Downloaded 1,490 times

![ The following parameters need be
considered:
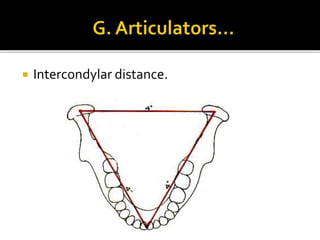
1. Intercondylar distance
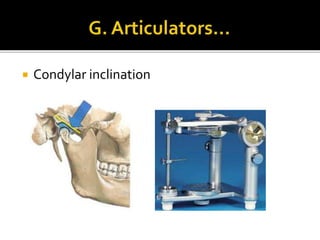
2. Condylar inclination
3. Mandibular arc of closure
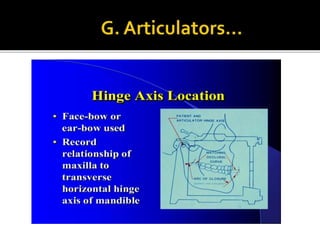
4. Hinge axis position [Centric Relation (CR)
and Centric Occlusion (CO)]](https://image.slidesharecdn.com/centricrelation-141018104357-conversion-gate01/85/Centric-relation-54-320.jpg)

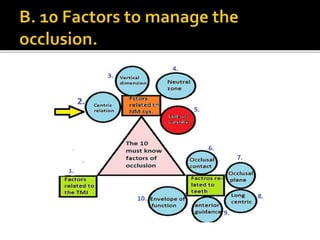
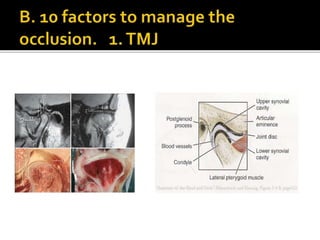
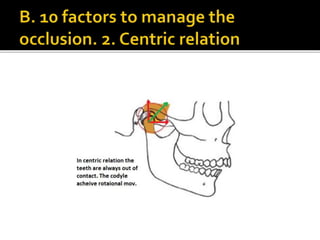
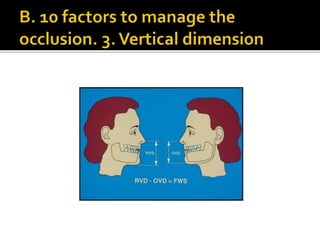
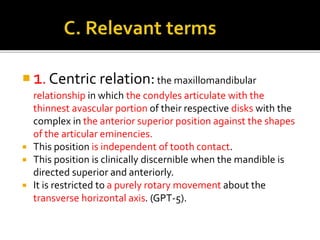
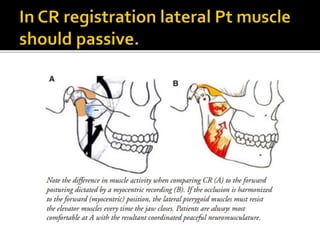
The document discusses the concepts of centric relation (CR) and maximum intercuspation position (MIP) within the masticatory system, outlining their significance in dental procedures and occlusion management. It emphasizes the importance of understanding the relationship between CR and MIP to prevent pathologic conditions and to ensure effective treatment for occlusal problems. Furthermore, it details the role of articulators in simulating jaw movements and achieving accurate dental work, highlighting the necessity of proper occlusal adjustments for patient comfort.








































![occlusion mmmmmmmm- Copy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/occlusion-copyautosaved-240715160312-7fd34768-thumbnail.jpg?width=640&height=640&fit=bounds)













































