Downloaded 103 times
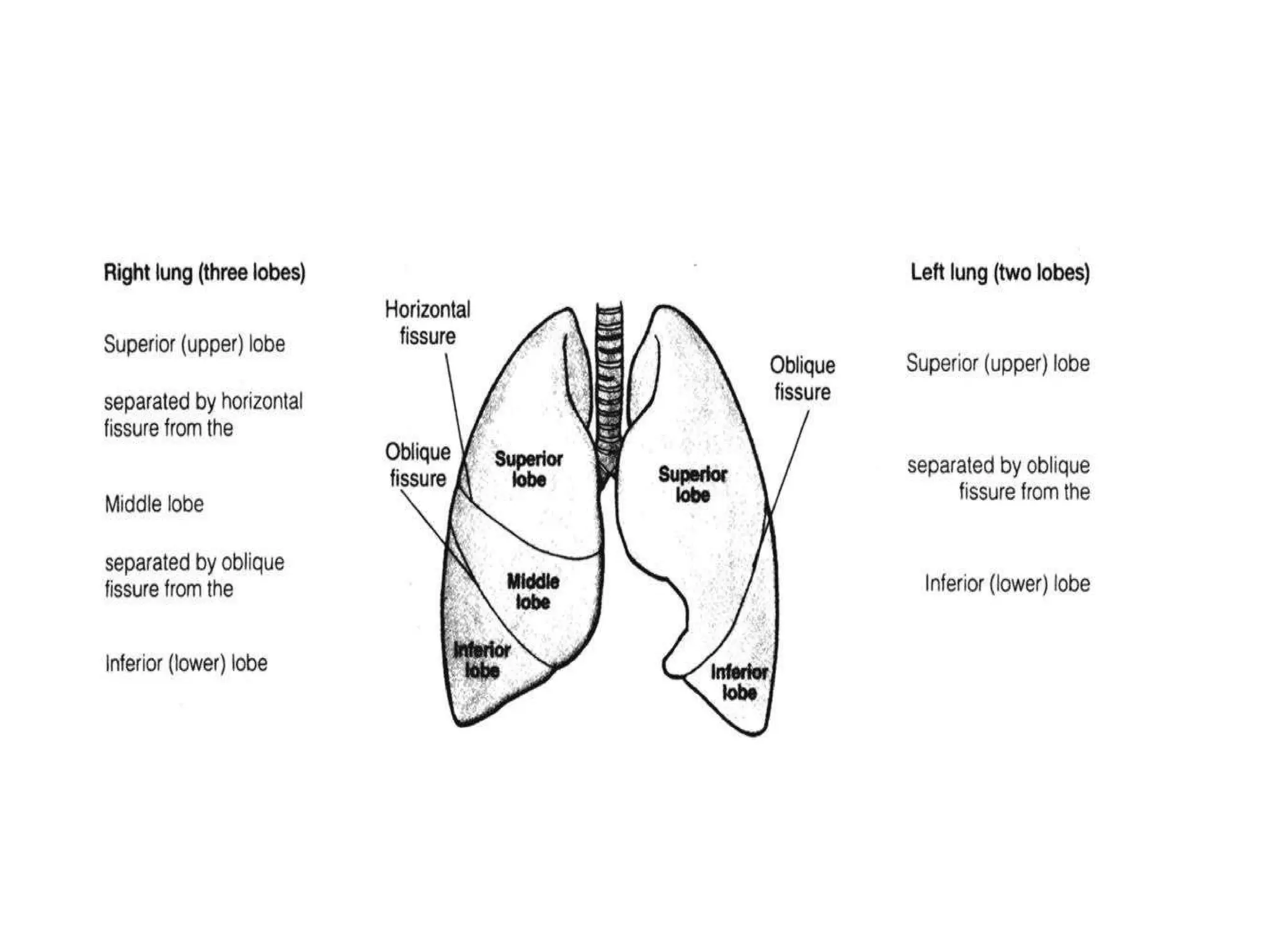
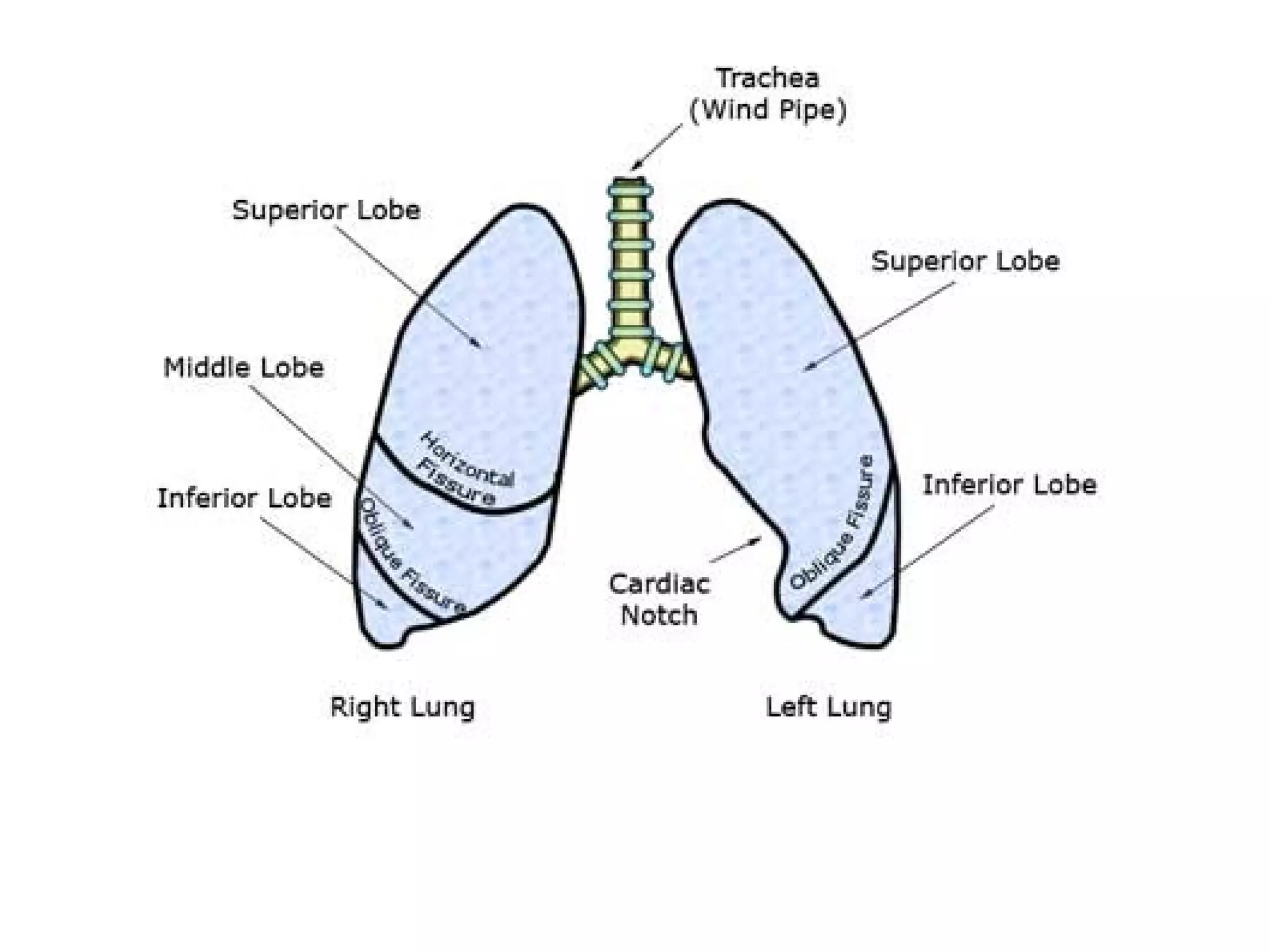


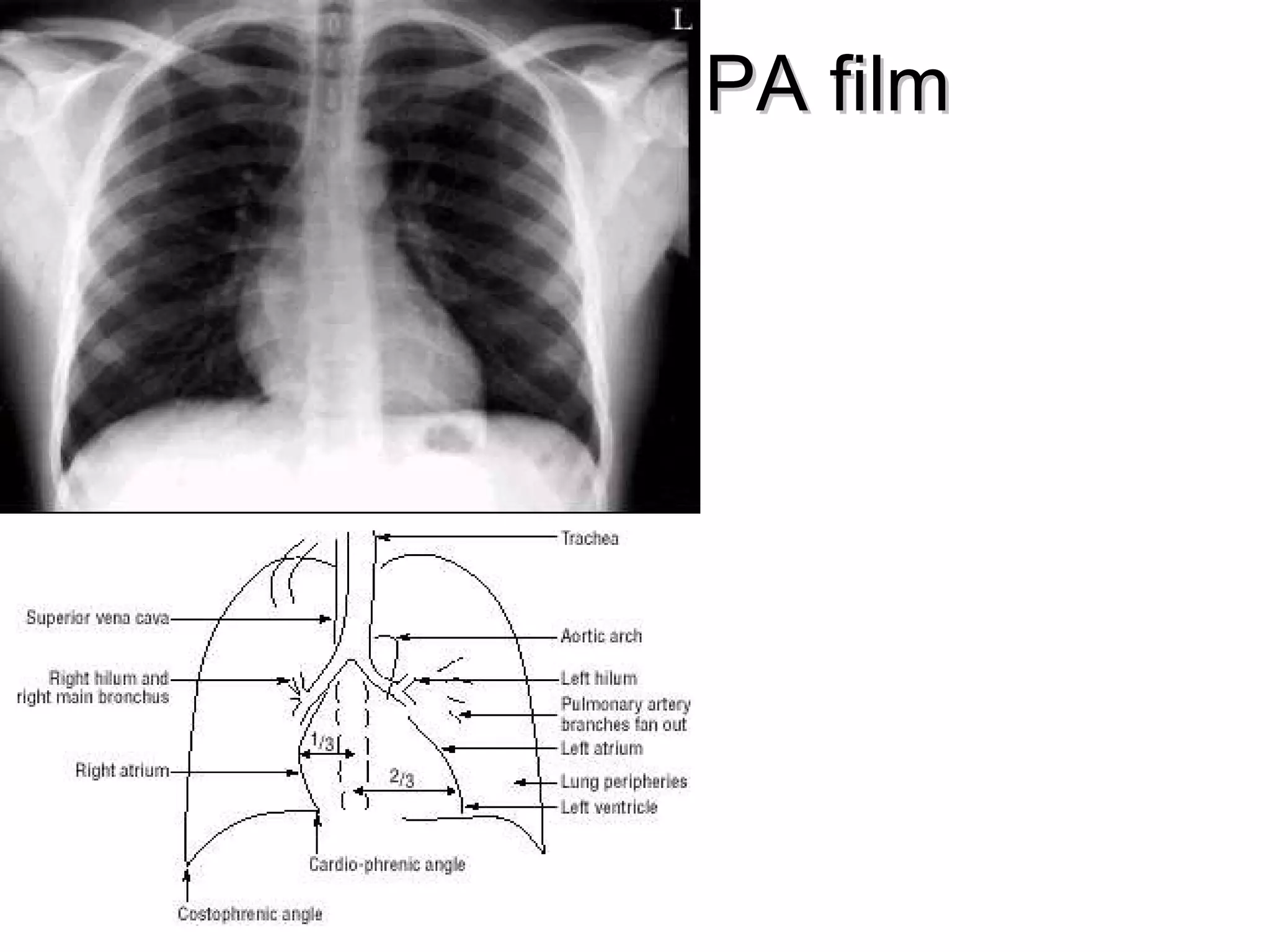
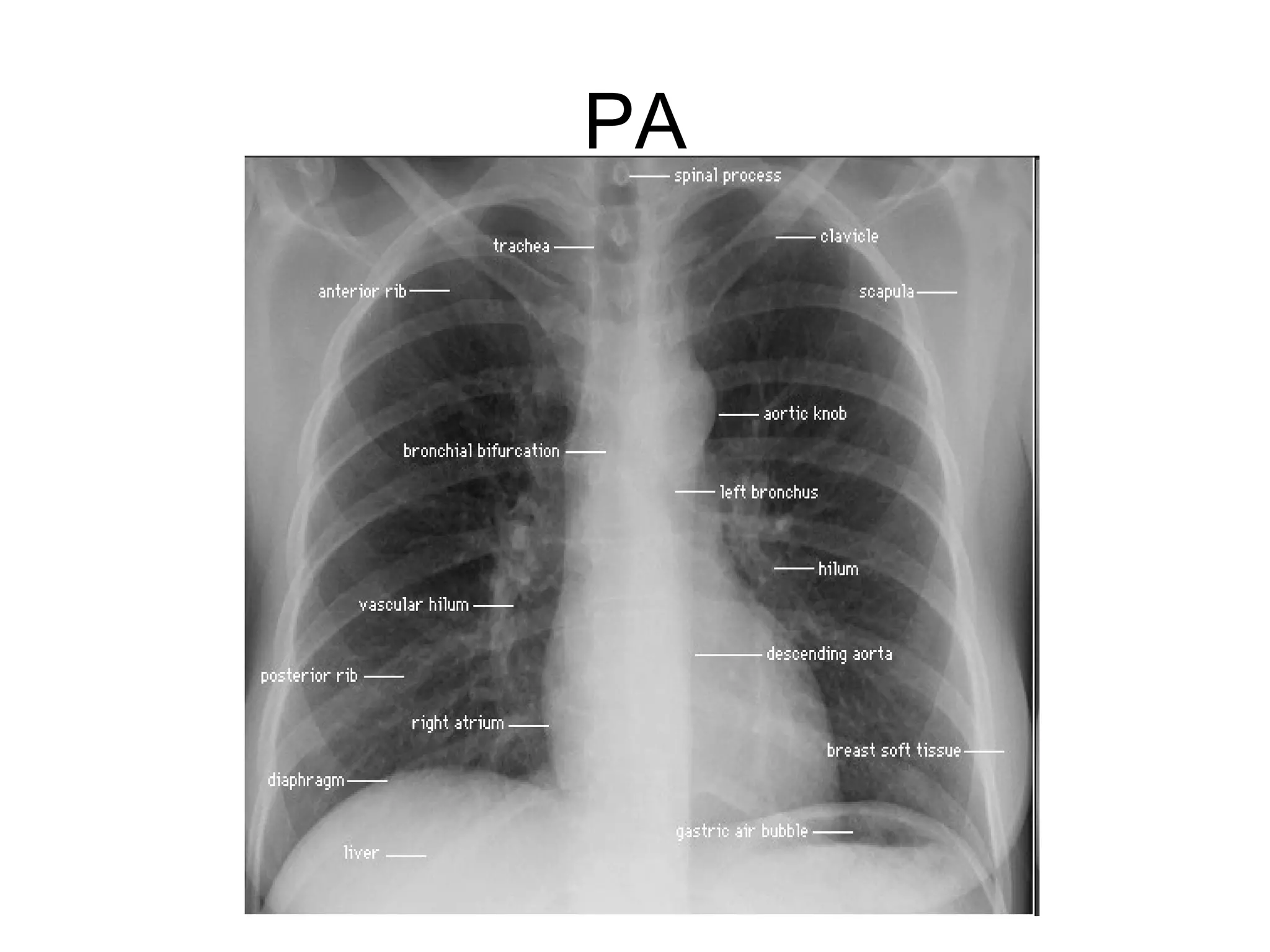
