Downloaded 80 times

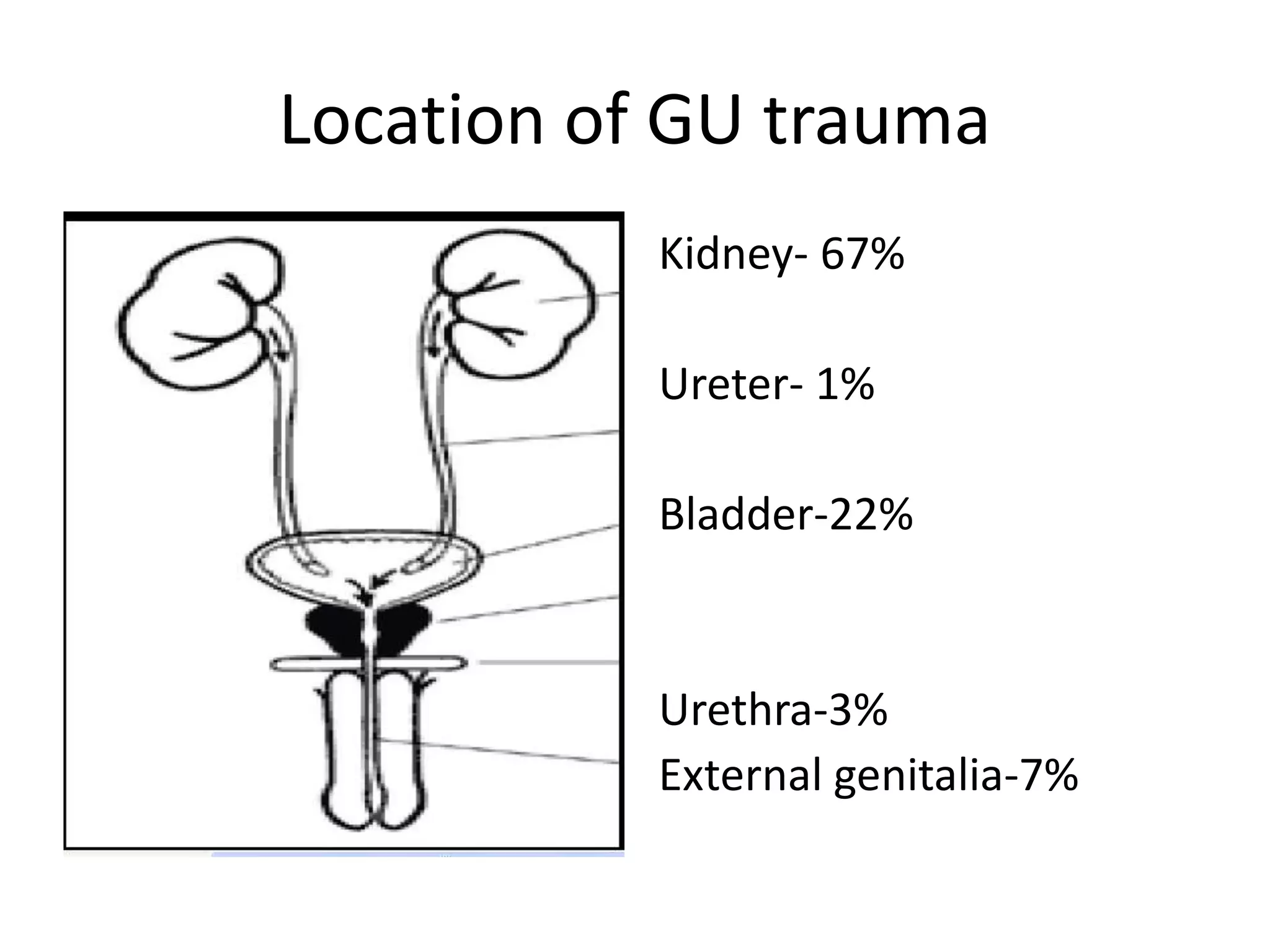

















































































This document discusses urinary tract trauma, focusing on kidney injuries. It notes that kidney injuries account for 67% of GU trauma and are usually blunt. CT scan is the preferred imaging modality. The Federle and AAST classification systems for renal injuries are described, grading injuries from I-V in severity. Grade I are minor injuries like contusions. Higher grades involve deeper lacerations, vascular injuries, and devascularized or shattered kidneys. CT findings for each grade are provided with examples. Other imaging modalities like ultrasound, IVU, and angiography are also discussed.