DEFINITION
• An exodeviationis a manifest (exotropia) or latent (exophoria) divergent strabismus.
• Simple words : Eye deviating outwards (away from nose).
• Could be :
a. constant (one eye)
b. Alternating (preference / no preference)
c. Mixed with vertical deviation
d. Associated with A orV pattern
2.
RISK FACTORS
Maternal substanceabuse , smoking during pregnancy
Premature birth
Perinatal morbidity
Genetic anomalies
Family history of strabismus
Uncorrected refractive errors.
PSEUDO-EXOTROPIA
• Appearance ofexodeviation when the eyes are actually aligned.
• May occur when there is a wide interpupillary distance or a positive
angle kappa with or without other ocular abnormalities.
5.
EXOPHORIA(X’)
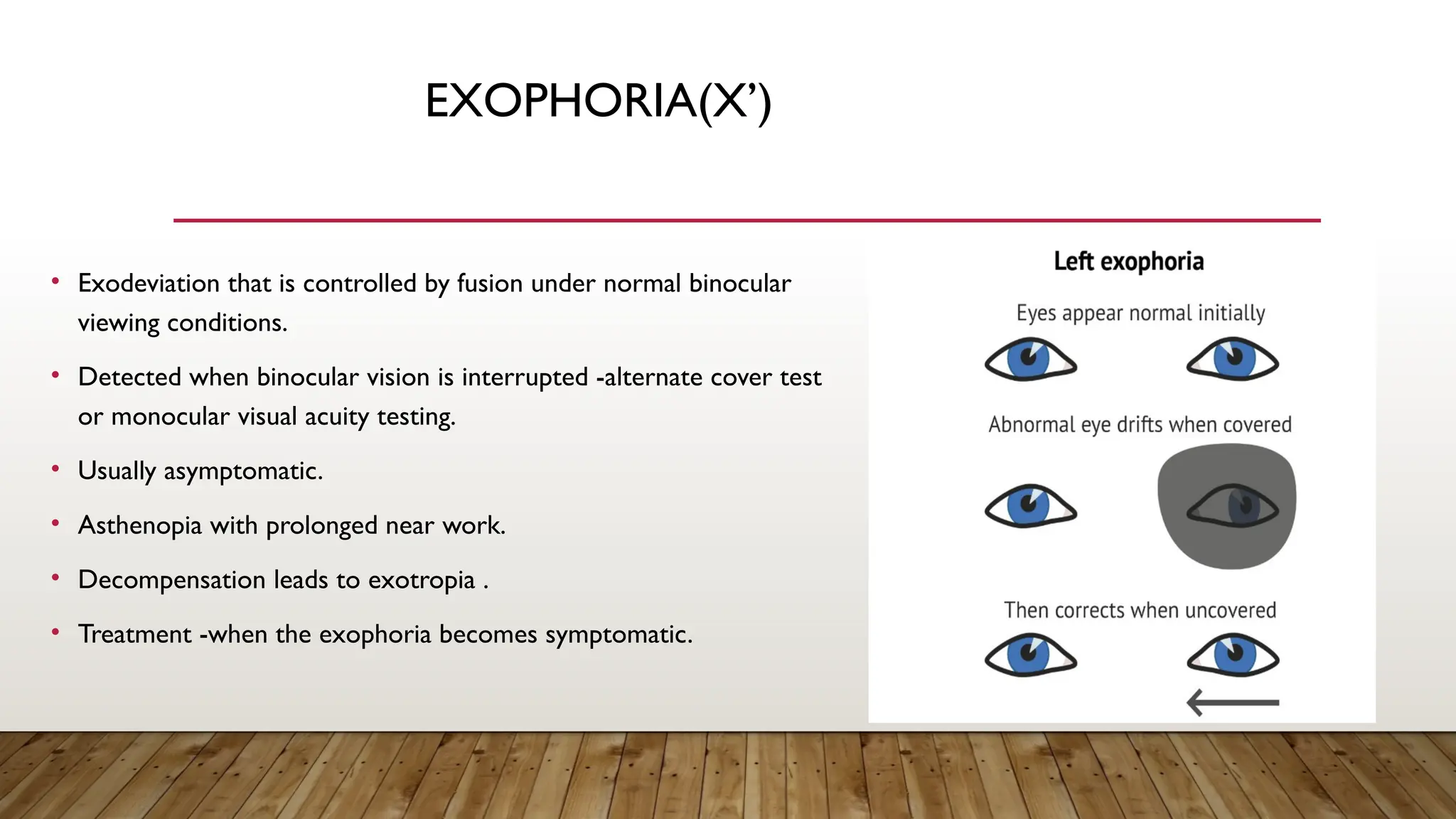
• Exodeviation thatis controlled by fusion under normal binocular
viewing conditions.
