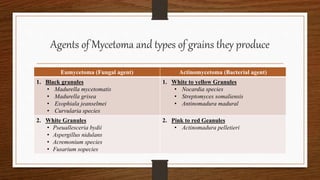
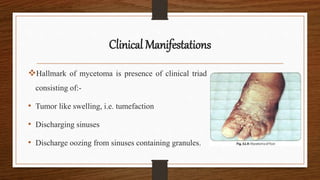
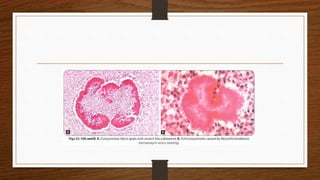
Mycetoma, or subcutaneous mycoses, is a chronic infection characterized by swelling, discharging sinuses, and granules, primarily caused by fungal (eumycetoma) or bacterial (actinomycetoma) agents found in soil. The pathogenesis involves traumatic skin entry, with actinomycetoma being more prevalent globally. Diagnosis includes direct examination and cultures, while treatment requires surgical removal and appropriate antifungal or antibiotic therapy.