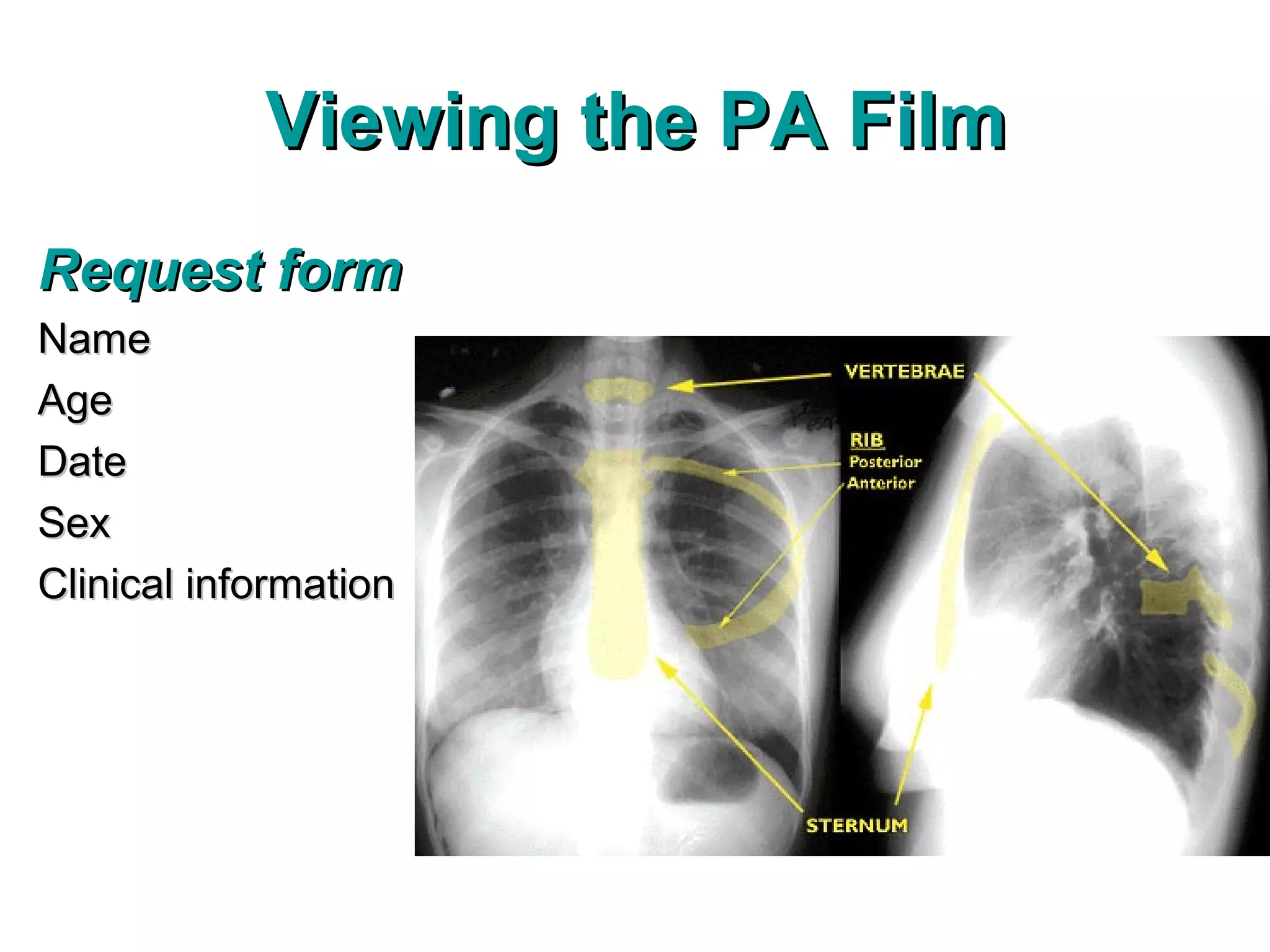
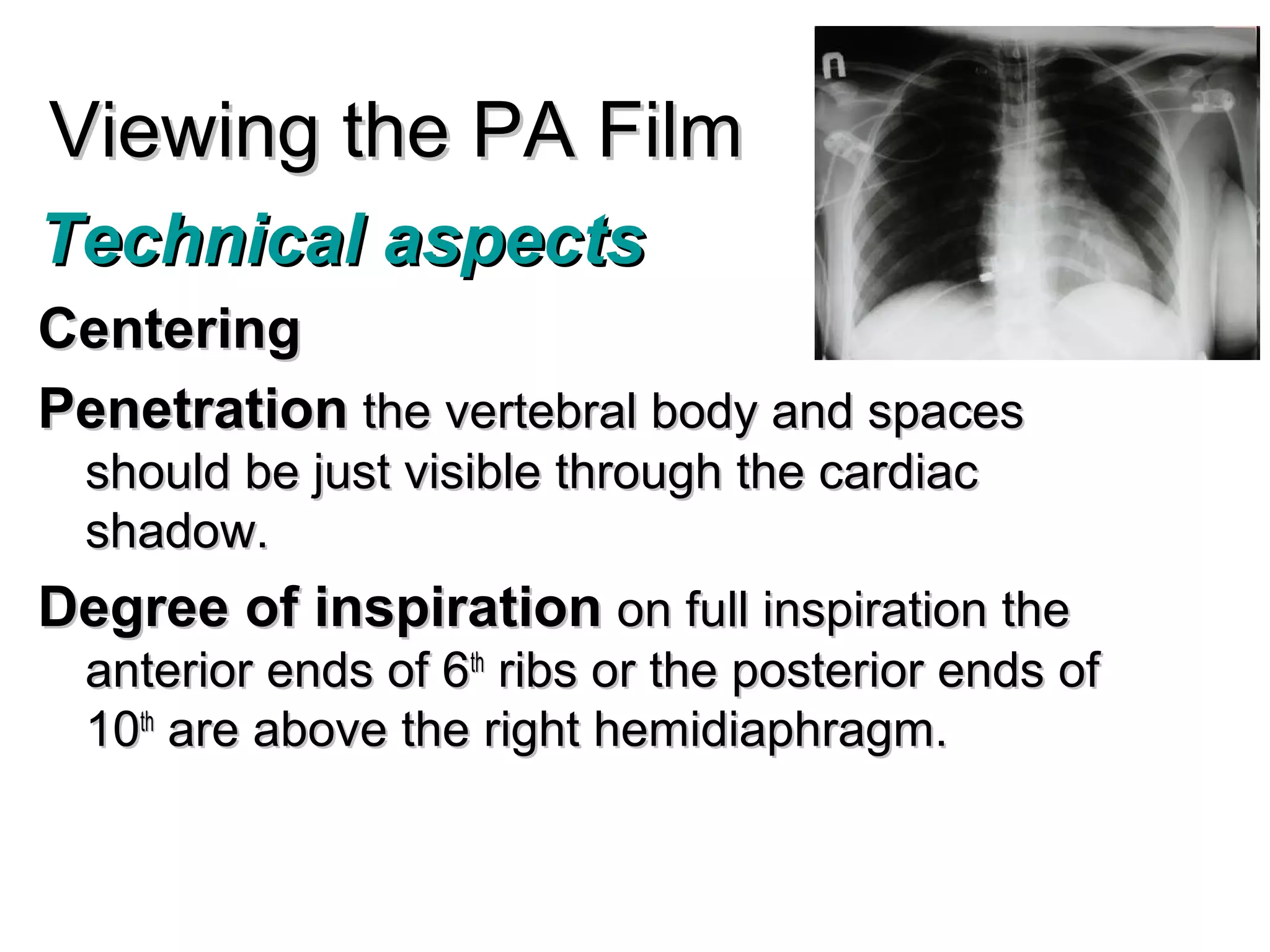
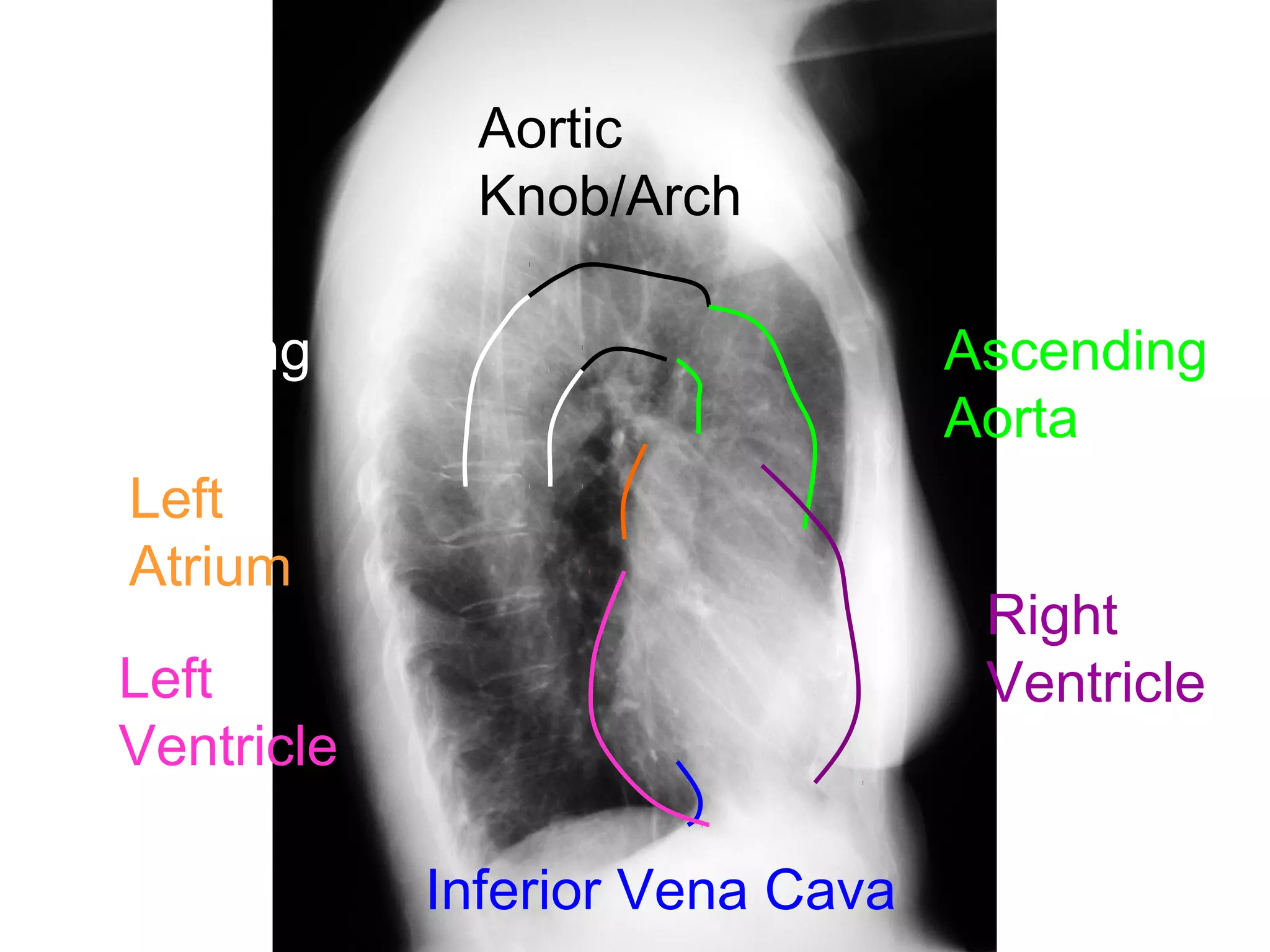
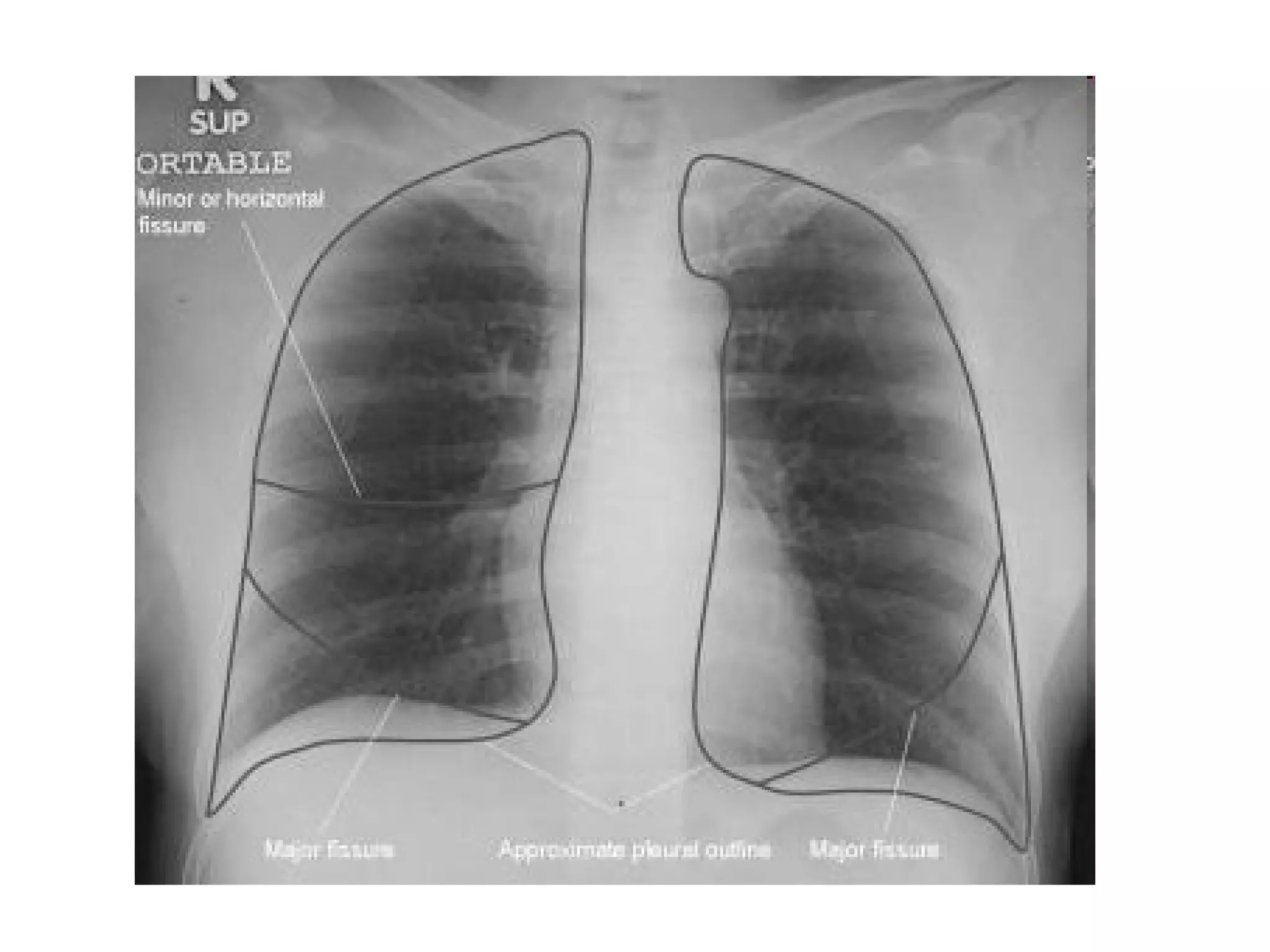