• Detected when binocular vision is interrupted -alternate cover test
or monocular visual acuity testing.
• Usually asymptomatic.
• Asthenopia with prolonged near work.
• Decompensation leads to exotropia .
• Treatment -when the exophoria becomes symptomatic.
6.
INTERMITTENT EXOTROPIA -X(T)
• Eye deviated outward but controlled by fusion/accommodation.
• Onset usually before 5 years.
• Manifest during times of visual inattention, fatigue, stress, or illness.
• Parents say that the exotropia occurs late in the day or when the child is daydreaming or tired.
• Usually larger when the patient views distant targets, and difficult to elicit at near fixation.
• May be associated with small hypertropias,A andV patterns, and overelevation and underelevation
in adduction
7.
CONSTANT EXOTROPIA
• Outwarddeviation is constant.
• Constant angle of deviation.
• Often seen in older patients with sensory exotropia or in patients with a history of long-
standing intermittent exotropia that has decompensated.
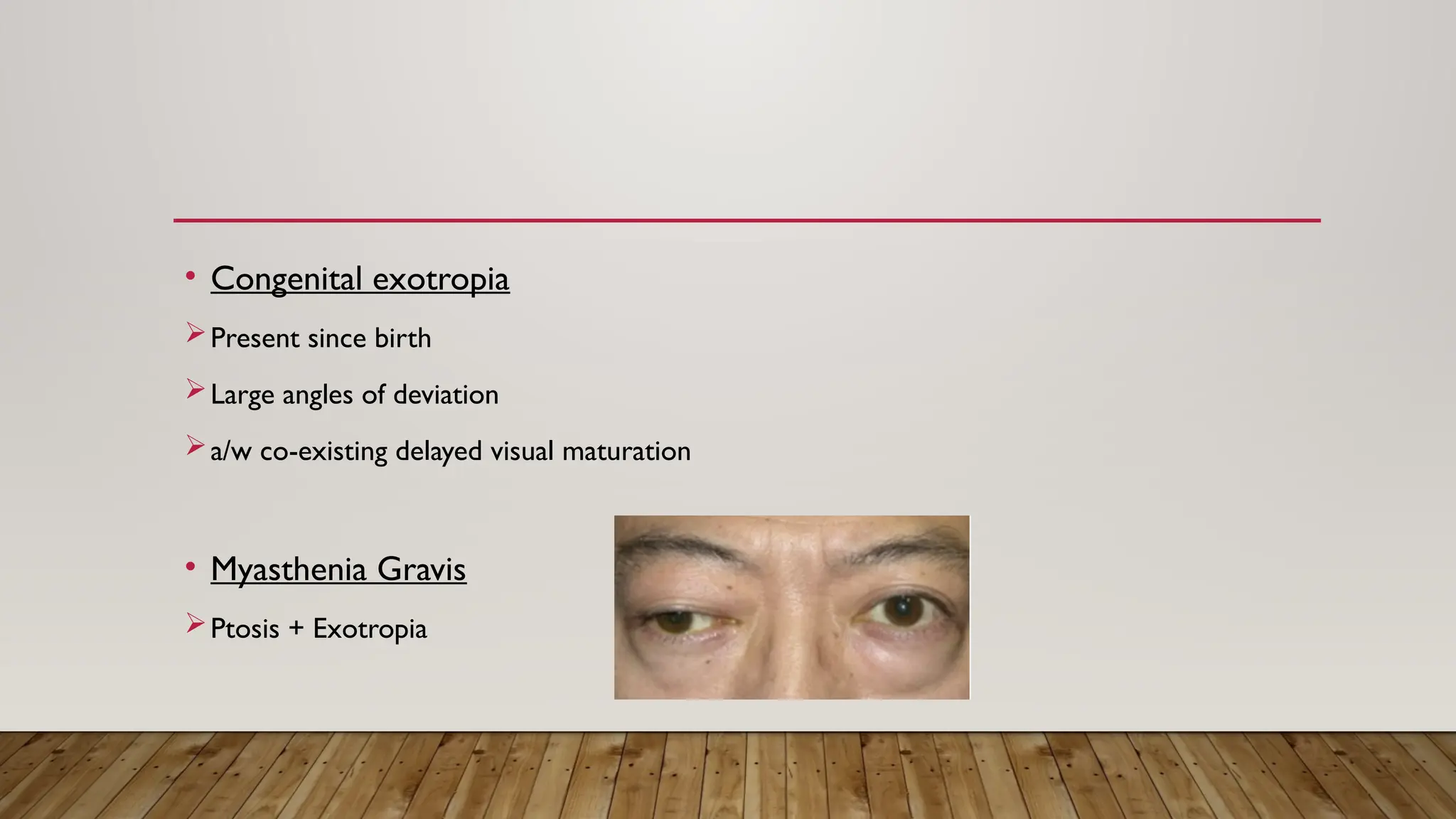
INFANTILE EXOTROPIA
