This document provides an overview of Doppler ultrasound of the normal portal system. It discusses adjusting spectral Doppler settings and interpreting normal and abnormal findings. Key points include:
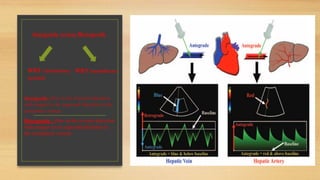
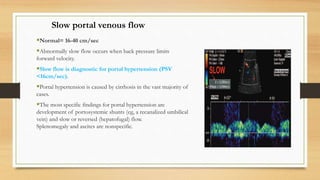
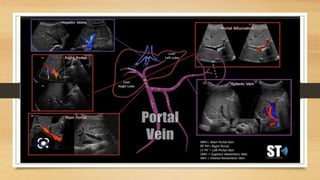
- Normal Doppler findings of the portal vein include a velocity of 13-23 cm/sec and antegrade flow. Increased diameter or retrograde flow indicate portal hypertension.
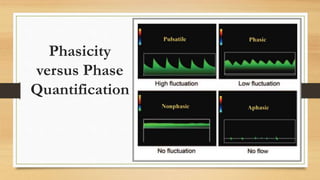
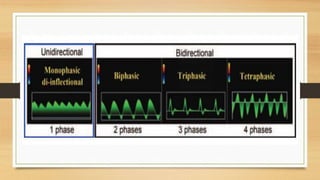
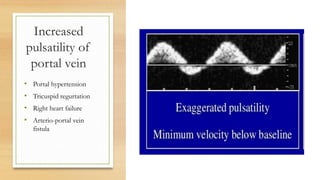
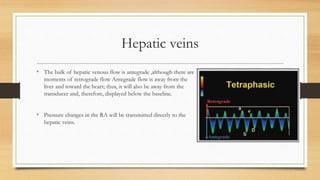
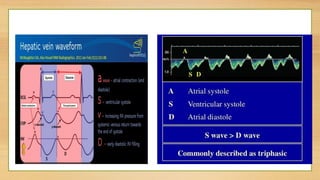
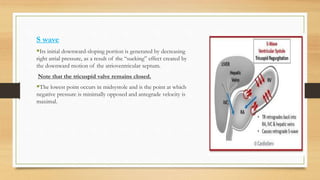
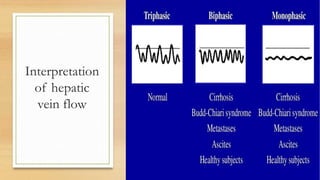
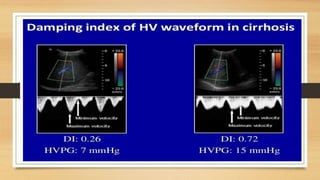
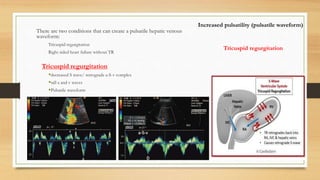
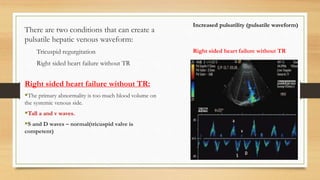
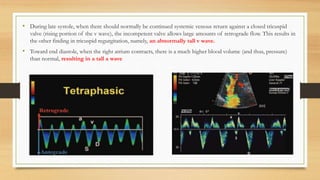
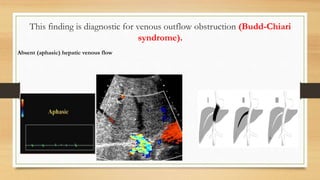
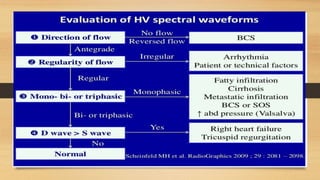
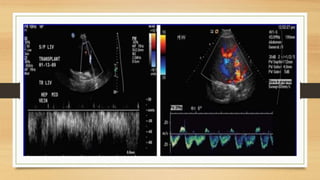
- Hepatic vein Doppler shows a triphasic waveform. Increased pulsatility can be seen with tricuspid regurgitation or right heart failure. Loss of phasicity indicates outflow obstruction.
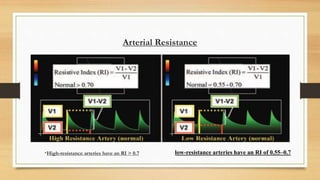
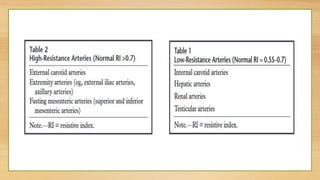
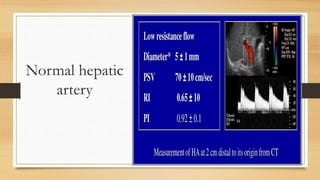
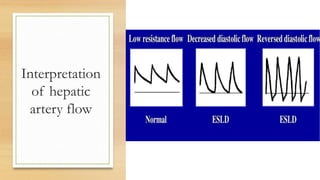
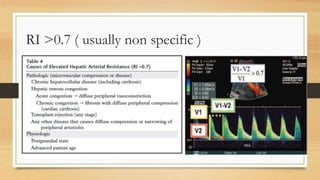
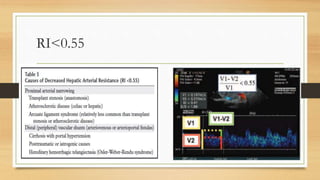
- The hepatic artery has a resistive index over 0.7 normally. Values under 0.55 may indicate stenosis.
- Transjugular intrahepatic portos