Downloaded 47 times


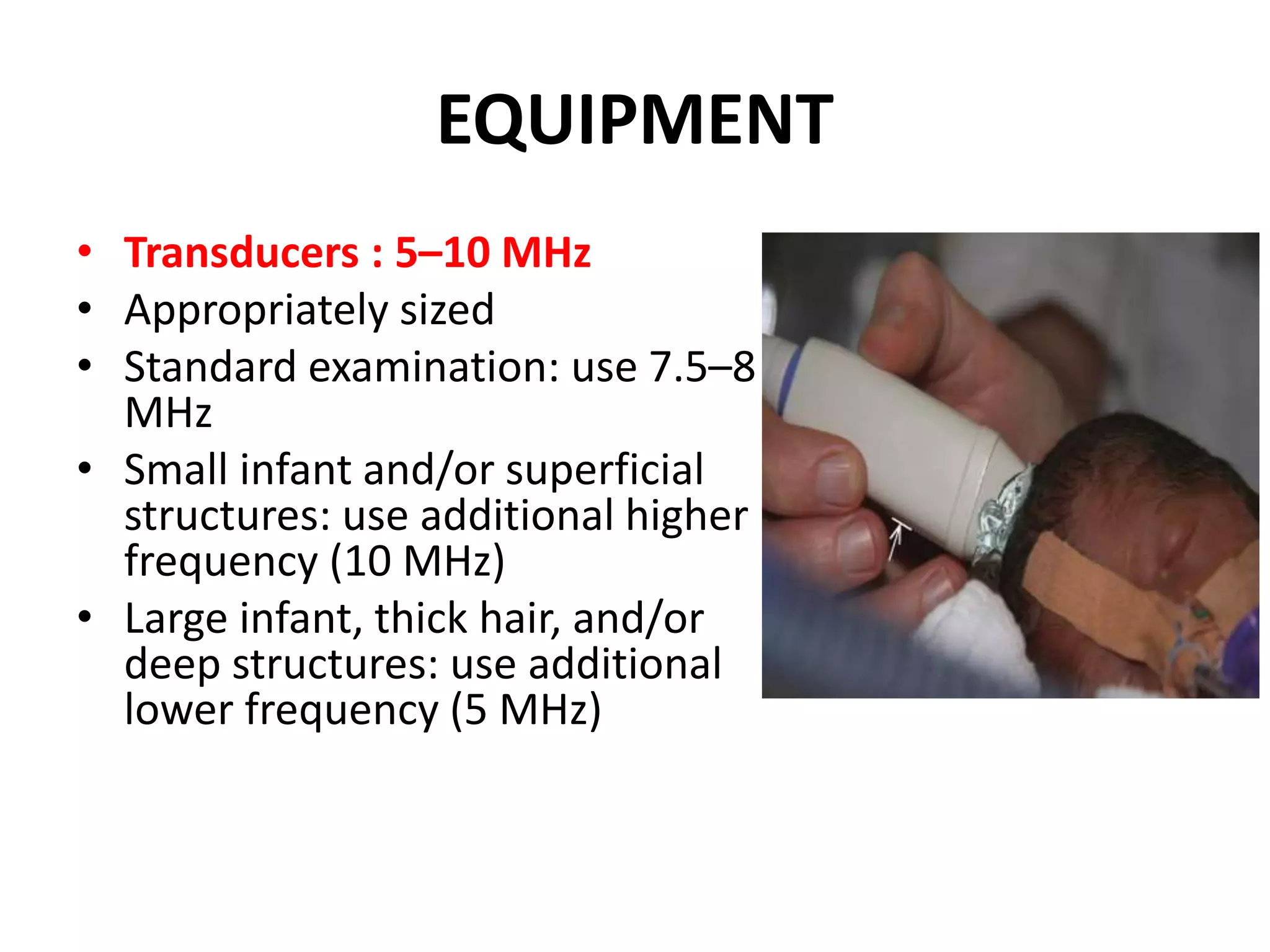
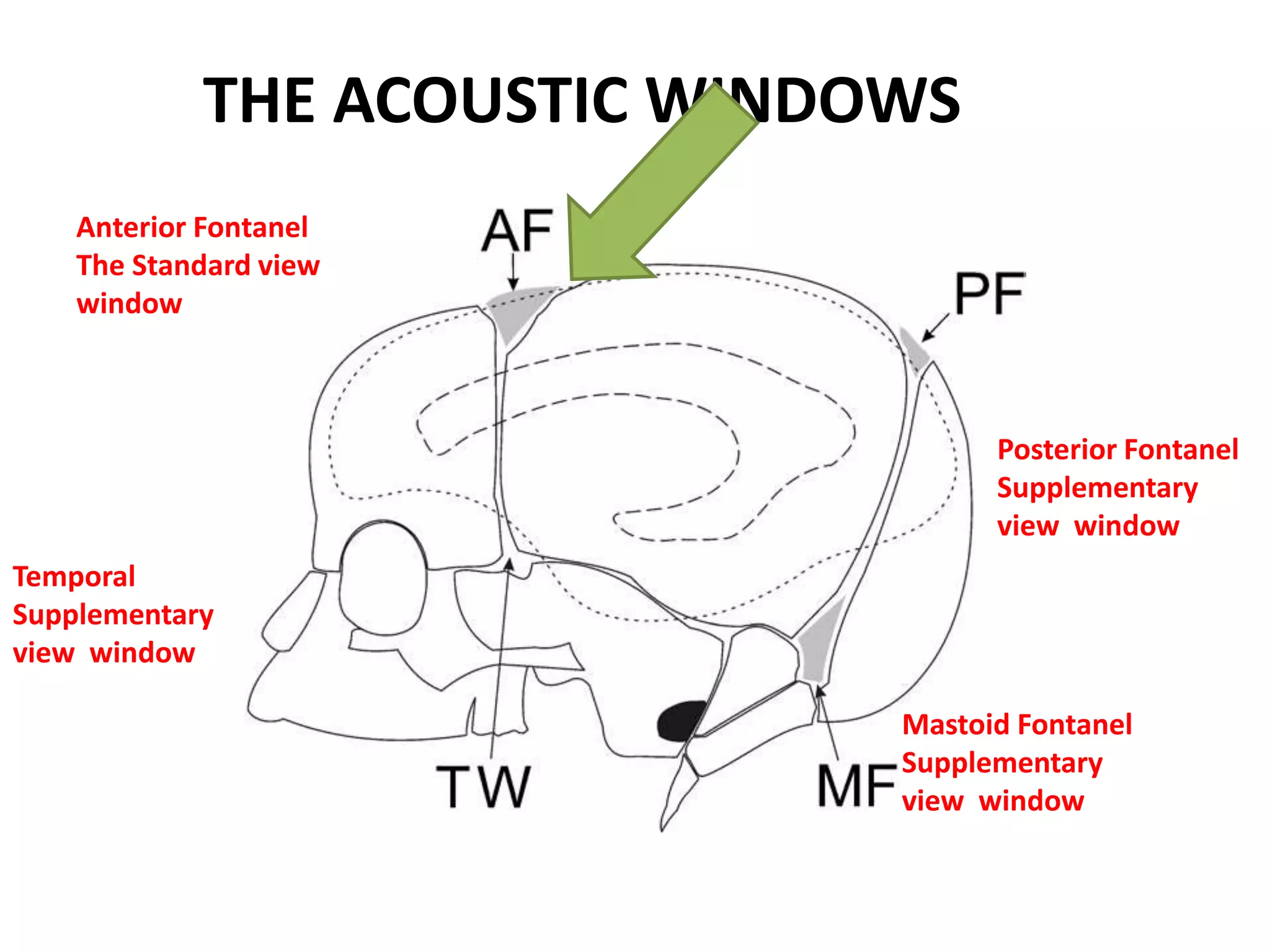

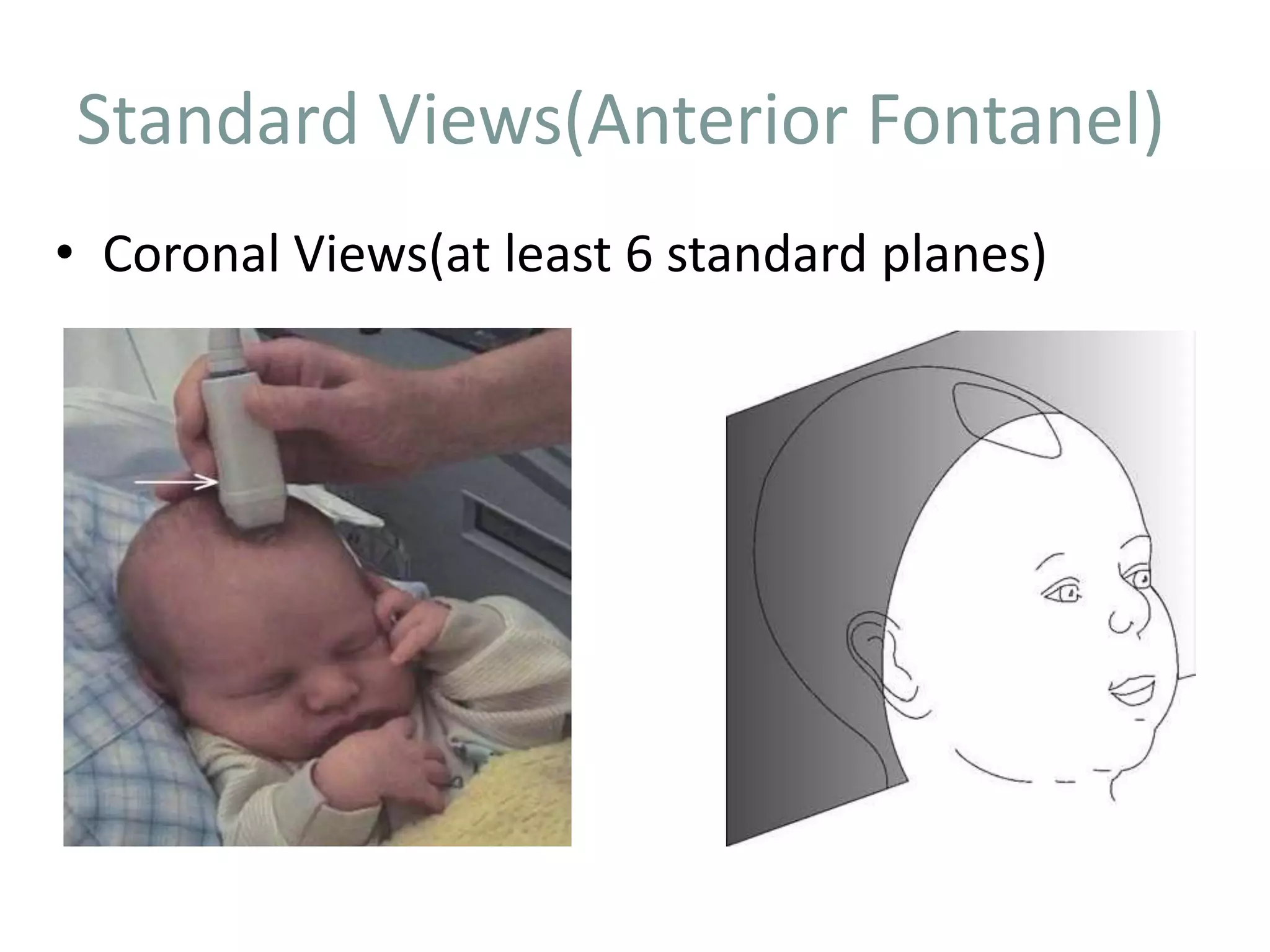