• Infantileexotropia is much less common than
infantile esotropia.
• Onset before age 6 months as a large-angle
deviation .
• The risk of amblyopia is higher in constant
exotropia than in intermittent exotropia.
10.
WHY EXOTROPIA HAPPENS?
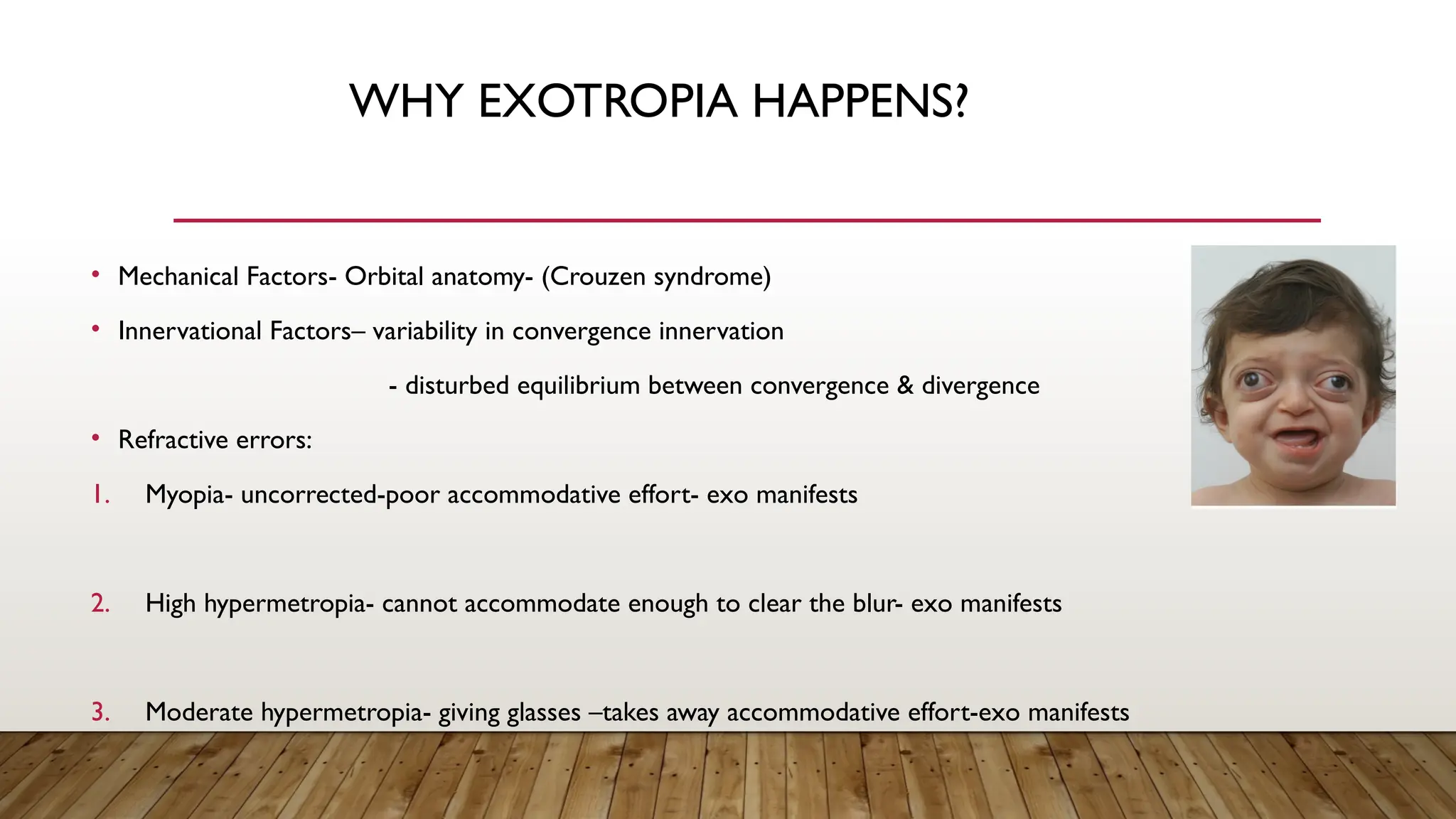
•Mechanical Factors- Orbital anatomy- (Crouzen syndrome)
• Innervational Factors– variability in convergence innervation
- disturbed equilibrium between convergence & divergence
• Refractive errors:
1. Myopia- uncorrected-poor accommodative effort- exo manifests
2. High hypermetropia- cannot accommodate enough to clear the blur- exo manifests
3. Moderate hypermetropia- giving glasses –takes away accommodative effort-exo manifests
11.
HISTORY
age at onset/ present
since birth? (less
stereopsis)
h/o prematurity—ROP?
Developmental delay?
Viral illness?
h/o vaccination , h/o
trauma , family history
frequency and duration of
misalignment
circumstances under which
the deviation is manifest
whether the exotropia is
becoming more frequent
with time.
symptoms such as
diplopia, asthenopia, or
difficulty with interpersonal
interactions secondary to
ocular misalignment are
present.
12.
EXAMINATION
• A typicalexamination order is:
1. Stereopsis (distance and near) - eg:Titmus fly test..
2. Duction andVersion
3. Exodeviation control
• Good: Exotropia manifests only after cover testing; the patient resumes fusion rapidly without blinking or refixating.
• Fair: Exotropia manifests after fusion is disrupted by cover testing; the patient resumes fusion only after blinking or refixating.
• Poor:Exotropia manifests spontaneously ,may remain manifest for an extended time.
4.Exodeviation angle
5.Visual acuity (monocular & binocular)
EXODEVIATION ANGLE
• Prismand alternate cover testing is used to evaluate the exodeviation at
fixation distances of 6 m and 33 cm.
• A far-distance measurement at 30 m or greater (eg, at the end of a long
hallway or out a window) may uncover a latent deviation or elicit an even
larger one.
16.
OTHER THINGSTO KEEPIN MIND DURING
EXAMINATION
Amblyopia
Distance near disparity
Co-existing A/V pattern
Refractive correction
Media and Fundus
17.
