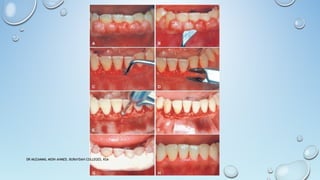
The document discusses gingivectomy and gingivoplasty, detailing their definitions, indications, contraindications, various surgical techniques, and healing processes. Gingivectomy involves the excision of gingiva to eliminate pockets or enlargements, while gingivoplasty reshapes gingiva for better contouring. Different methods, including surgical, electrosurgical, and laser techniques, are outlined, alongside the healing timeline and importance of proper post-operative care.