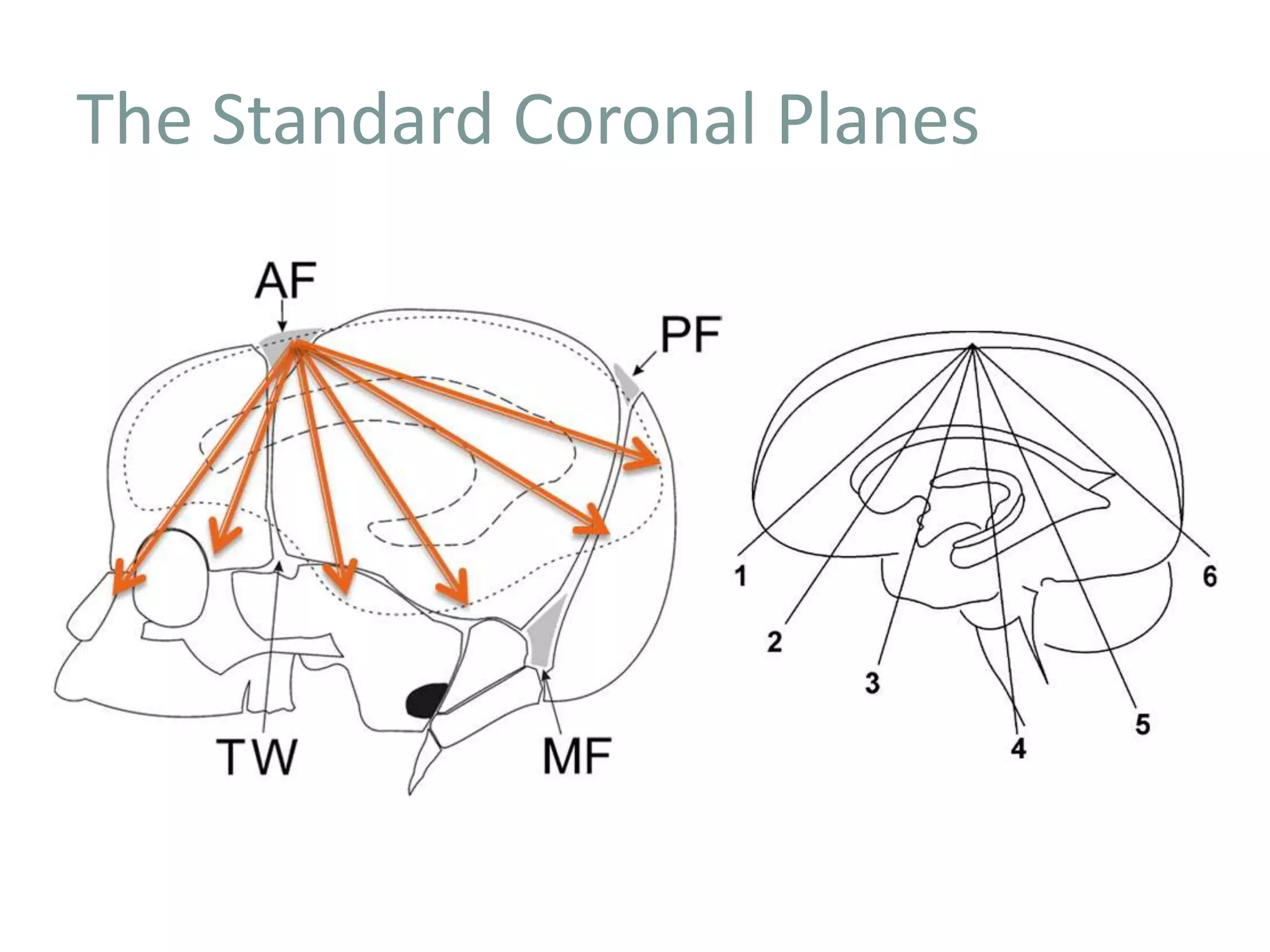





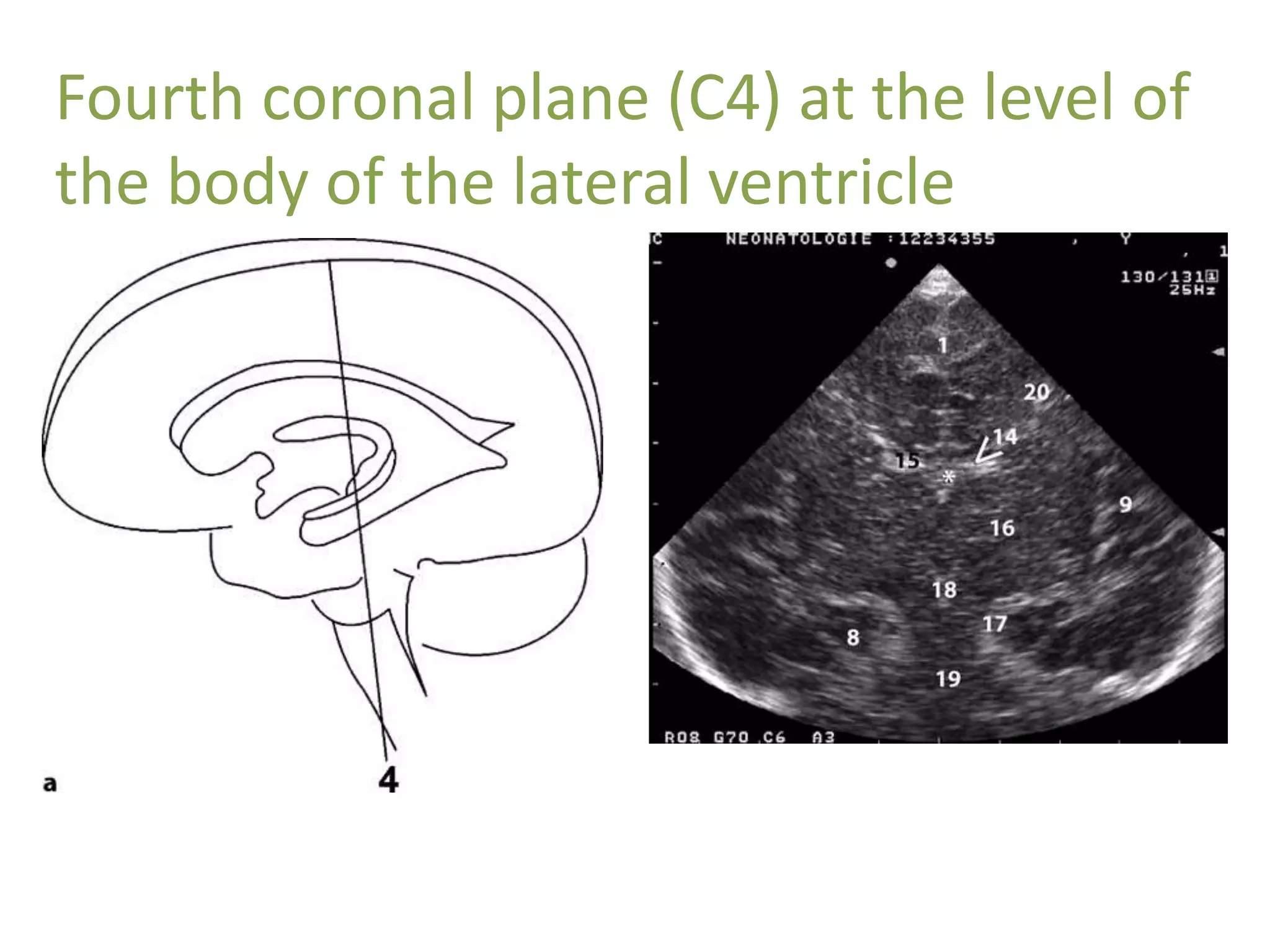


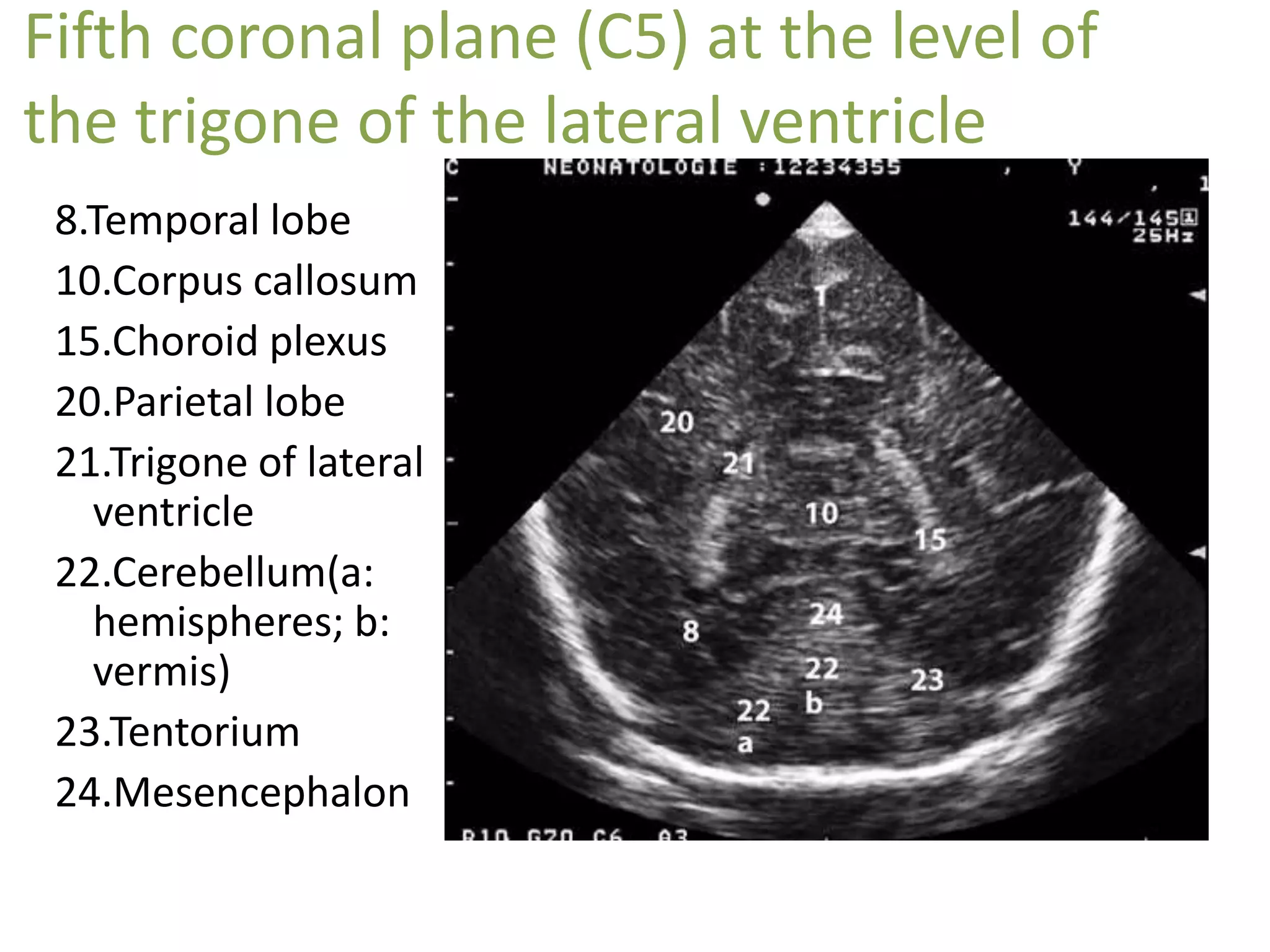



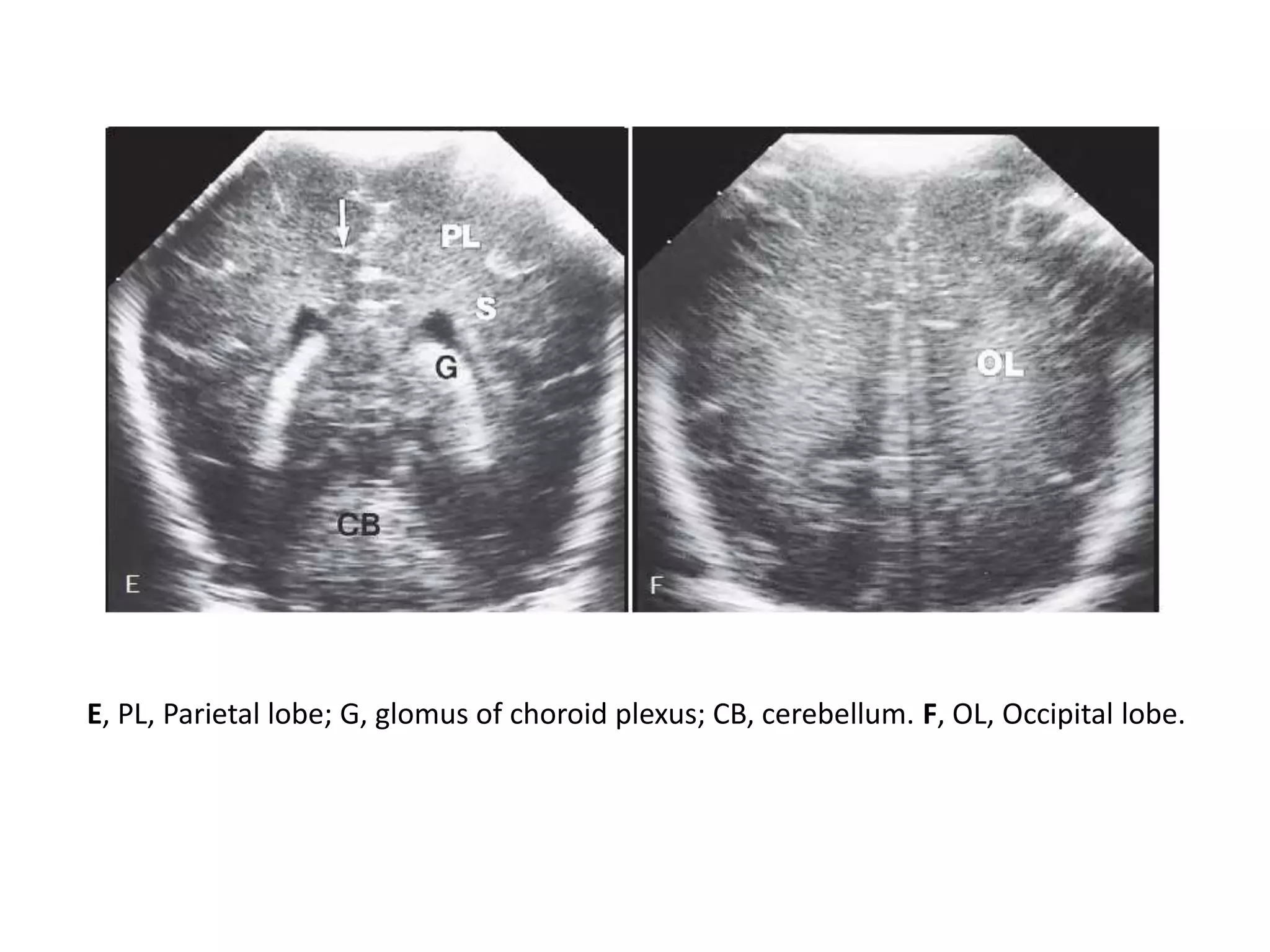


