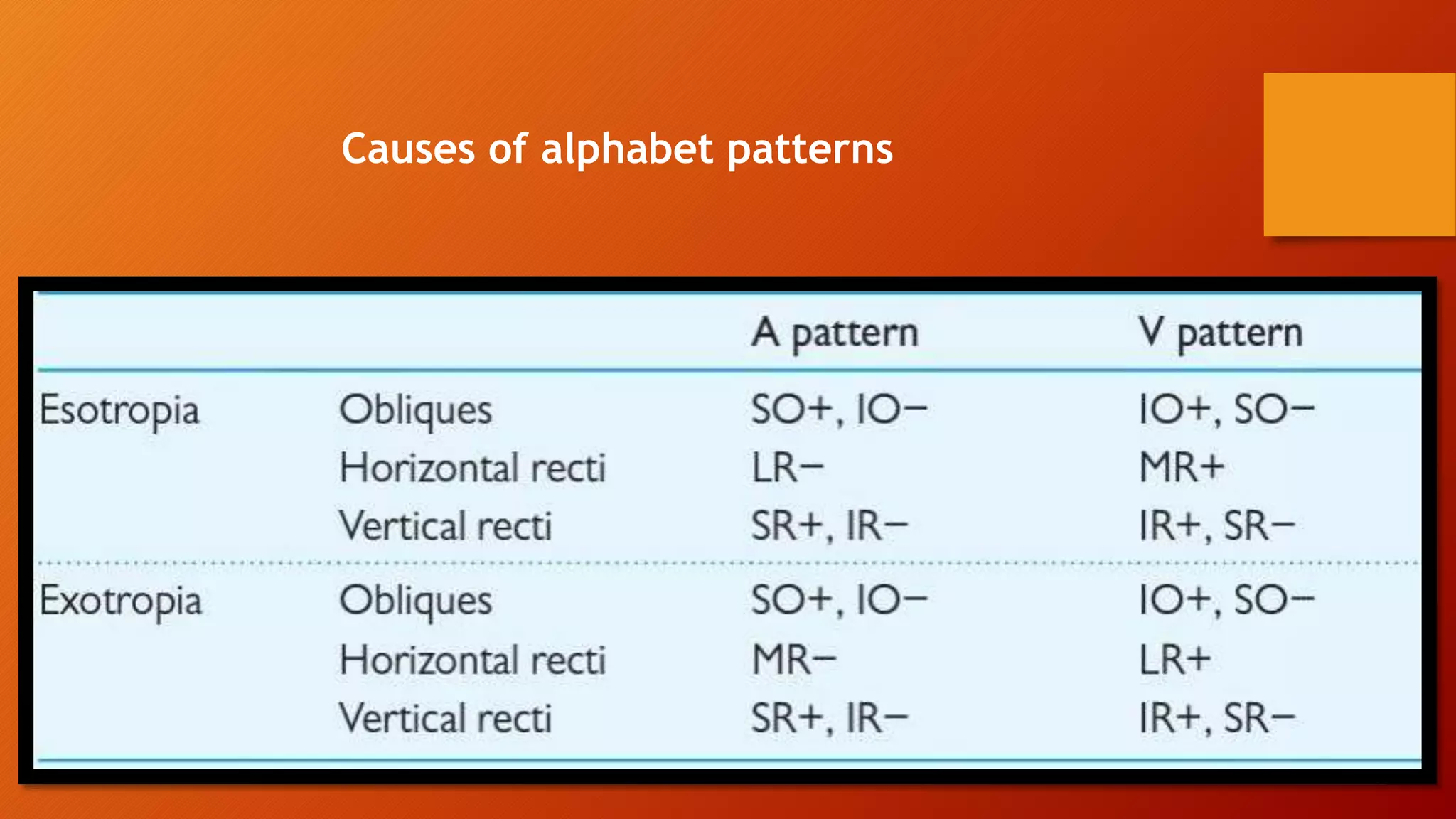
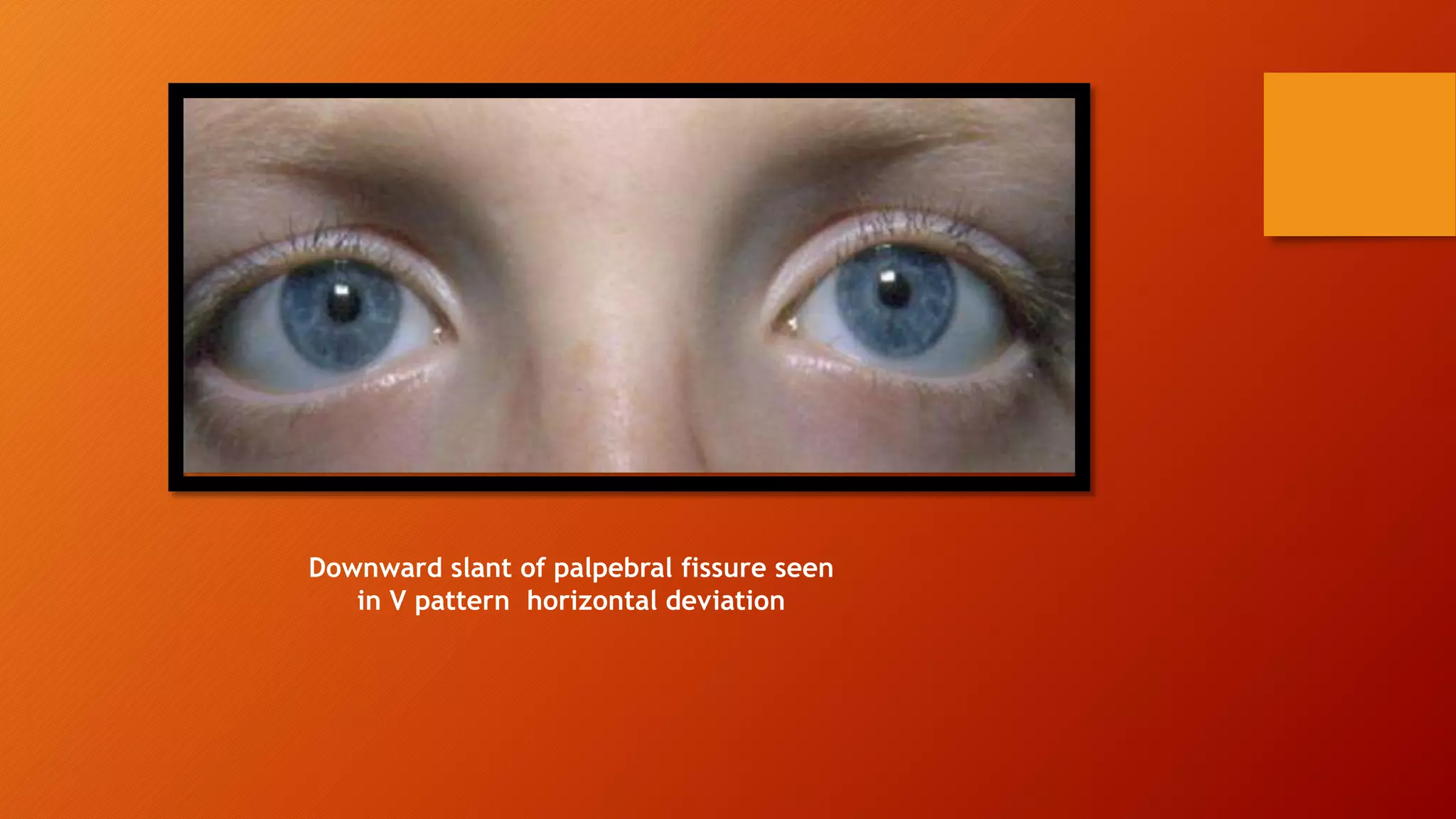
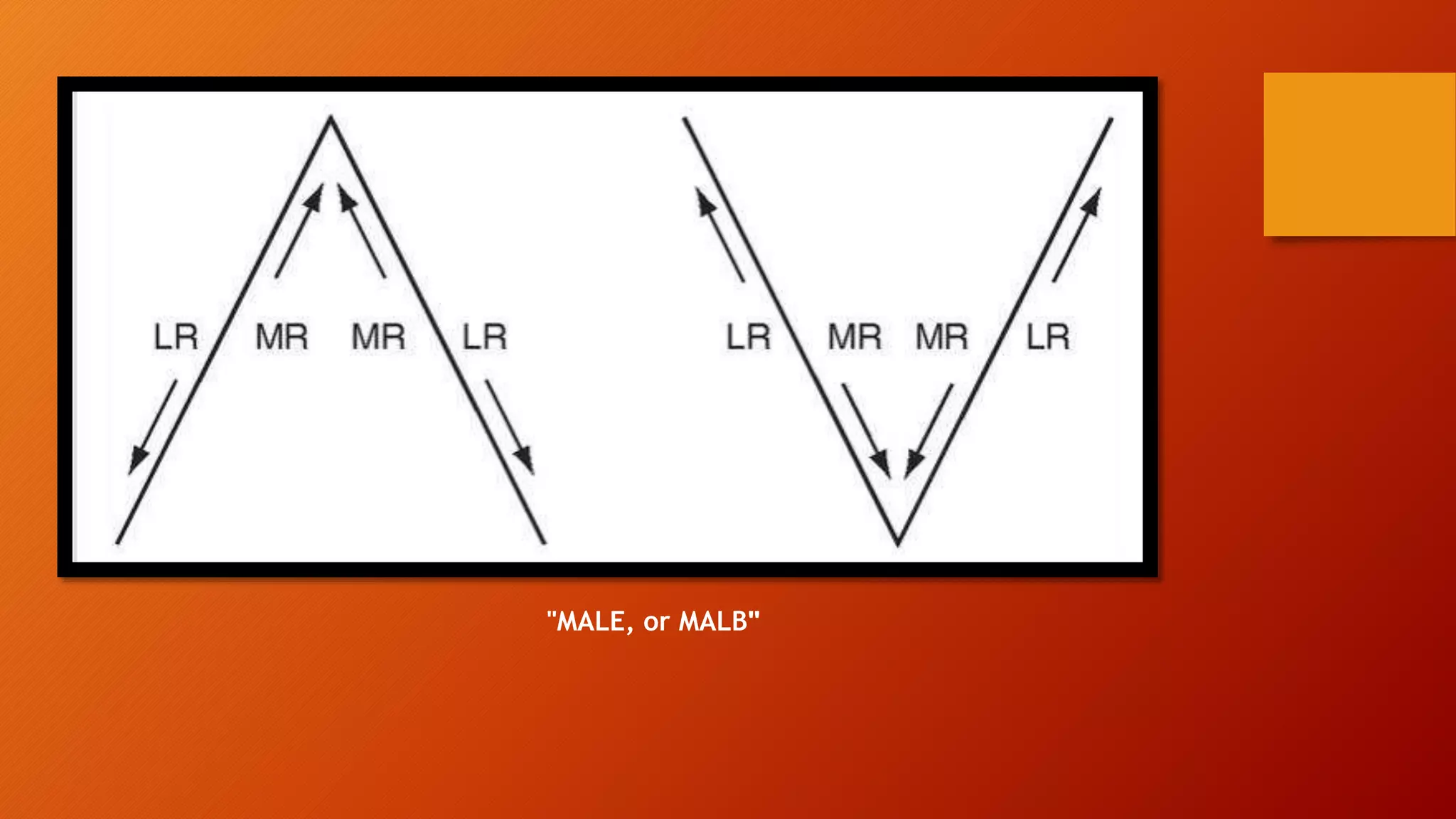
