Downloaded 3,602 times

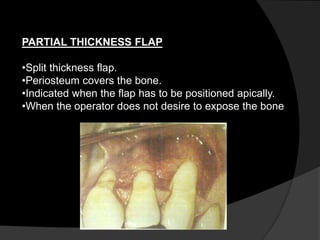








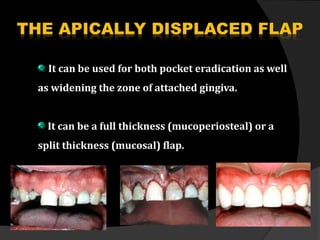



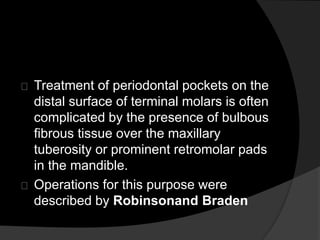

This document discusses periodontal flaps, which are sections of gingiva surgically separated from underlying tissues to provide access to bone and roots. It defines different types of flaps classified by bone exposure, placement, and papilla design. Indications and contraindications for various flaps are outlined. Procedures for modified Widman, undisplaced, apically displaced, and regenerative flaps are described. Distal molar surgery techniques and use of periodontal packs are also summarized.













































