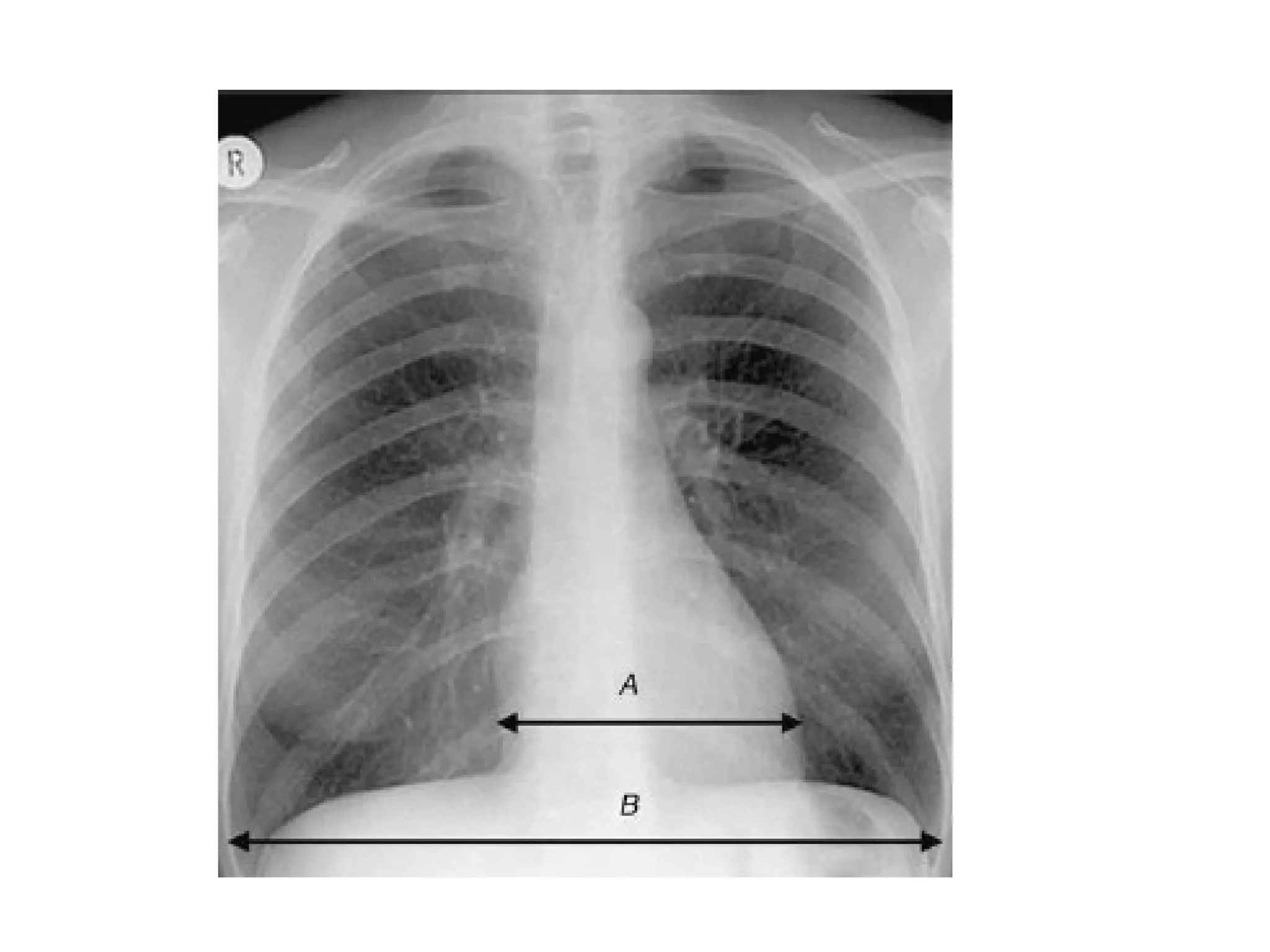
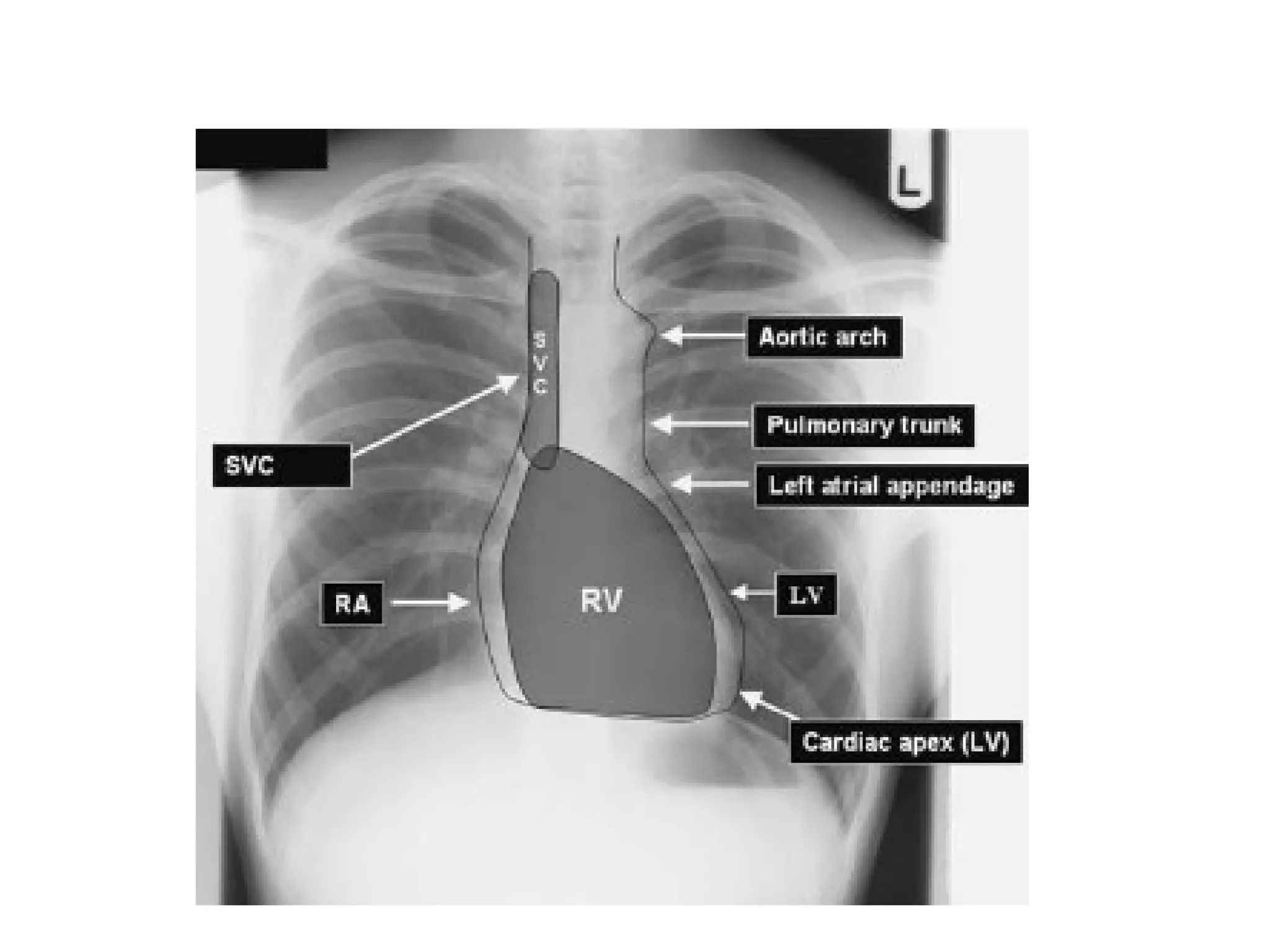
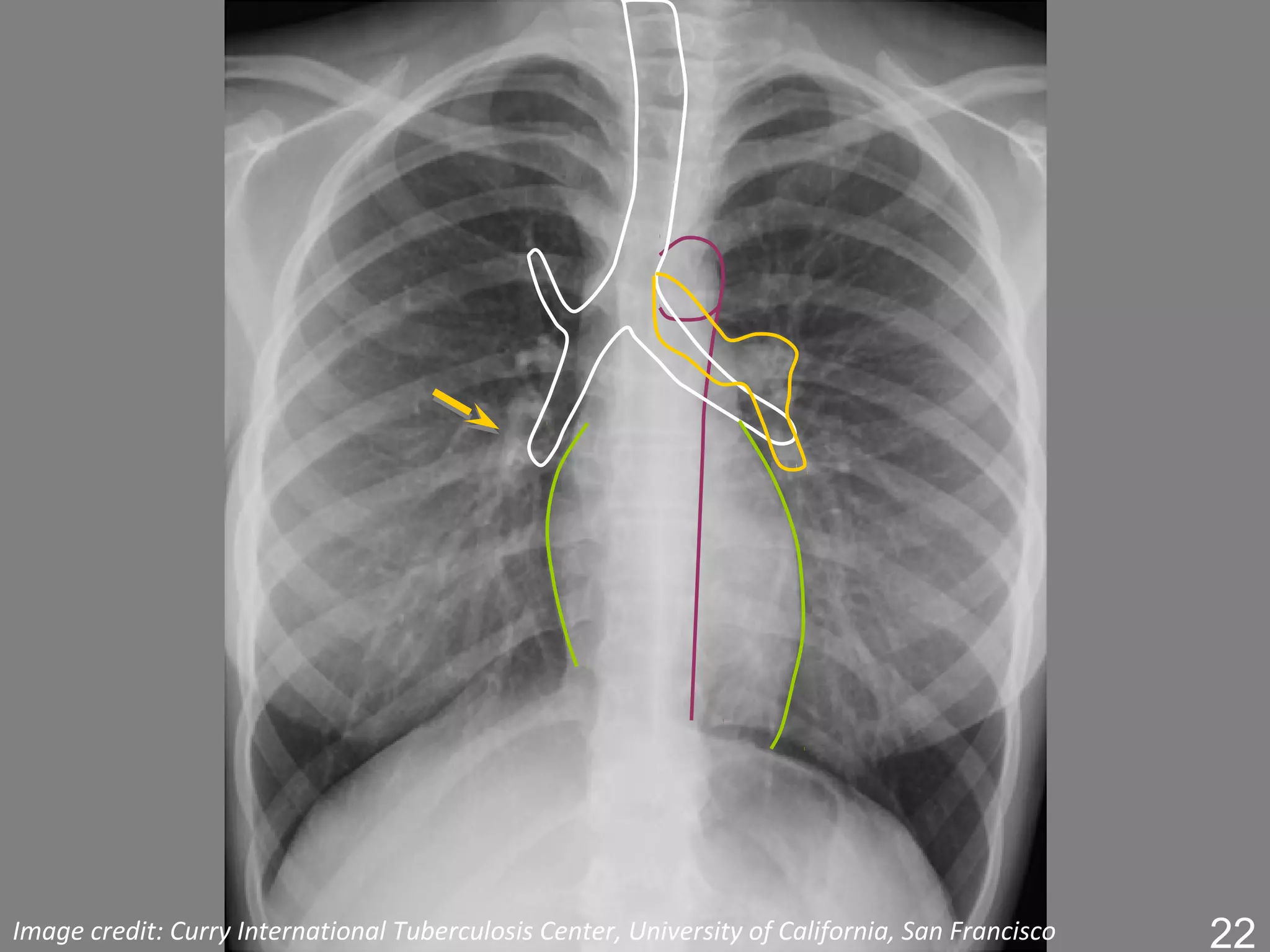
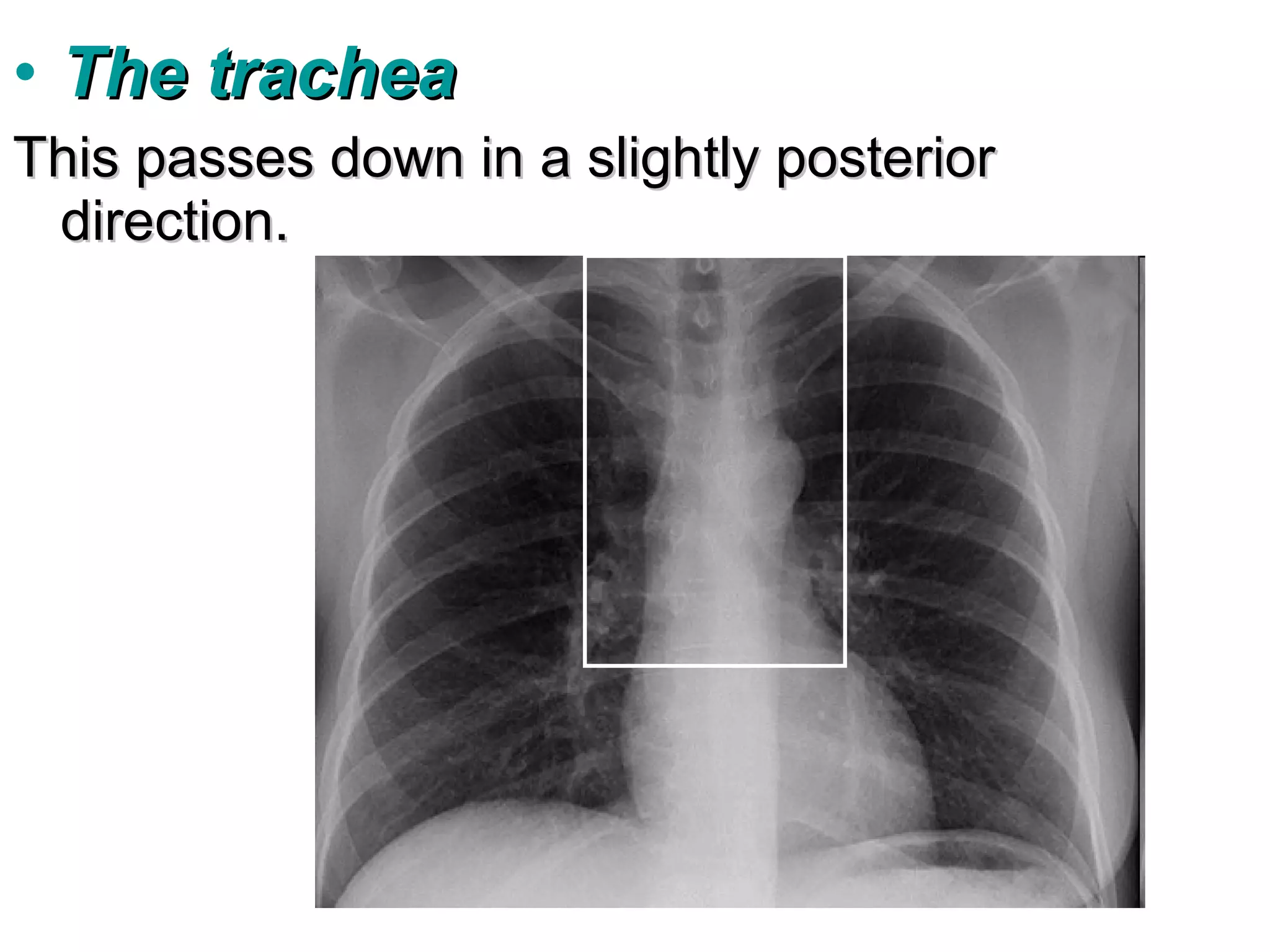
