Downloaded 46 times


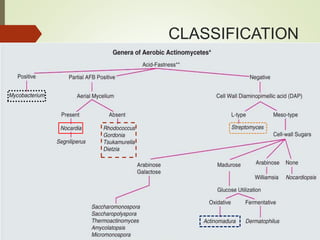

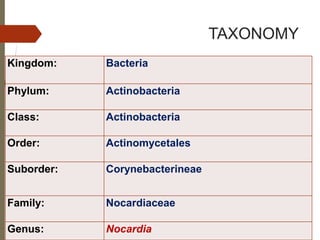

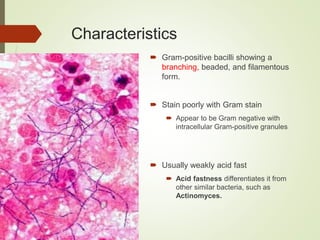
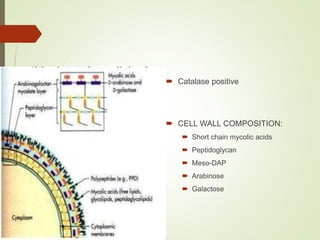
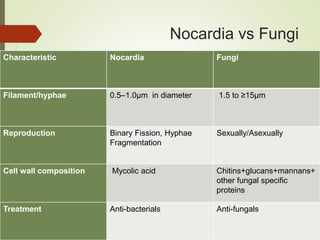



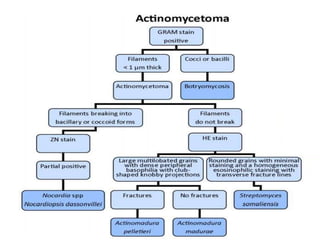
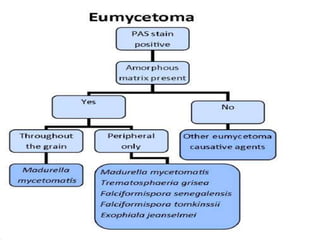
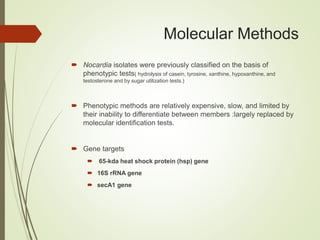
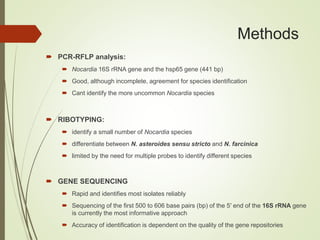


This document discusses the aerobic actinomycete Nocardia. It begins by classifying Nocardia taxonomically and noting it is an opportunistic pathogen found in soil. The document then covers the epidemiology, pathogenesis, clinical manifestations including pulmonary, skin and disseminated infections, diagnosis through microscopy, culture and molecular methods, and treatment with antimicrobials. In summary, Nocardia is an environmental actinomycete that can cause infection in immunocompromised individuals, with pulmonary disease being most common and diagnosis relying on microscopy, culture and molecular identification methods.



































































