
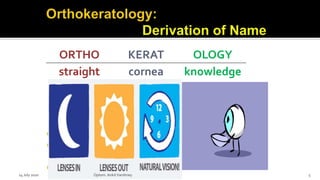
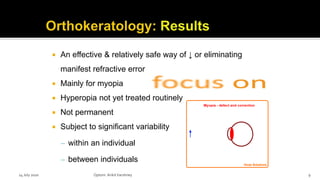

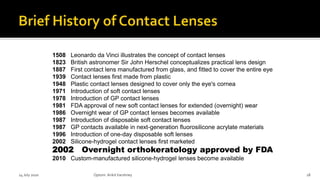
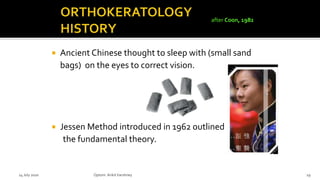
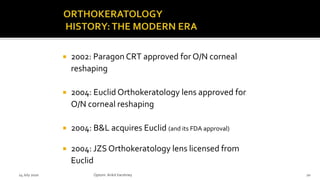
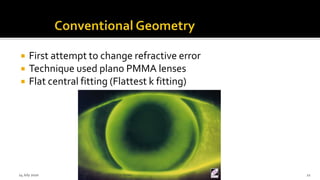




The document discusses orthokeratology (ortho-k), a non-surgical method for reshaping the cornea to reduce or eliminate refractive errors, particularly myopia. It covers the technology's advantages, such as being reversible and suitable for children, as well as potential disadvantages like variability in results and patient compliance issues. Additionally, the document outlines the fitting process, necessary patient evaluations, and the history of contact lens development related to ortho-k.


















































