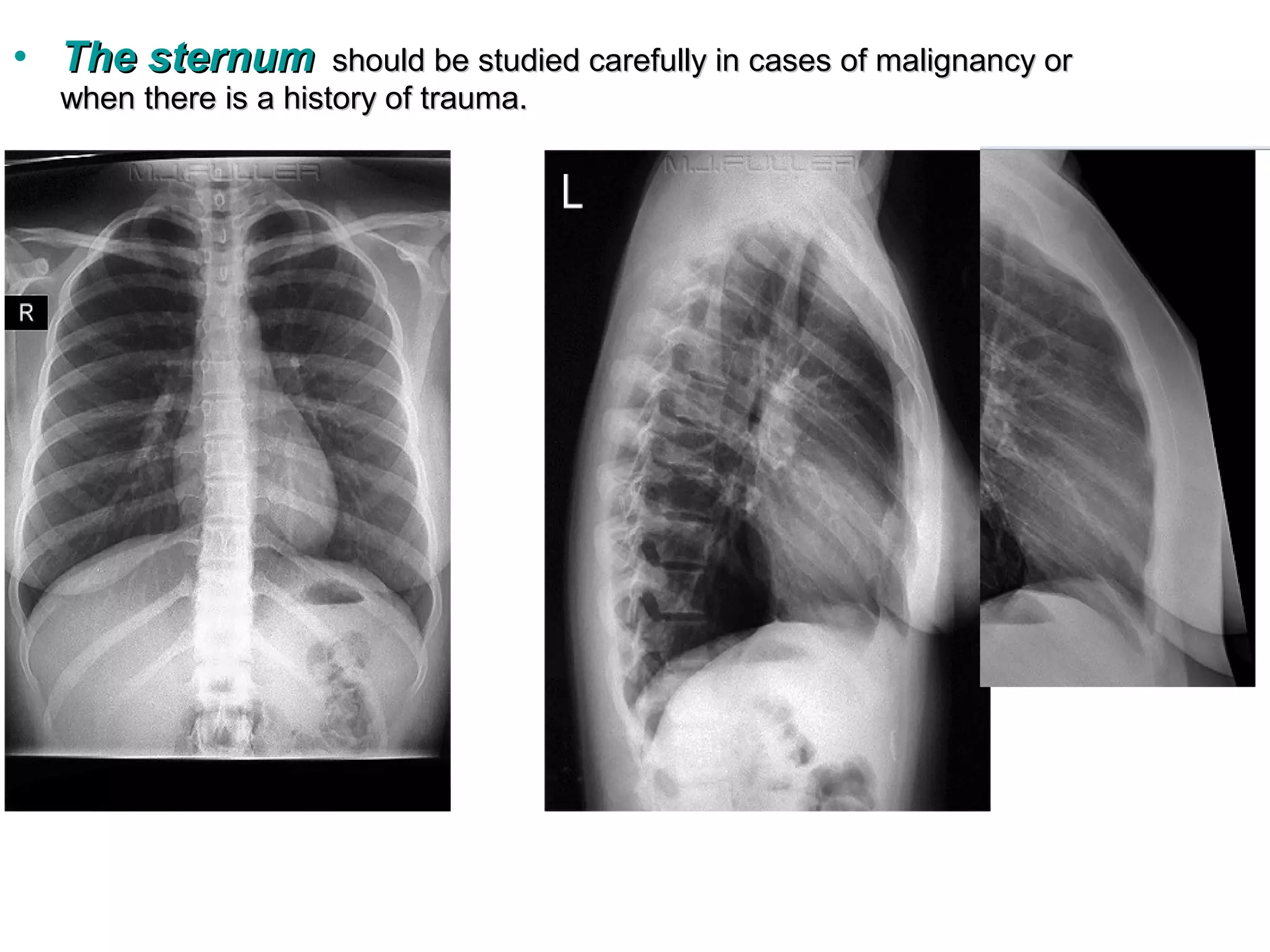
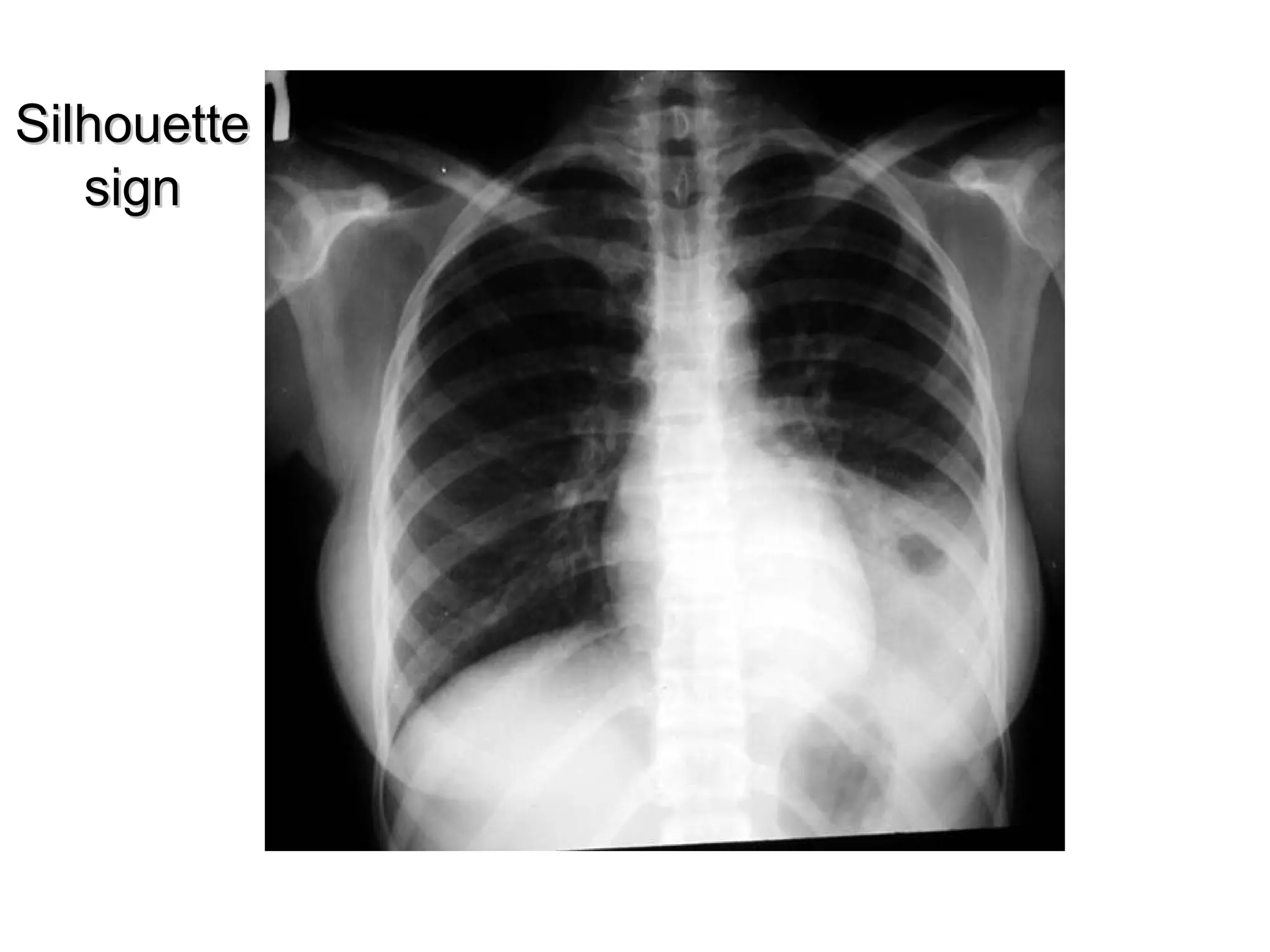


This document provides an overview of how to view and interpret a normal chest x-ray (CXR) and discusses some key radiological concepts: 1. It describes the technical aspects of a PA view CXR including proper centering, inspiration level, and visibility of structures like the trachea. 2. The mediastinum, heart, diaphragm, lungs, bones, and soft tissues are identified and their normal appearances discussed. 3. Important radiological signs like the silhouette sign and air bronchogram that are used to interpret abnormal films are introduced.



































![Radiografia De TòRax [Modo De Compatibilidad]](https://cdn.slidesharecdn.com/ss_thumbnails/radiografiadetraxmododecompatibilidad-100319093214-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















































