Downloaded 3,998 times










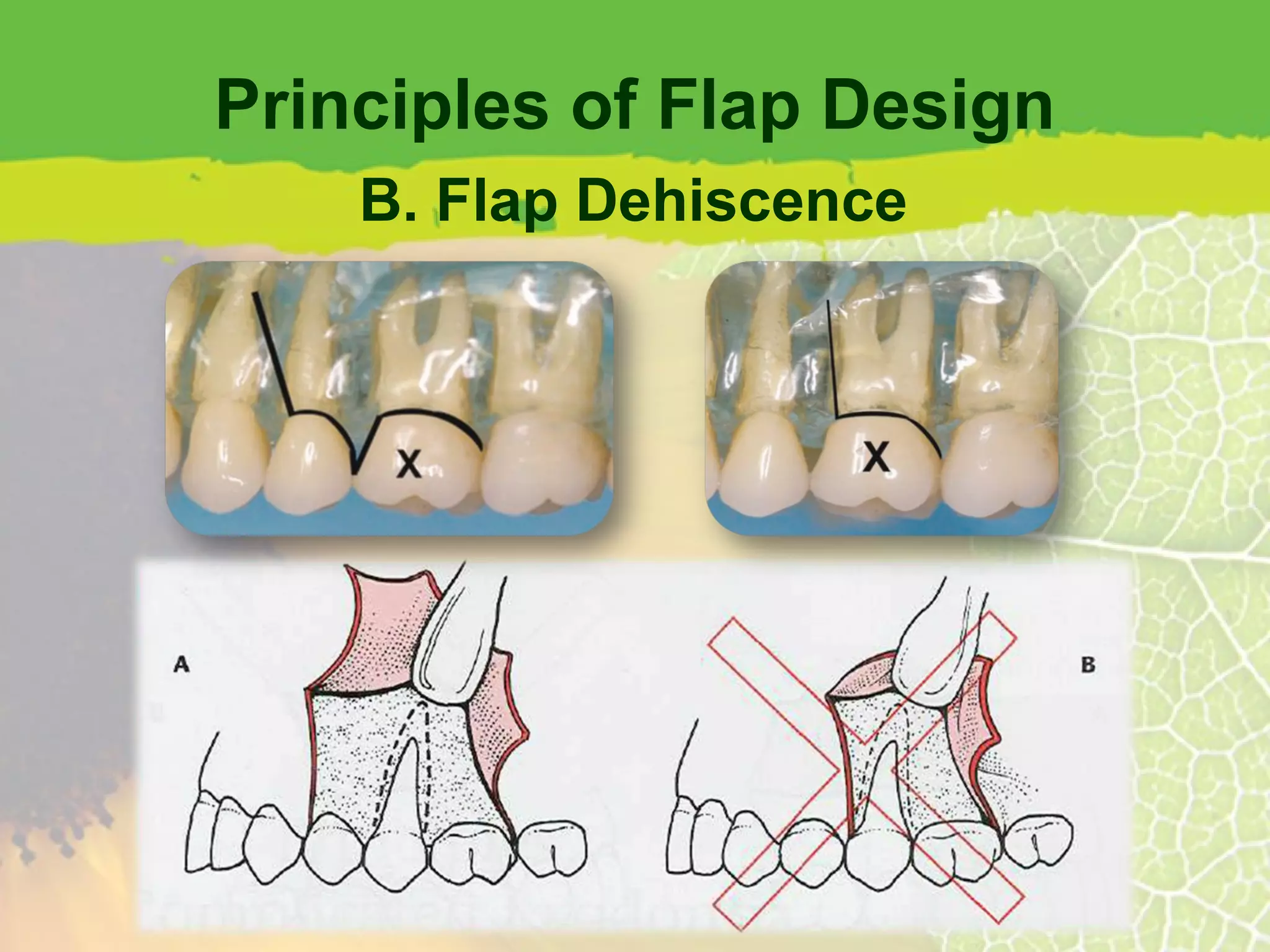

















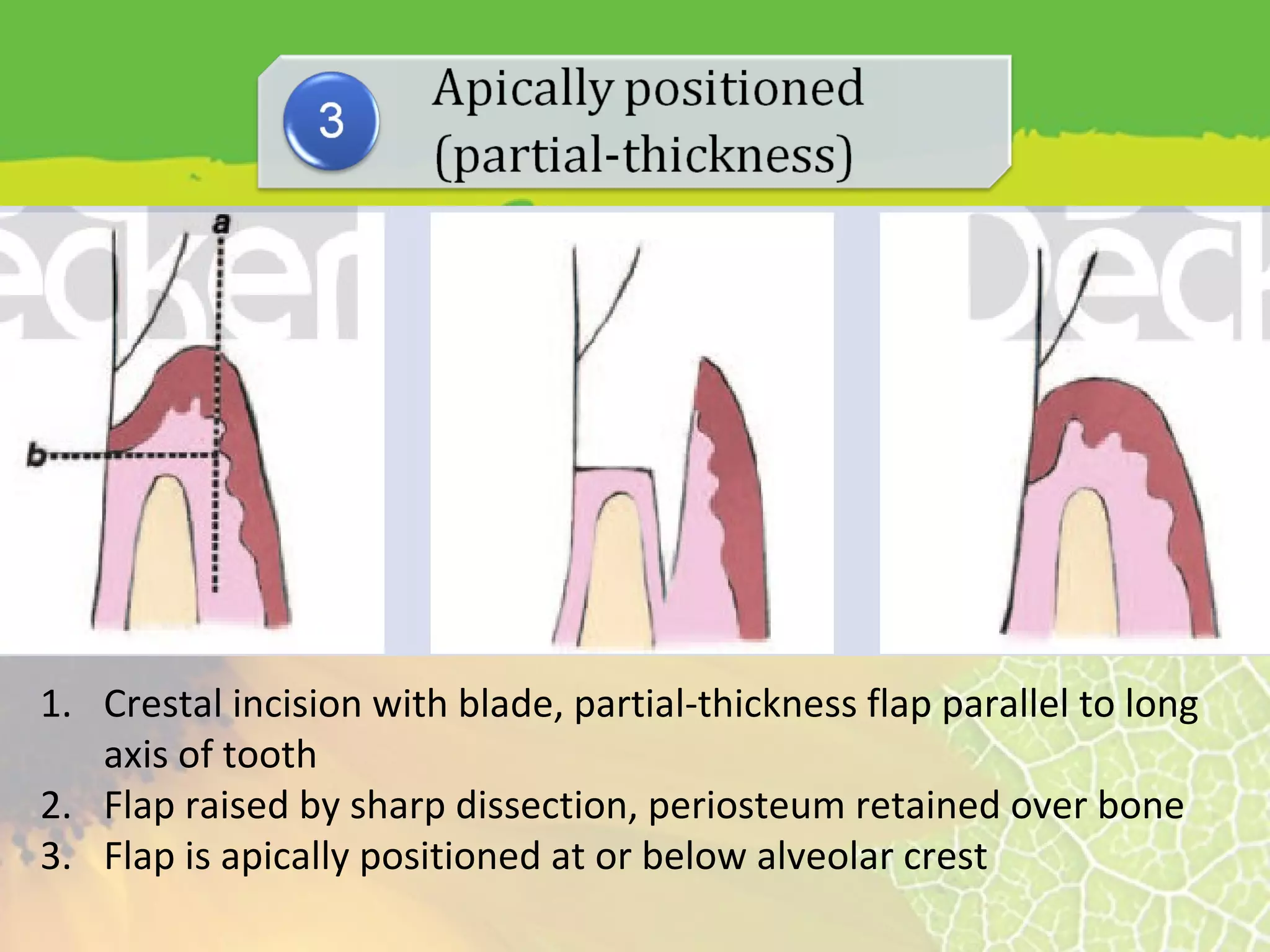
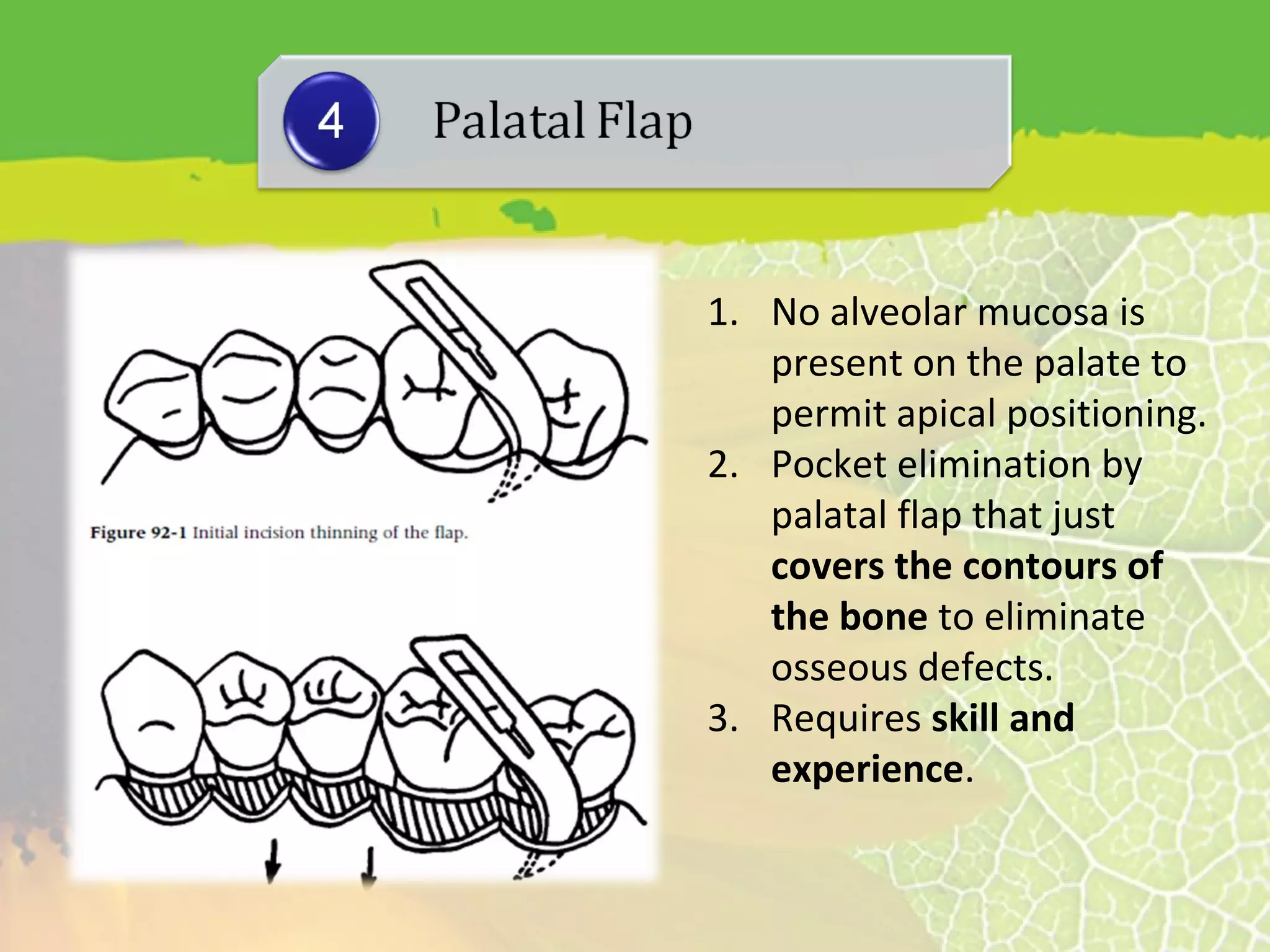








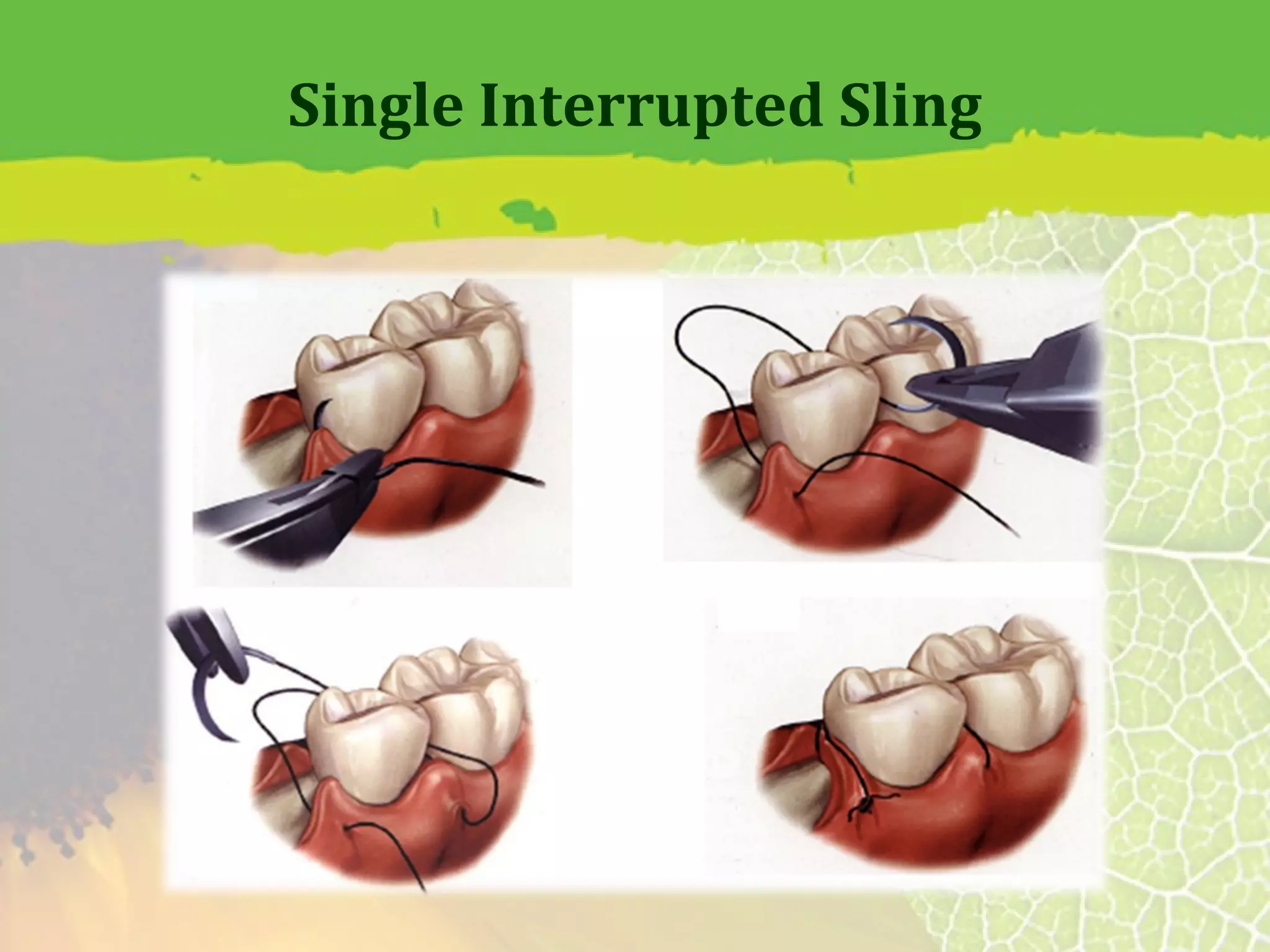
















This document provides information about flap surgery procedures in periodontics. It discusses the purposes of flap surgery, which include gaining access to deeper periodontal structures, relocating the frenulum, maintaining attached tissue, and eliminating pockets. It outlines the indications for flap surgery as well as contraindications. It then describes principles of flap design such as base width and length, blood supply, and avoiding tension. Different types of flaps and incisions are presented, along with techniques for suturing flaps. The document provides an overview of flap surgery procedures in periodontics.















































