DUANE’S CLASSIFICATION
1. Divergenceexcess pattern : Distance deviation 15 Prism dioptres (PD) larger than near deviation.
2. Convergence insufficiency pattern : Near deviation 15 PD larger than distance deviation.
3. Basic exodeviation : Exodeviation equal for near and far distance ( usually within 10 PD).
4. Simulated divergence excess/ Pseudo divergence excess : type of basic deviation presenting as divergence
excess due to part compensation of near deviation by fusional or accommodative convergence.
IMPLEMENTATION
1) Near=30XT ,Distance=30XT
Dx-Basic XT
2) Near=20XT , Distance=40XT
?Divergence excess
Do a patch test (45min occlusion)
3) Near=35XT , Distance=40XT
Dx=Divergence excess with Tenacious proximal fusion
Fusion used to keep near deviation in check
20.
4) Near=20XT ,Distance=40XT
Patch test
Near=20XT , Distance=40XT
AC/A ratio (Hold up +3.00DS lens)
Near=35XT , Distance=40XT
Dx-Simulated Divergence excess with high AC/A ratio
5) Near=10XT , Distance=35XT
After patch test and AC/A ratio with +3.00DS lens
Same measurements
Dx- True divergence excess
6) Near=45XT , Distance=20XT
Dx- Convergence insufficiency
21.
SYMPTOMS
• Exophoria– Diplopia,Visual disturbances , Eyestrain , Headache (d/t constantly trying to fuse)
• Intermittent exotropia : precipitates on exposure to strong light
may lead to decreased vision when both eyes open
sometimes micropsia
• Constant exotropia : lack binocular vision
have wide peripheral vision