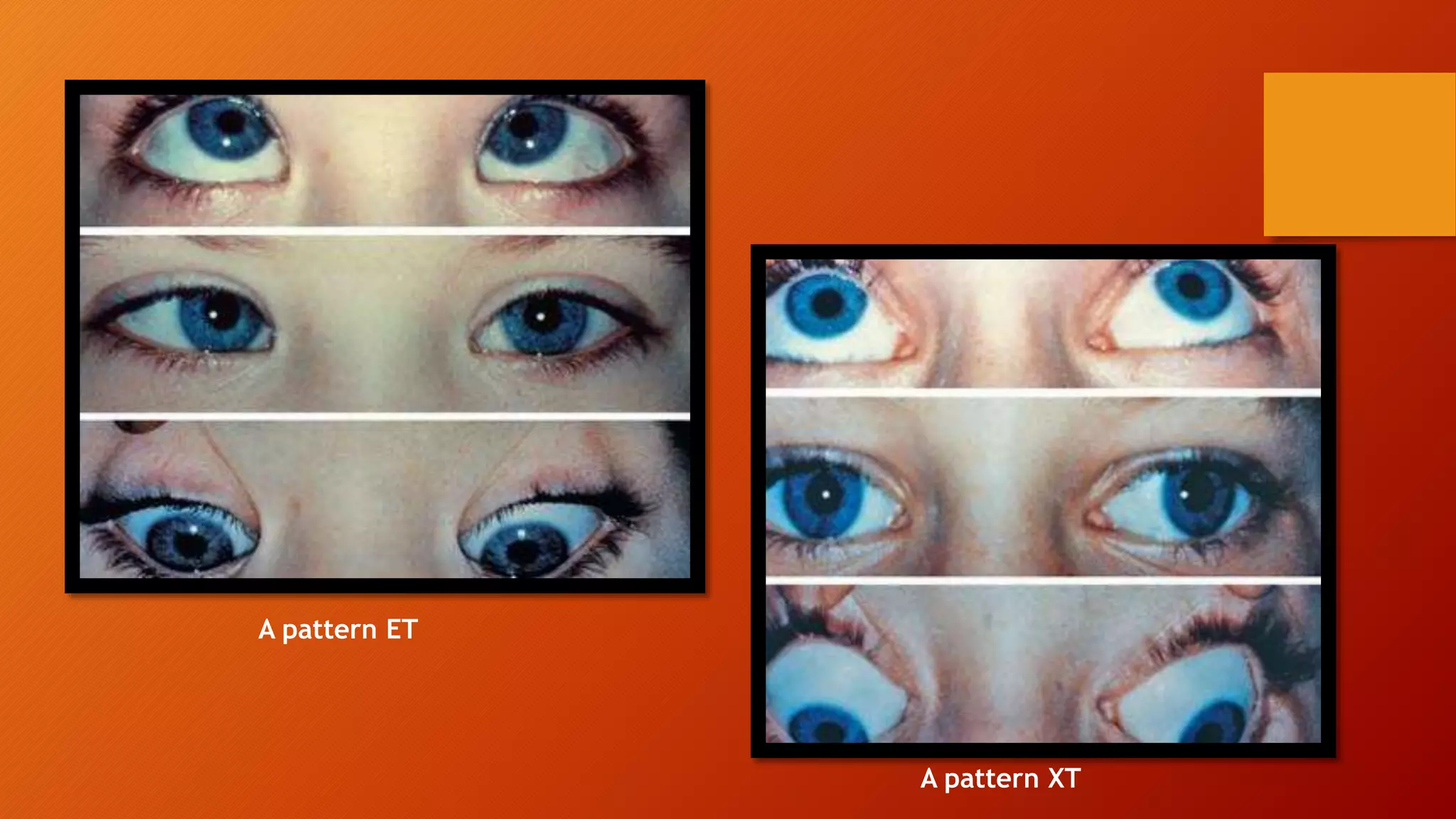
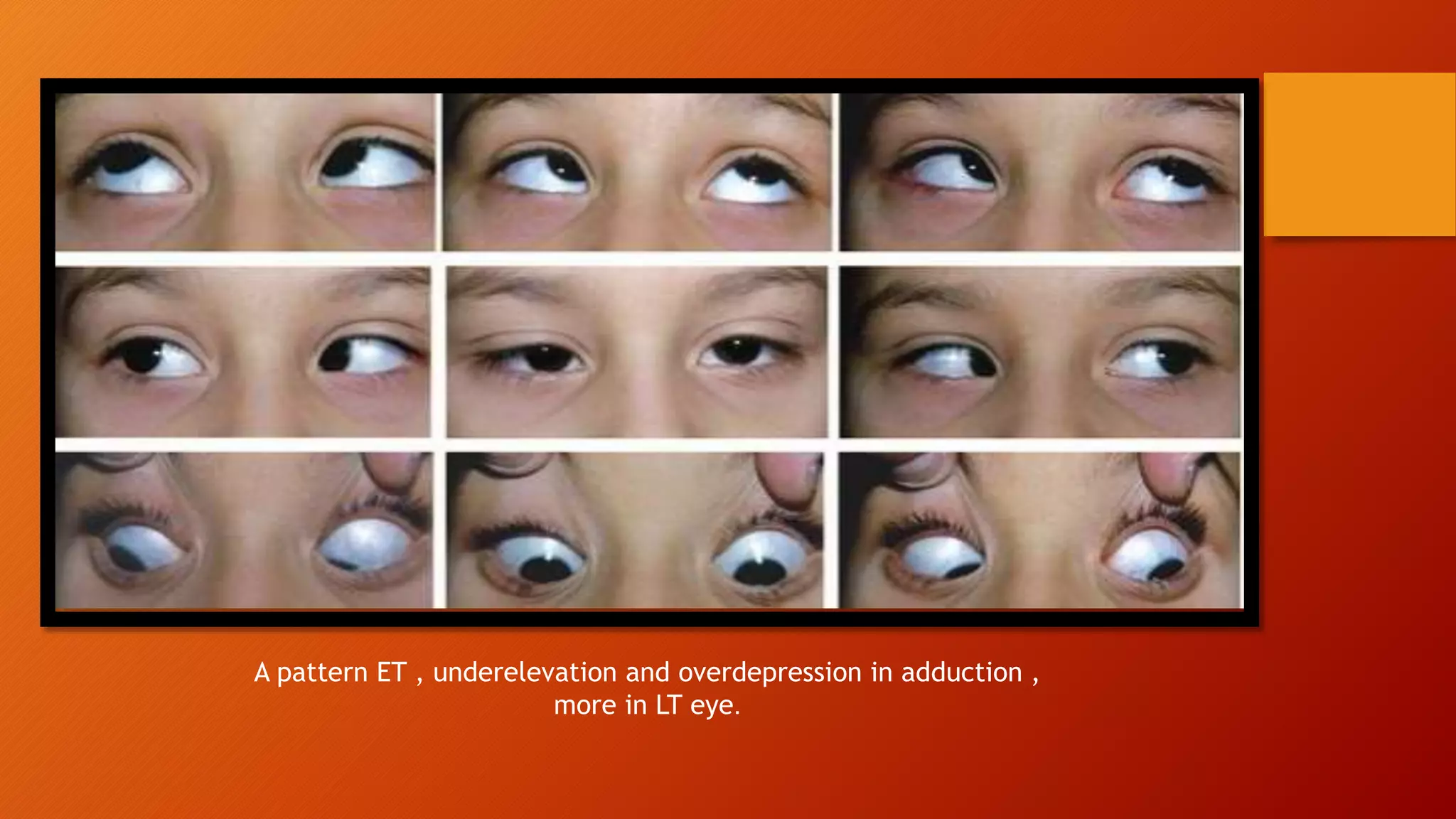
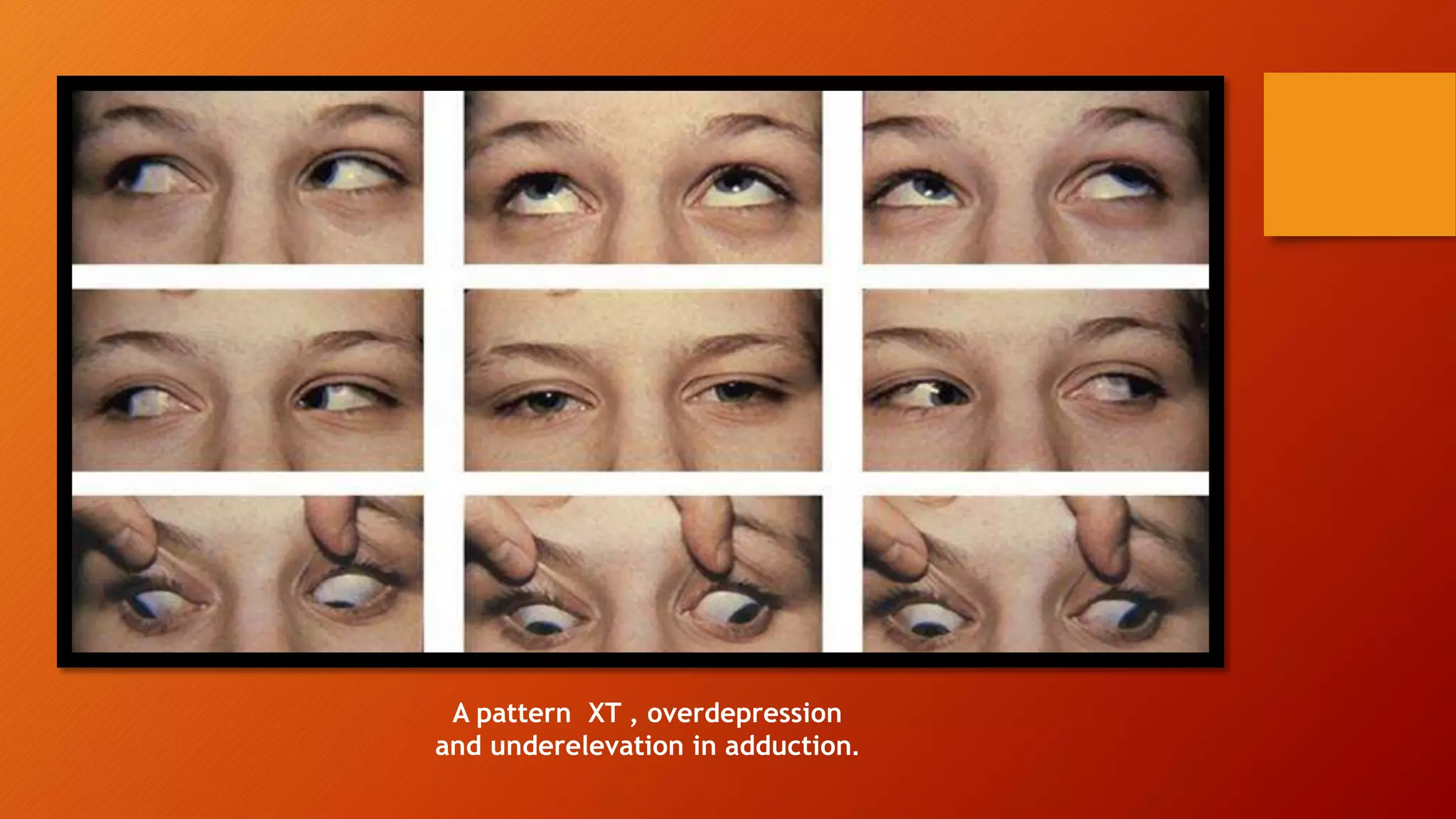
This document discusses different types of alphabet patterns in strabismus, including A and V patterns. An A pattern is defined as a horizontal deviation that is less divergent in upgaze than downgaze, usually caused by superior oblique overaction. A V pattern is more divergent in upgaze than downgaze, commonly due to inferior oblique overaction. Treatment of significant patterns may involve weakening overacting muscles and vertical translations of horizontal recti. Other patterns like Y, λ, and X patterns are also briefly described.