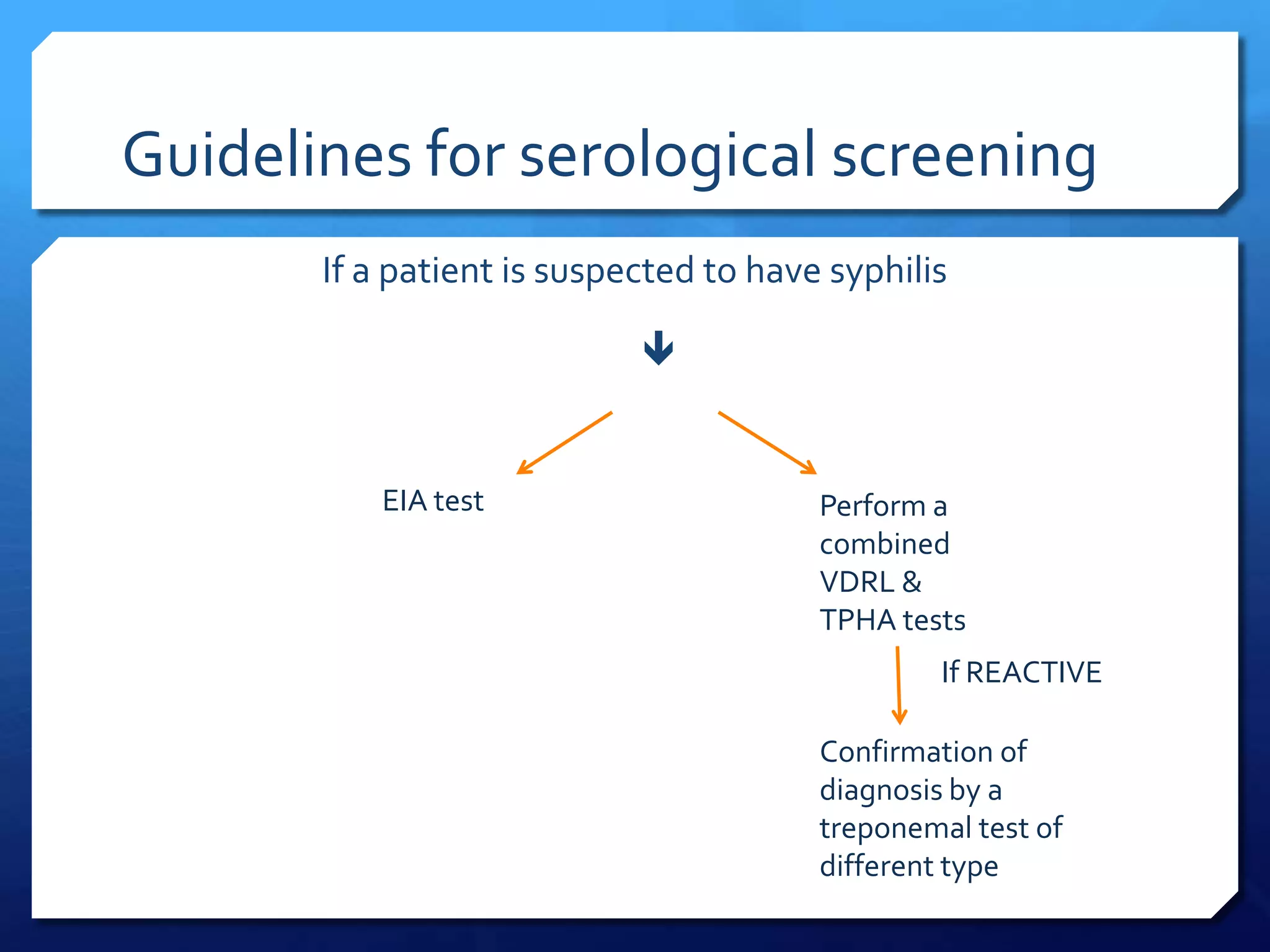
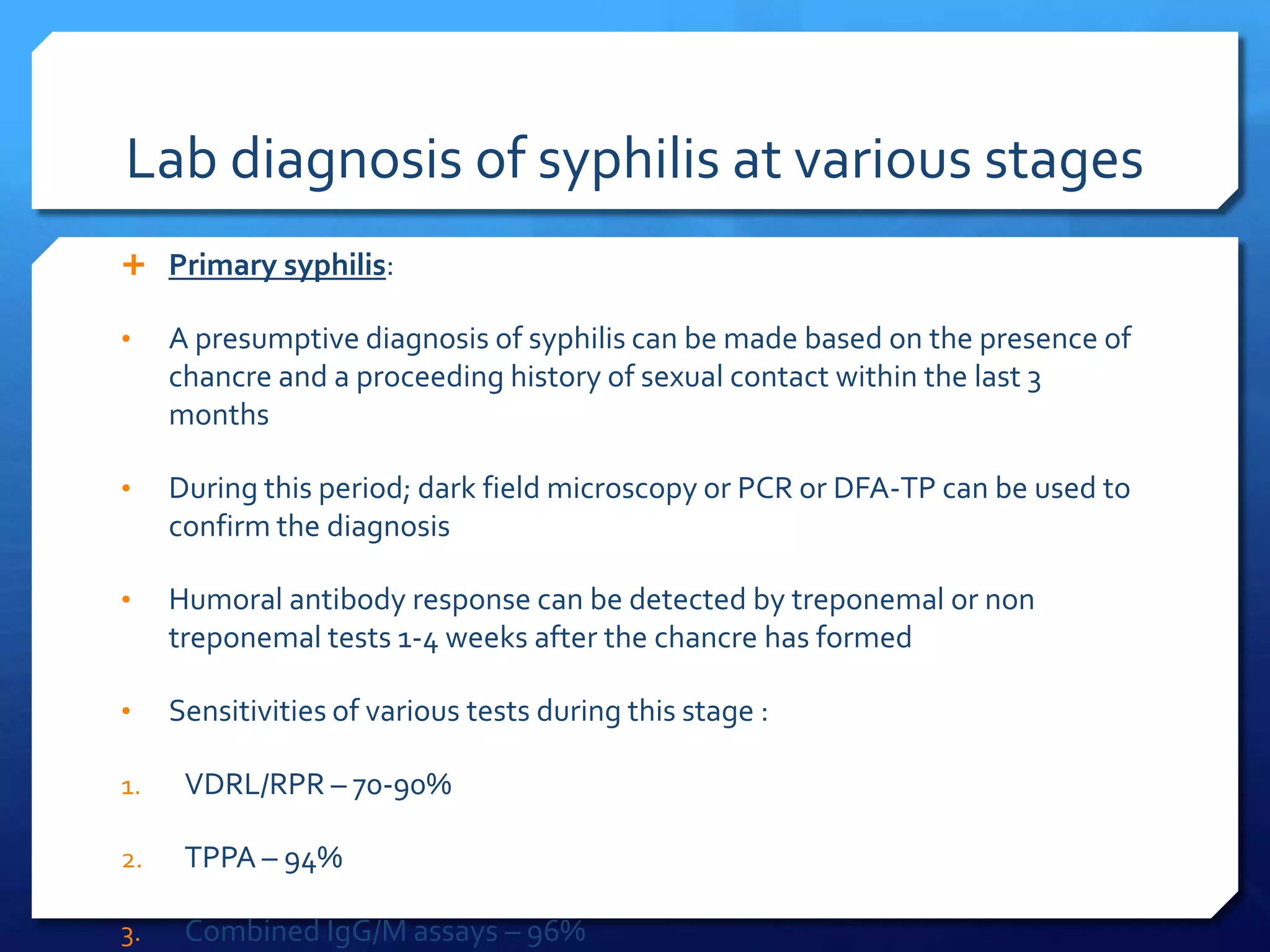


1. There are two main types of tests for diagnosing syphilis - direct tests that detect the bacteria Treponema pallidum, and indirect serological tests that detect antibodies produced in response to the infection. 2. Direct tests include dark-field microscopy, direct fluorescent antibody testing, and PCR to identify the bacterium in lesions. Serological tests include non-treponemal tests like VDRL and RPR that detect nonspecific reagin antibodies, and treponemal tests like FTA-ABS, TPHA, and EIA that detect treponema-specific antibodies. 3. Dark-field microscopy examines exudate from lesions under a dark-field microscope to visualize































































![Syphilis new.pptx [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/syphilisnew-190407075658-thumbnail.jpg?width=640&height=640&fit=bounds)



























![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