22.
OTHER FORMS OFEXOTROPIA
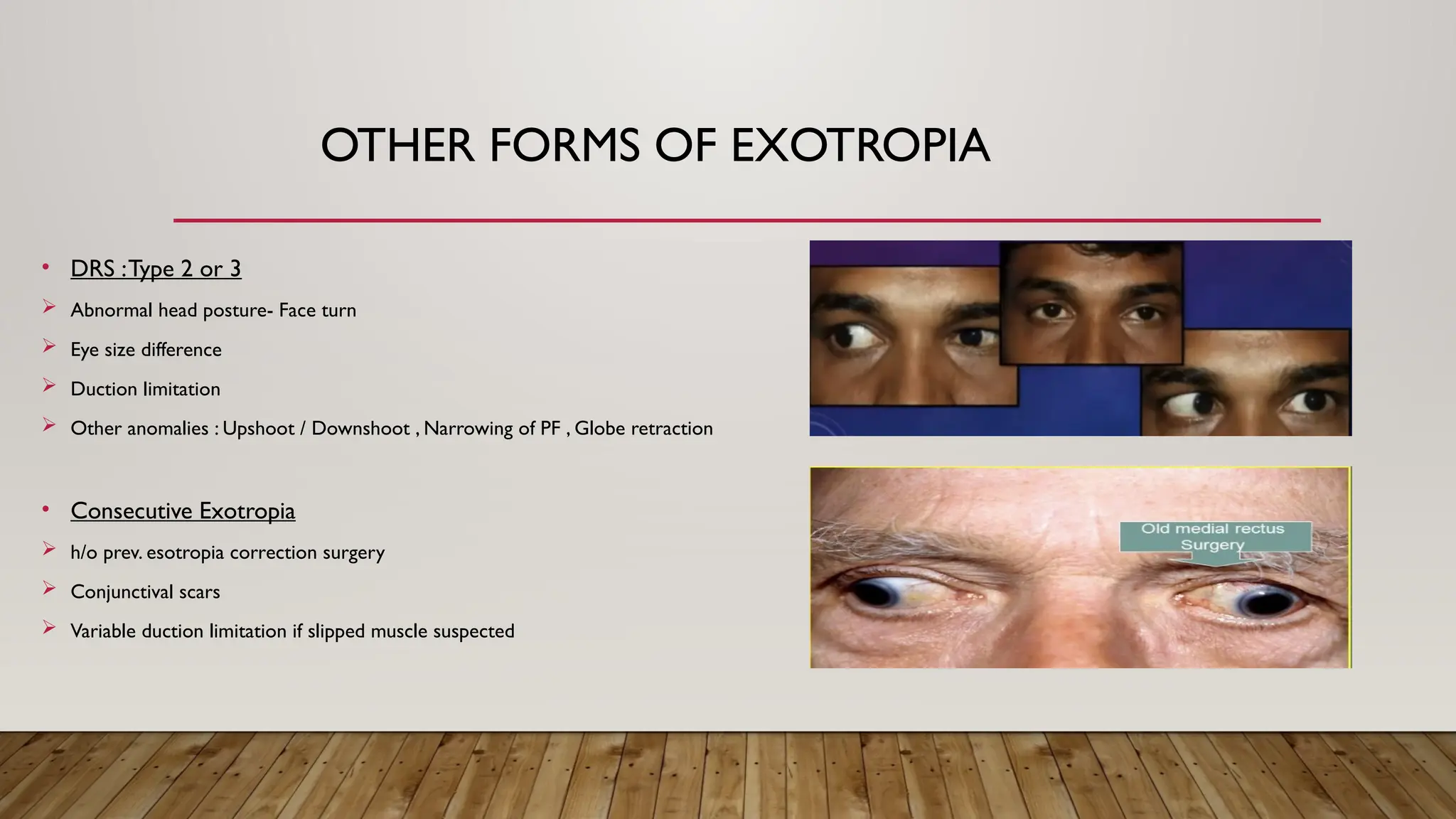
• DRS :Type 2 or 3
Abnormal head posture- Face turn
Eye size difference
Duction limitation
Other anomalies : Upshoot / Downshoot , Narrowing of PF , Globe retraction
• Consecutive Exotropia
h/o prev. esotropia correction surgery
Conjunctival scars
Variable duction limitation if slipped muscle suspected
23.
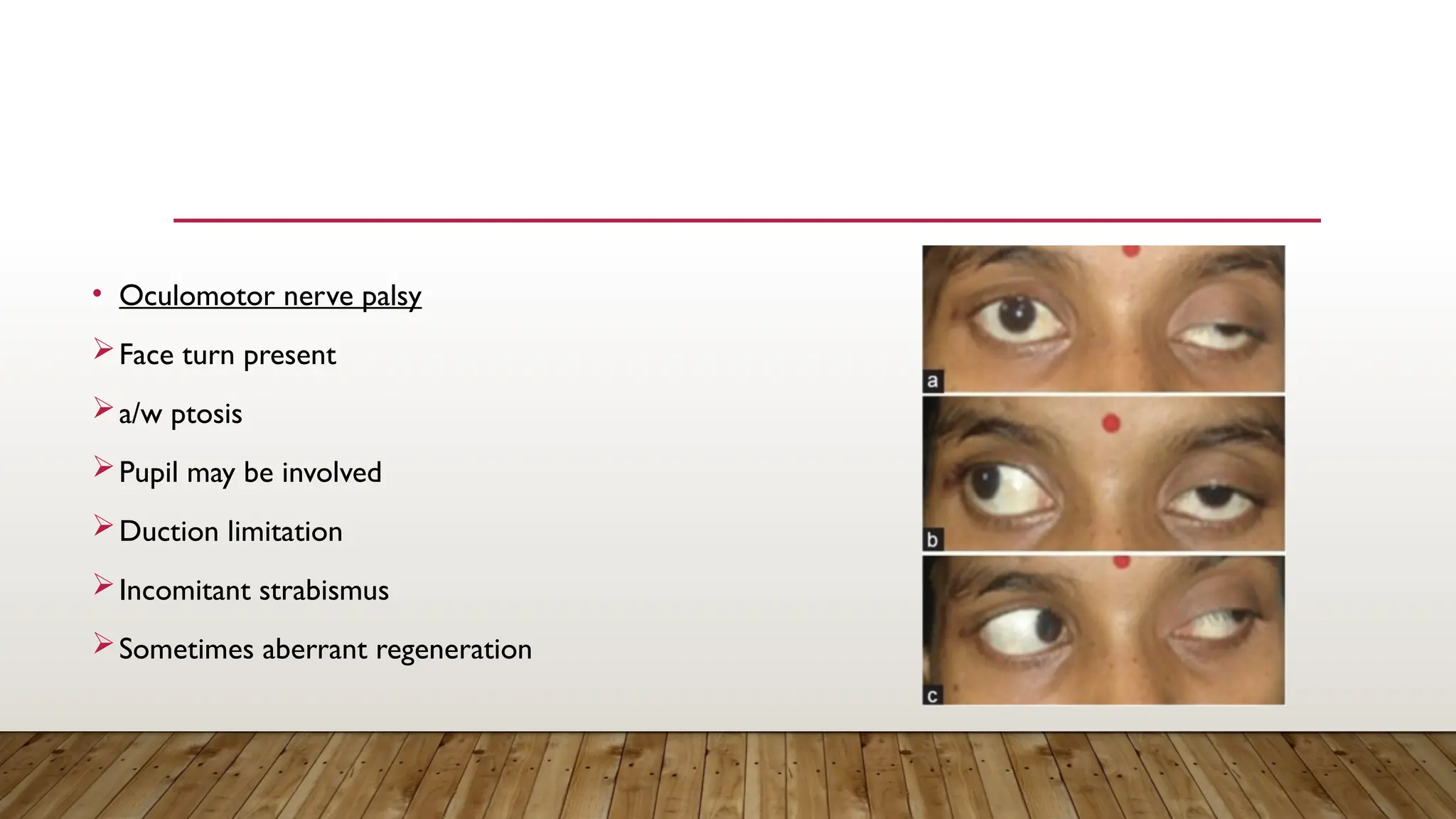
• Oculomotor nervepalsy
Face turn present
a/w ptosis
Pupil may be involved
Duction limitation
Incomitant strabismus
Sometimes aberrant regeneration
NON-SURGICAL
• Glass correction:
1.Uncorrected myopia- give full myopic correction
2. Astigmatism – full astigmatic correction in children
maximum tolerated correction in older children & adults
3. Hypermetropia – appropriate under-correction may improve control because of clear retinal
image
27.
OCCLUSIONTHERAPY
• Occlusion therapy(patching) for amblyopia may improve exotropic deviations.
• For patients without amblyopia, part-time patching of the dominant (nondeviating) eye or alternate
patching (alternating which eye is patched each day) in the absence of a strong ocular preference
can improve control of small- to moderate-sized deviations
• The improvement is often temporary, however, and many patients eventually require surgery.
28.
• Base Inprisms can be used, but not longterm – as causes reduced fusional vergence
• Orthoptic exercises : Treatment of symptomatic CI involves orthoptic exercises such as
