This document provides a detailed overview of peritoneal anatomy and spaces. It begins by explaining the importance for radiologists to understand peritoneal spaces to localize disease. Key points include:
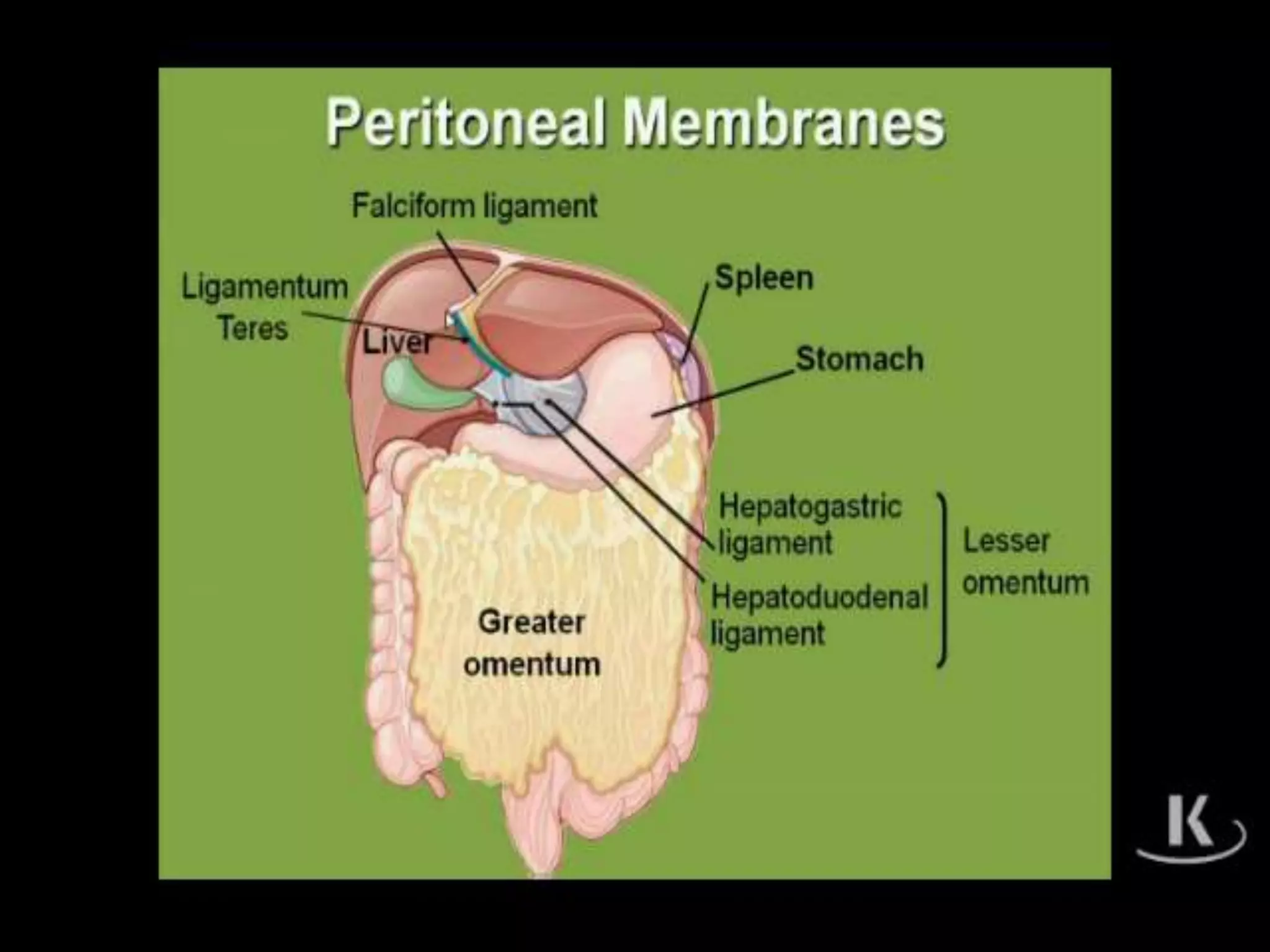
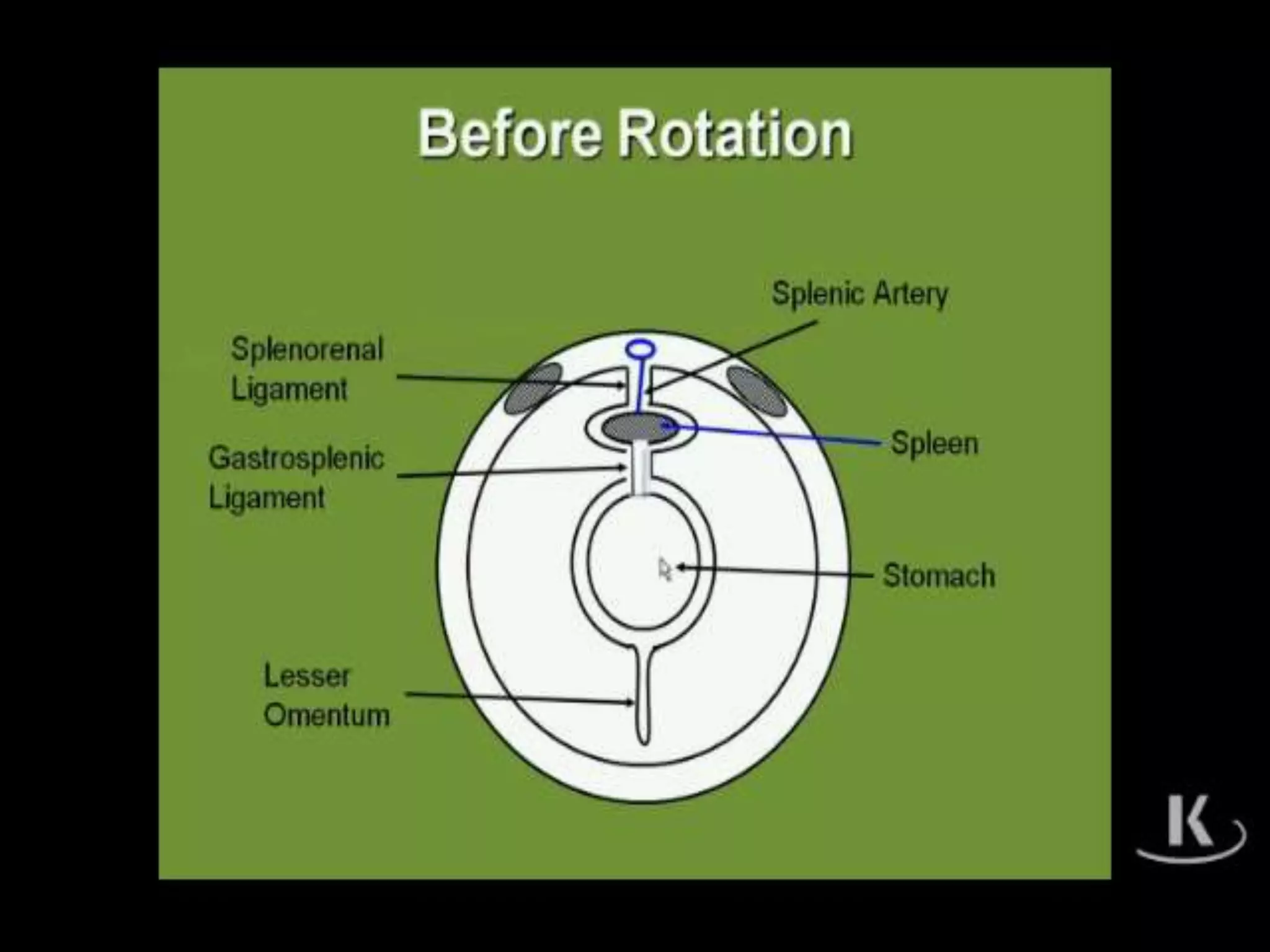
