Downloaded 1,649 times
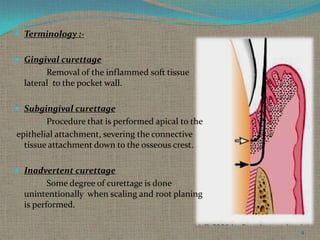
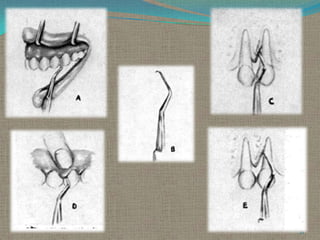
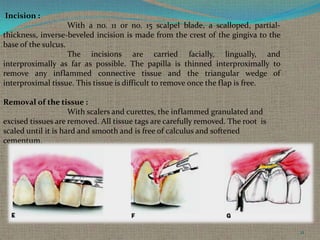
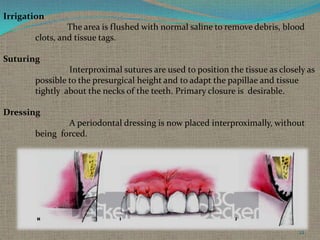
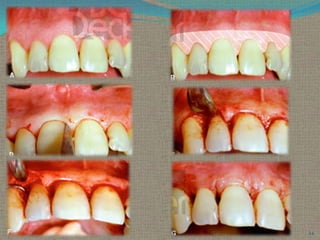

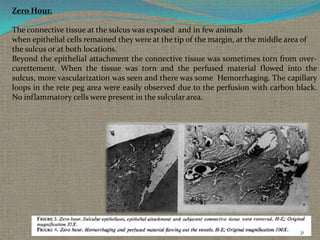
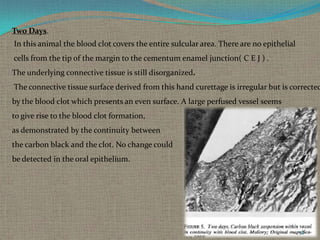
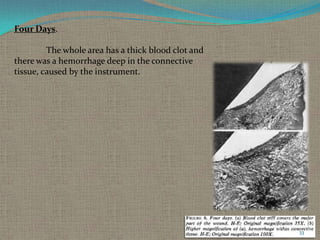
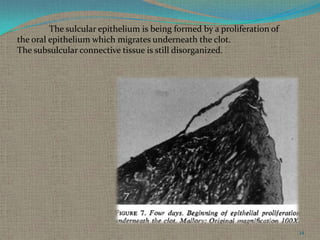
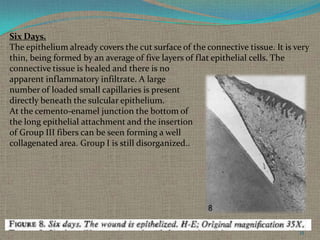
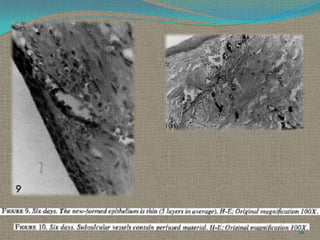
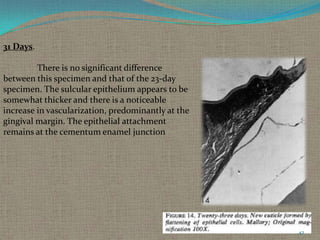

The document discusses gingival curettage, which involves using instruments to remove diseased soft tissue from periodontal pockets. It defines curettage and provides the history of the procedure. The basic technique is described as using curettes to scrape the inner lining of the pocket to remove ulcerated epithelium and damaged connective tissue. Indications include edematous pockets aiming to reduce inflammation and shrink tissue. Healing after curettage is examined through a study showing revascularization of the wound site over time.


































