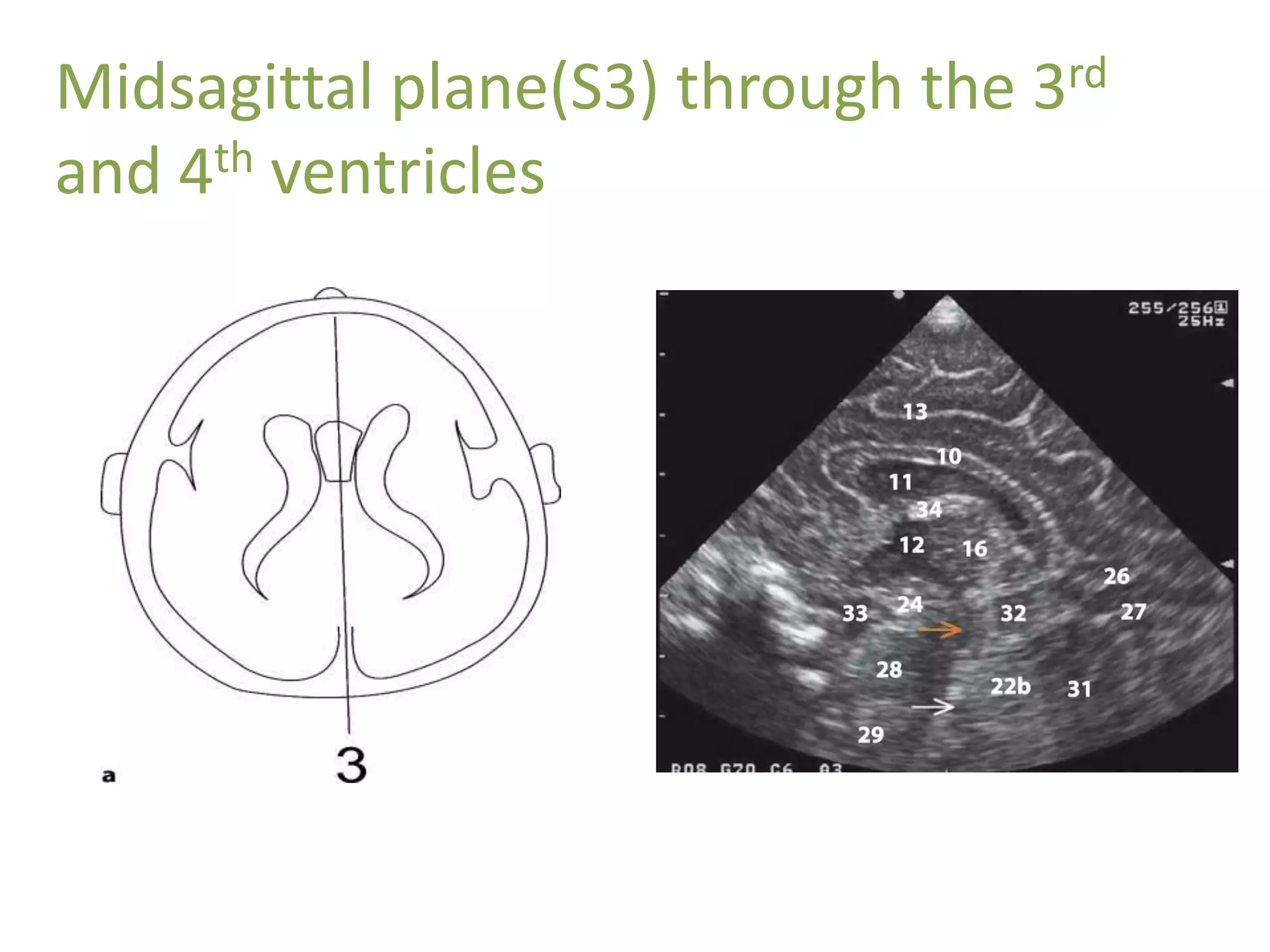



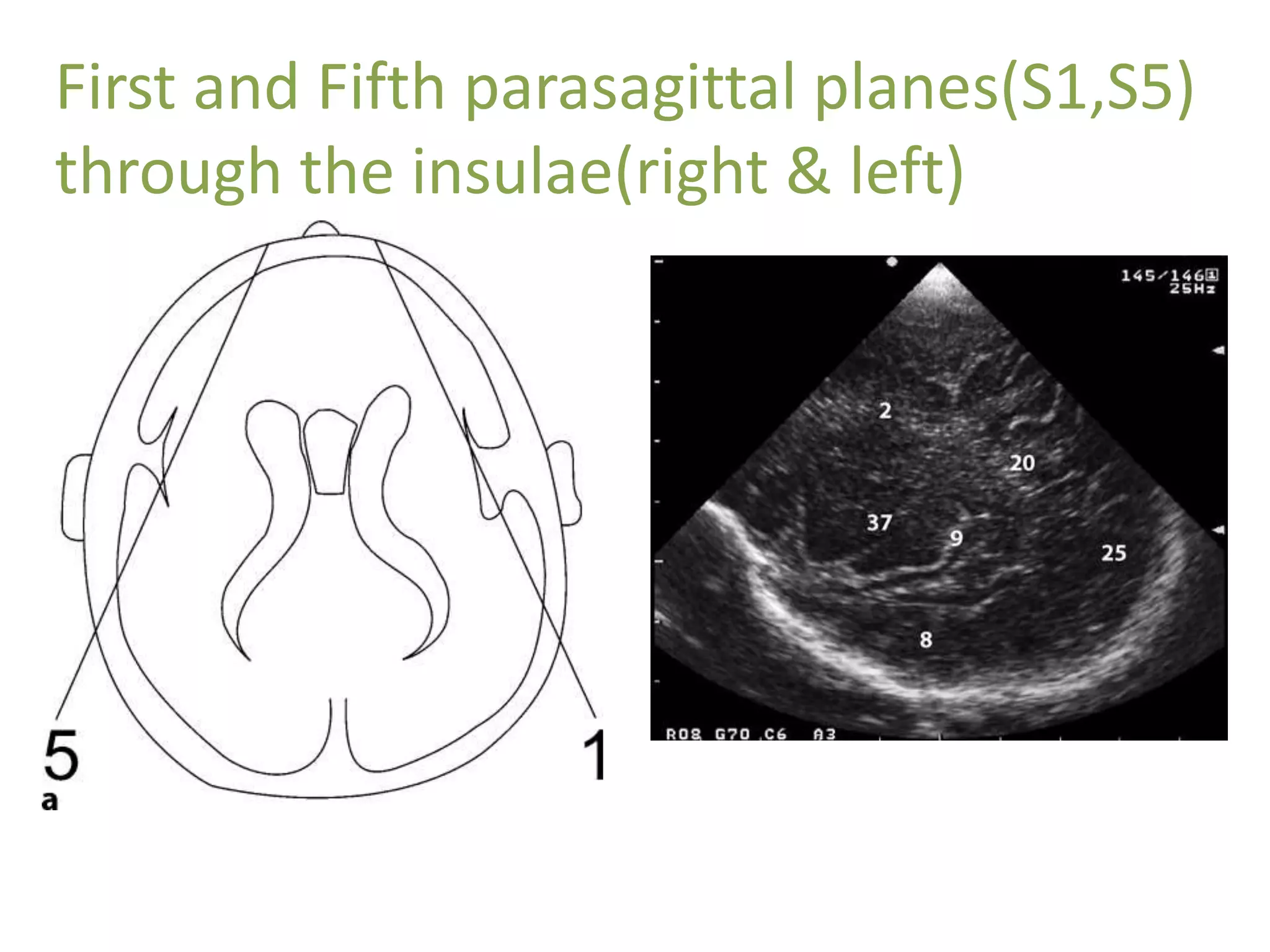

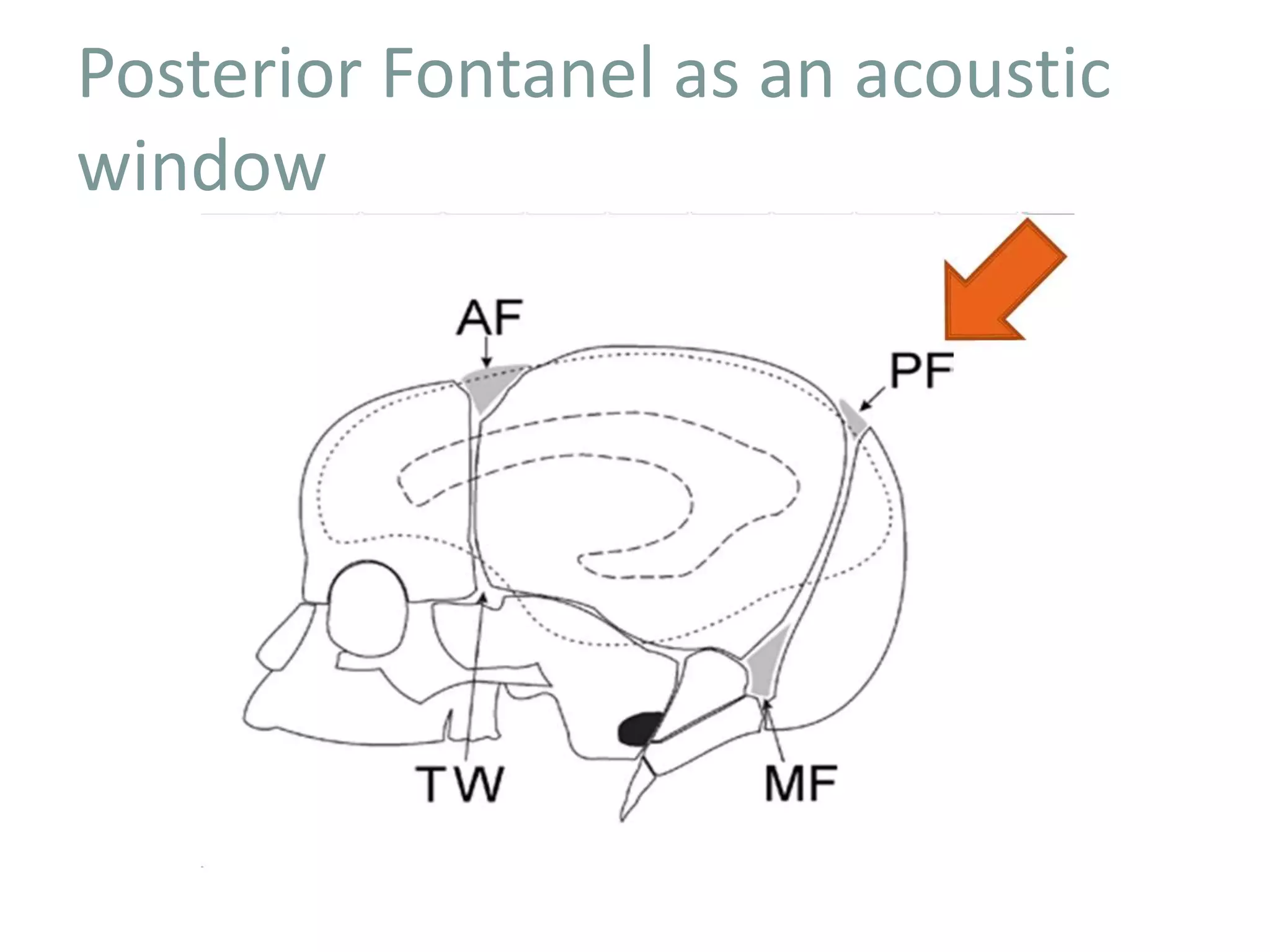
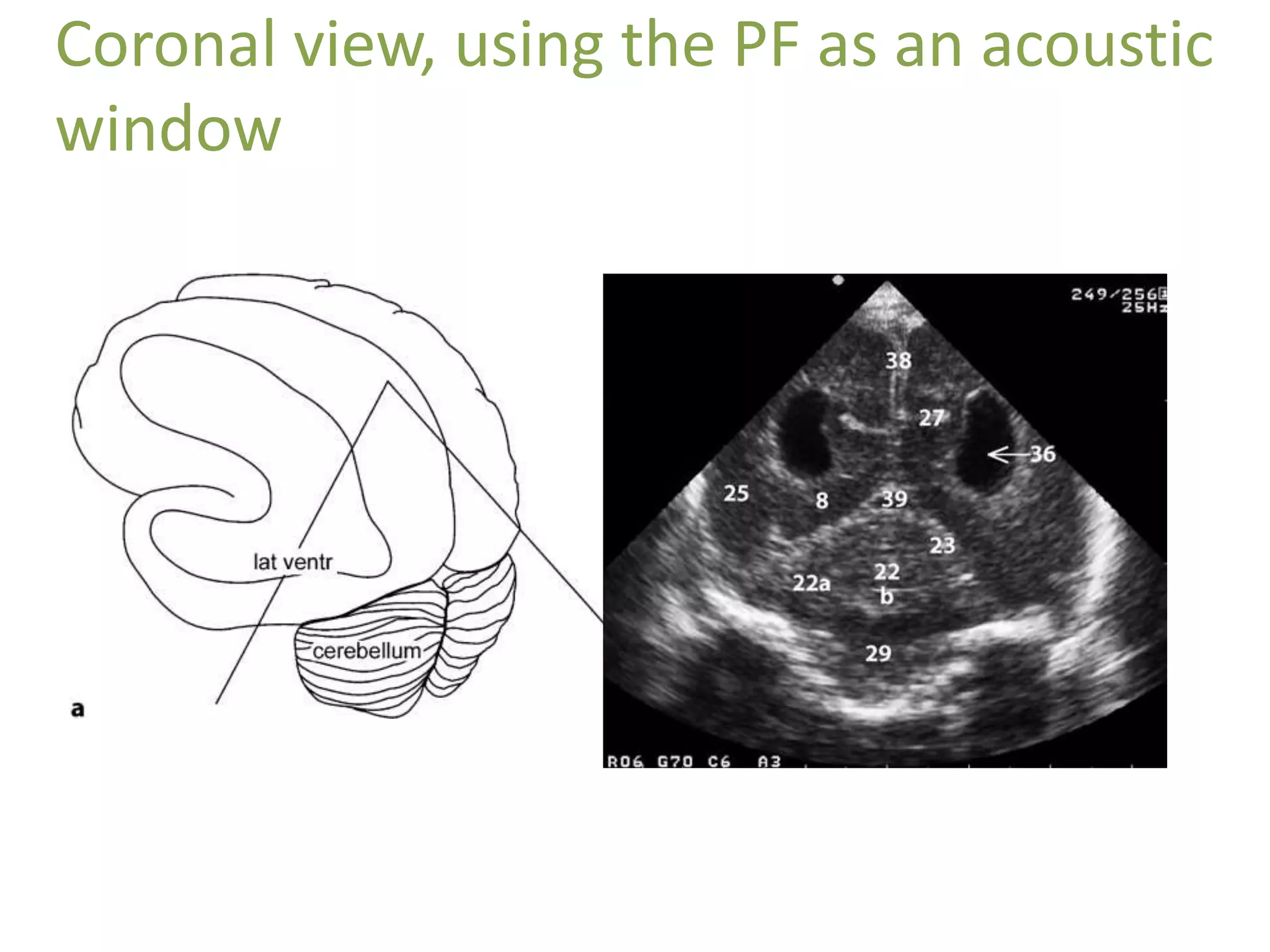



