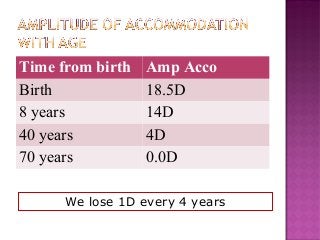
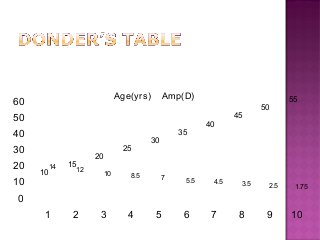
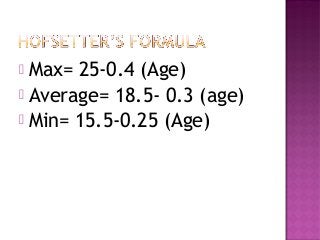

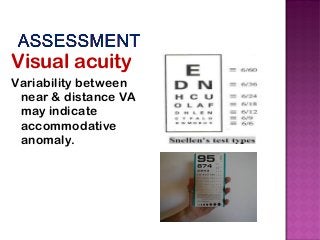


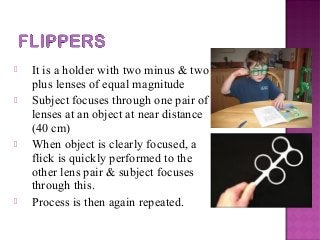
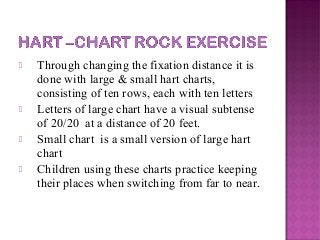
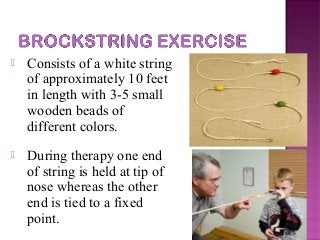


This document discusses accommodative insufficiency, including its definition, signs and symptoms, assessment methods, and management approaches. Accommodative insufficiency is characterized by an inability to focus or sustain focus at near due to an insufficient amplitude of accommodation based on age-expected norms. Evaluation involves assessing near point of accommodation and determining amplitude of accommodation. Management includes prescribing reading glasses to reduce accommodative demand, vision therapy using techniques like flippers and Hart charts to strengthen accommodation, and occasionally multifocal lenses. The goal of treatment is to improve the ability to make rapid accommodative responses without fatigue.























































































