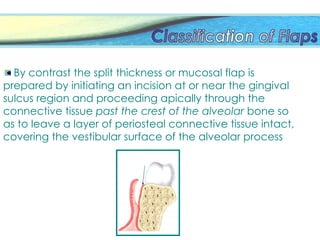
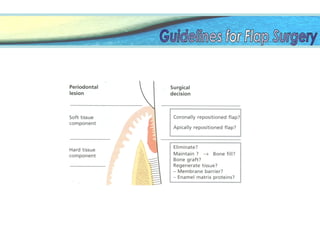
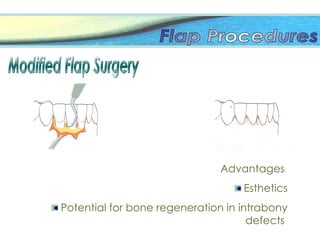
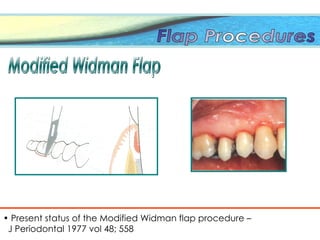
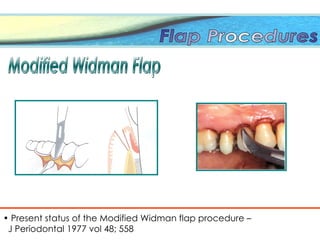
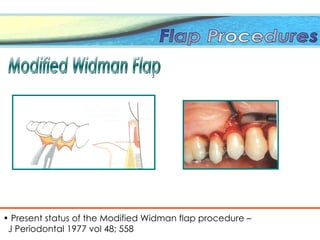
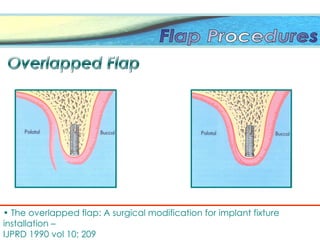
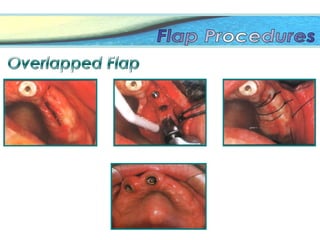
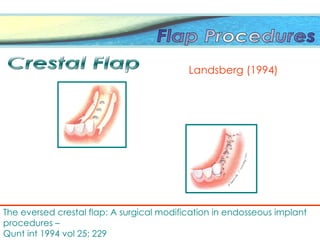
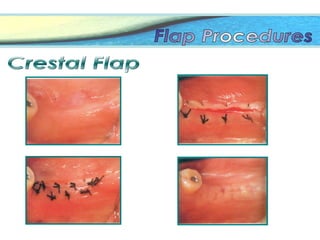
The document discusses the various surgical techniques and classifications of periodontal flaps used in the treatment of periodontal diseases. It details the definitions, types, and advantages of full thickness and partial thickness flaps, as well as specific incision techniques and their implications for healing and bone regeneration. The text also addresses considerations for flap survival and complications, such as hemorrhage and postoperative care.