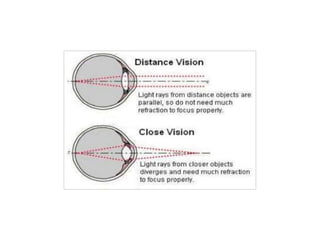
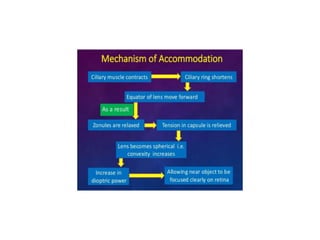
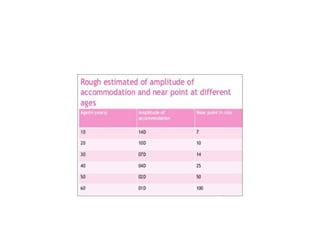
This document discusses accommodation and presbyopia. It defines accommodation as the ability of the eye to change focus from distant to near objects by changing the shape of the lens. Accommodation decreases with age in a process called presbyopia as the lens becomes less flexible. Presbyopia symptoms include difficulty seeing close objects clearly and can be treated with reading glasses, bifocal glasses, or multifocal contact lenses to restore near vision. The document also covers topics like ciliary muscle function, amplitude of accommodation measurement, and factors affecting presbyopia.