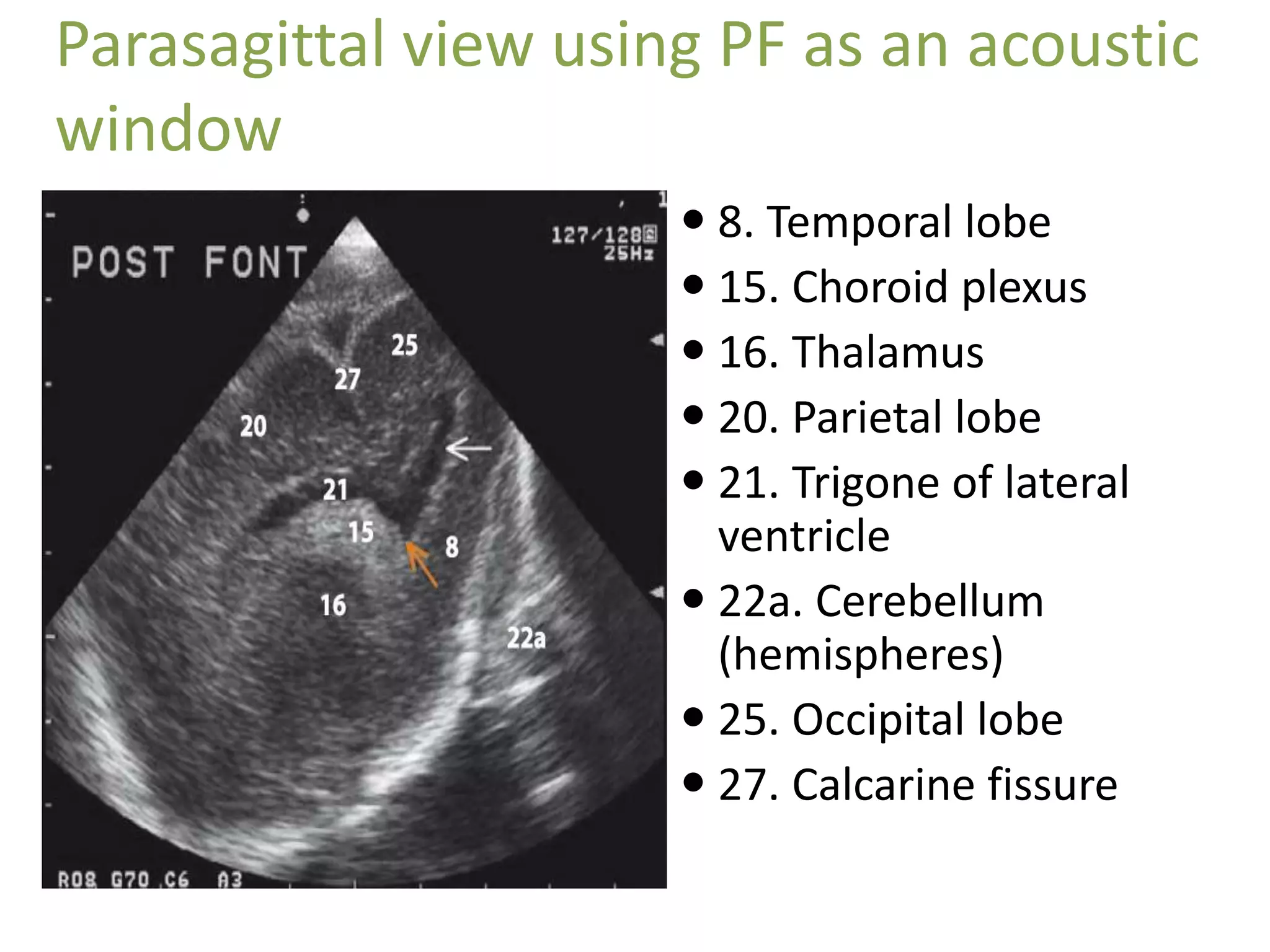
































Cranial sonography is an essential part of newborn care that allows for rapid evaluation of infants in the NICU with minimal risk. Standard brain ultrasound uses transducers of 5-10 MHz to obtain sagittal and coronal views through the anterior fontanelle, as well as views through the posterior and mastoid fontanelles. This provides evaluation of the brain structures and ventricles. Color Doppler may help differentiate certain lesions. Cranial ultrasound is a reliable, inexpensive and radiation-free method for serially imaging the brain in newborns.














































![NSG AND HIE [Autosaved].............pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nsgandhieautosaved-250908133023-52fc5444-thumbnail.jpg?width=640&height=640&fit=bounds)