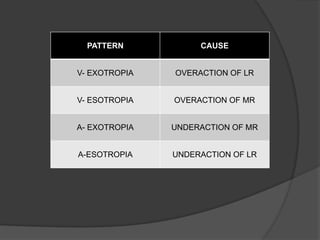
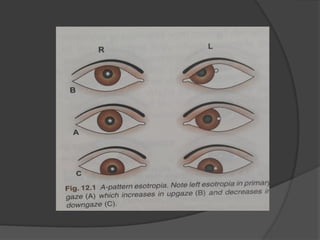
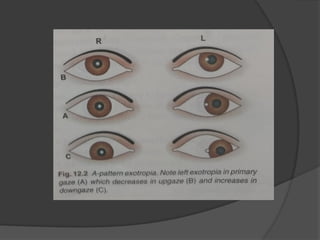
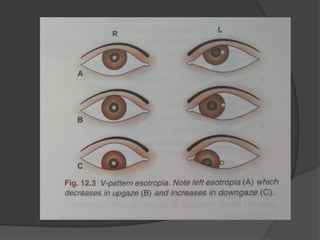
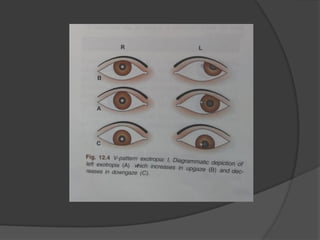
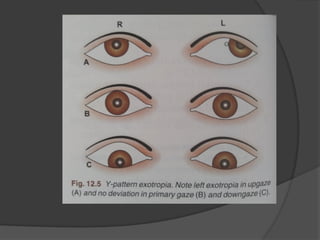
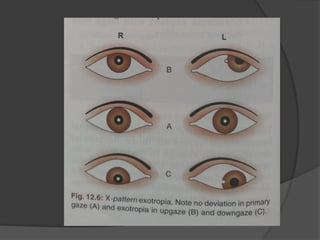
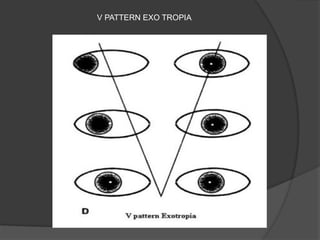
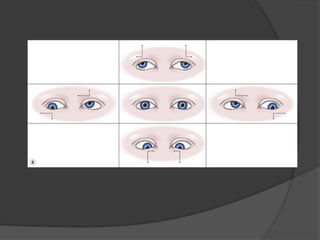
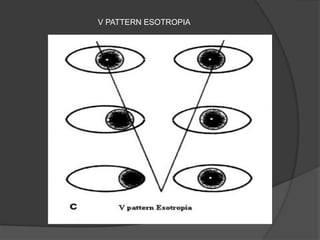
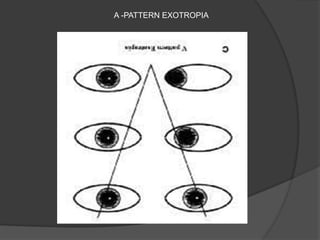
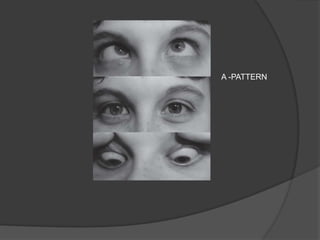
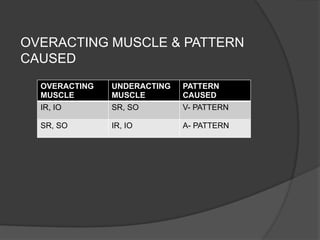
The document discusses different types of divergent strabismus (exotropia), including congenital, primary, sensory/secondary, and consecutive exotropia, detailing their characteristics, symptoms, and potential treatments. It emphasizes the importance of early diagnosis and intervention to prevent complications such as amblyopia, and it outlines various patterns of strabismus related to vertical gaze. Treatment options vary based on the type of exotropia and may include amblyopia therapy, surgical procedures, and vision therapy.