Download to read offline
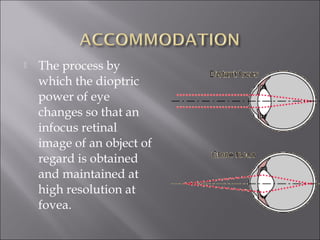
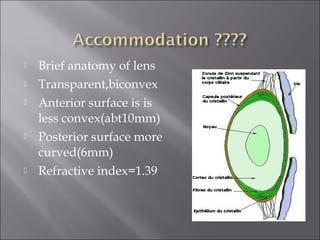



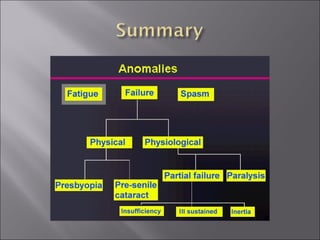

This document discusses accommodation and presbyopia. It begins by defining accommodation as the process by which the eye focuses on near objects. It then describes accommodation anatomy and the ranges and variation of accommodation with age. Presbyopia is introduced as a normal age-related condition where accommodation decreases. Theories of presbyopia are presented along with treatment options like glasses and contact lenses. Accommodative disorders like spasm and insufficiency are also summarized.




















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