stereograms,“pencil push-ups,” and computer-based or office-based convergence training
programs.
29.
SURGICALTREATMENT
• Factors influencingto proceed with surgery :
a. strabismus that is frequently manifest
b. poorly controlled
c. worsening (especially at near)
d. Symptomatic-decreased stereoacuity in the distance before near
e. poor self-image and difficulty with personal or professional relationships.
30.
• Surgical treatmentconsists of bilateral lateral rectus muscle recession or unilateral lateral rectus muscle
recession combined with medial rectus muscle resection.
• Large (>50 )
Δ deviations may require surgery on 3 or 4 muscles .
• Caution is advised when surgery is considered for a patient with true divergence excess exotropia, especially
with a high AC/A ratio, because of the associated risk of postoperative diplopia and esotropia at near.
31.
POST-OPERATIVE ALIGNMENT
• small-angleesotropia in the immediate postoperative period tends to resolve and is desirable because of its
association with a reduced risk of recurrent exotropia and higher success rates.
• Patients may experience diplopia.
• Postsurgical esotropia (unresolved) may require further treatment, such as hyperopic correction, base-out prisms,
patching to prevent amblyopia, or additional surgery.
• Bifocal glasses can be used in patients with a high AC/A ratio and should be discussed preoperatively with these
patients.