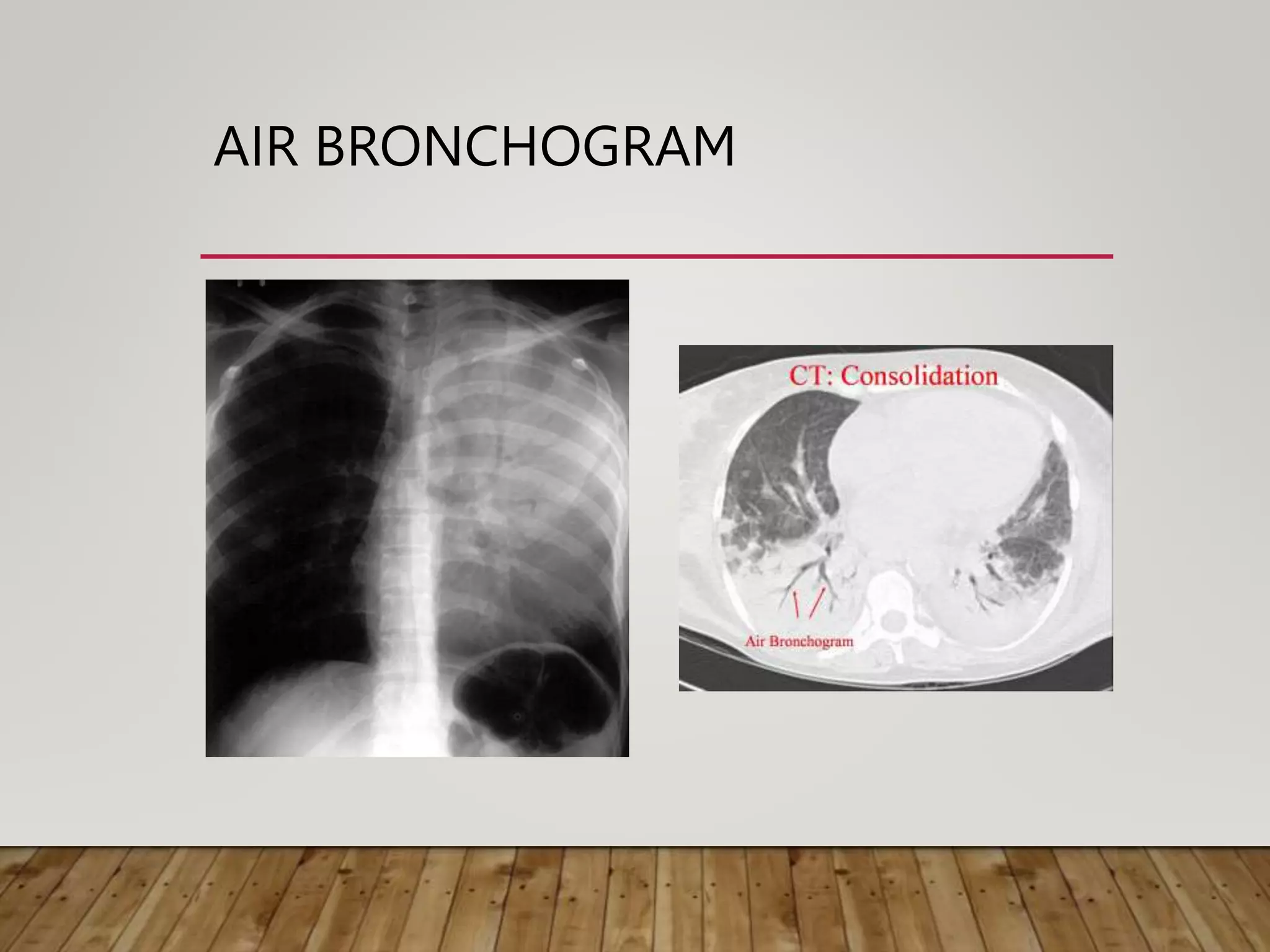
This document provides information on interpreting chest x-rays. It discusses how different tissues absorb x-rays differently, appearing white, grey, or black on images. It also describes common views, quality factors, and techniques for localizing abnormalities. Various pathologies are then outlined, including signs like air bronchograms that indicate a lesion is intra-pulmonary. Specific patterns such as reticulation, nodules, and honeycombing are also detailed.