Downloaded 714 times

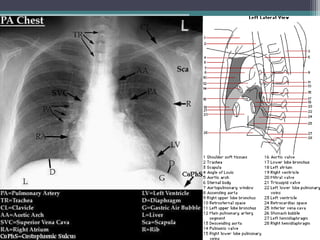
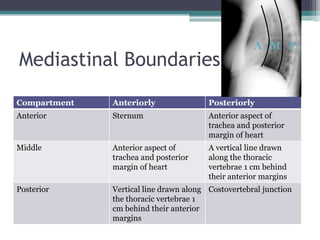
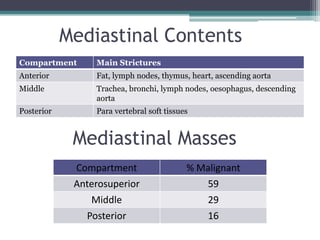
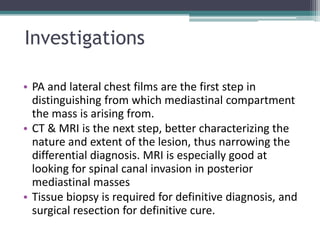
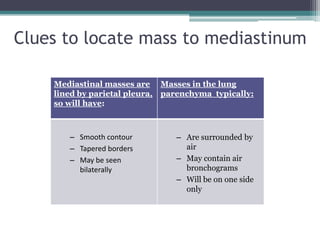




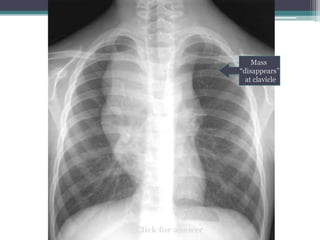





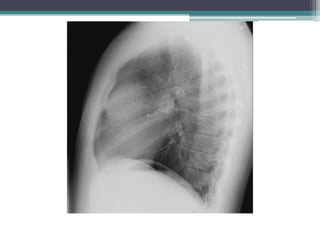


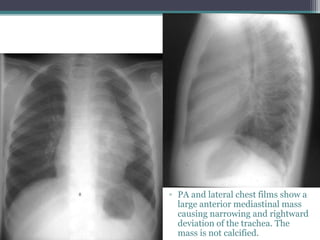
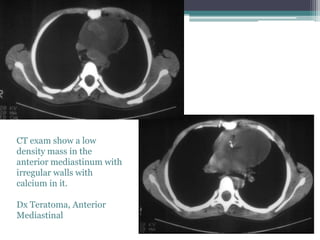
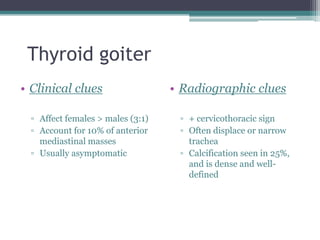
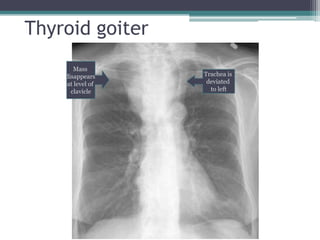


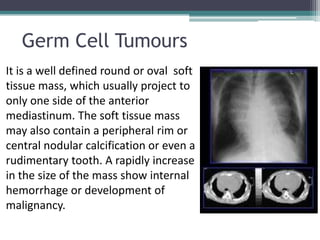
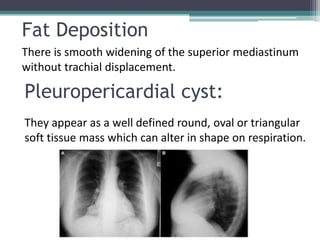
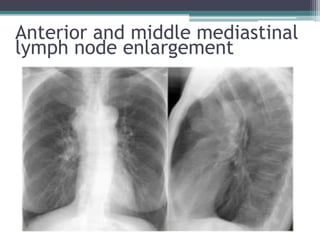
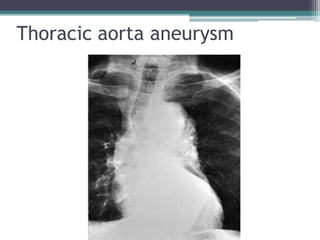



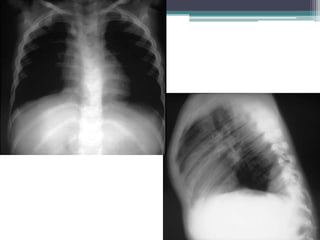
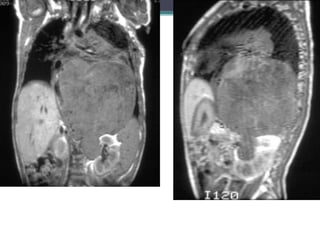
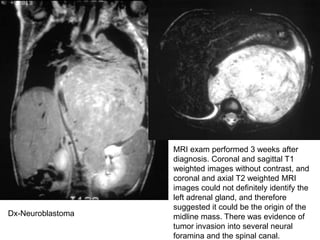

The document discusses mediastinal masses. It begins by defining the mediastinum and its boundaries. It then discusses approaches to evaluating mediastinal masses including distinguishing their location based on chest x-ray findings. Common masses are then reviewed for each compartment - anterior, middle, and posterior. Anterior masses include thymoma, teratoma, thyroid goiter, and lymphoma. Middle masses include adenopathy, primary neoplasms, aneurysms, and abnormalities. Posterior masses are often neural tumors, but can also include vertebral abscesses or vascular structures. Example cases are provided to demonstrate key radiographic findings.






























































































