
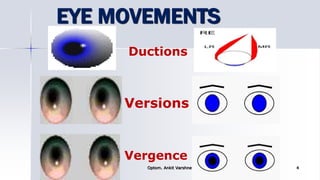


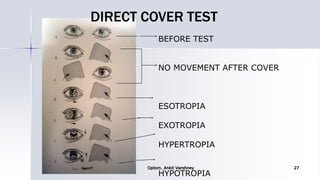
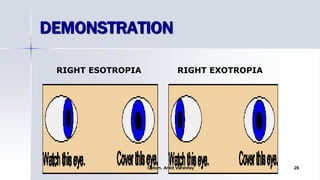
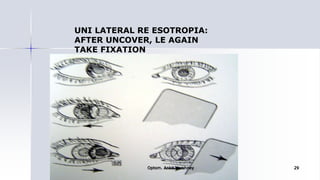


The document provides information on evaluating cases of orthoptics. It discusses evaluating a patient's history, visual acuity, eye movements, sensory status, and degree of strabismus. The evaluation includes assessing visual acuity, refraction, eye alignment using various objective tests like cover tests, assessing binocularity using stereopsis tests, and determining the presence of suppression or abnormal retinal correspondence. The document outlines the various tests used to evaluate motor and sensory functions in patients with strabismus.





















































