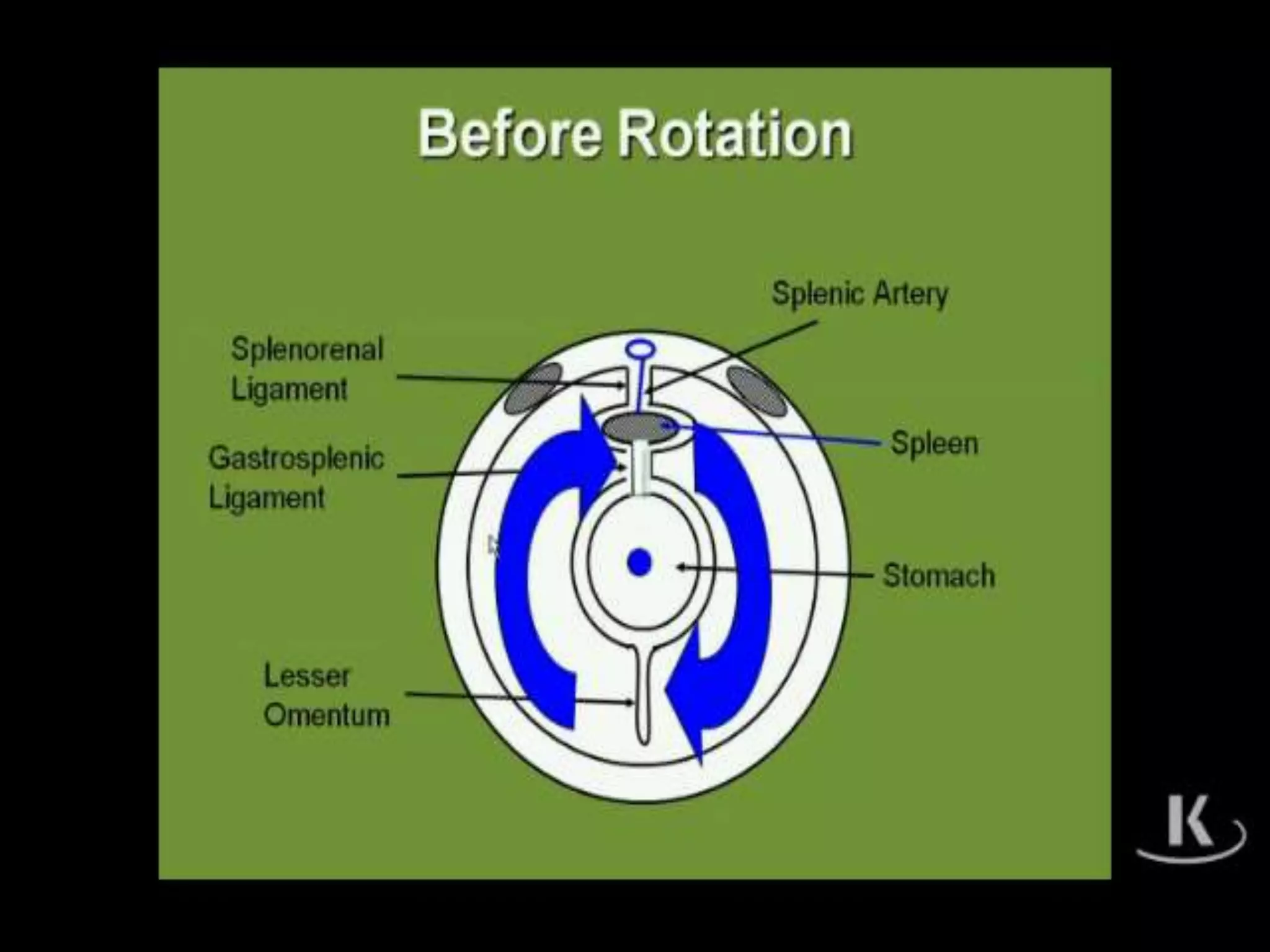
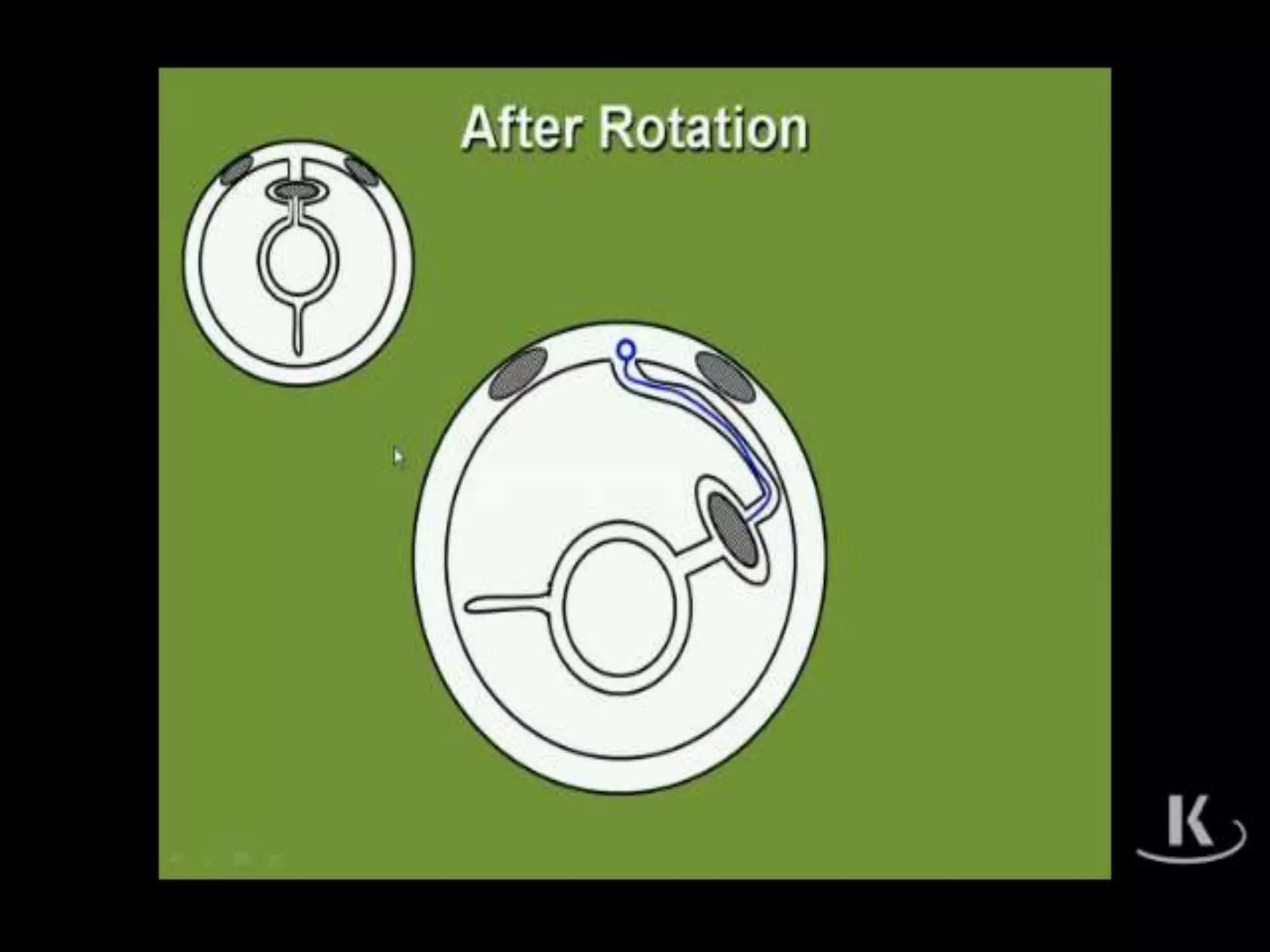
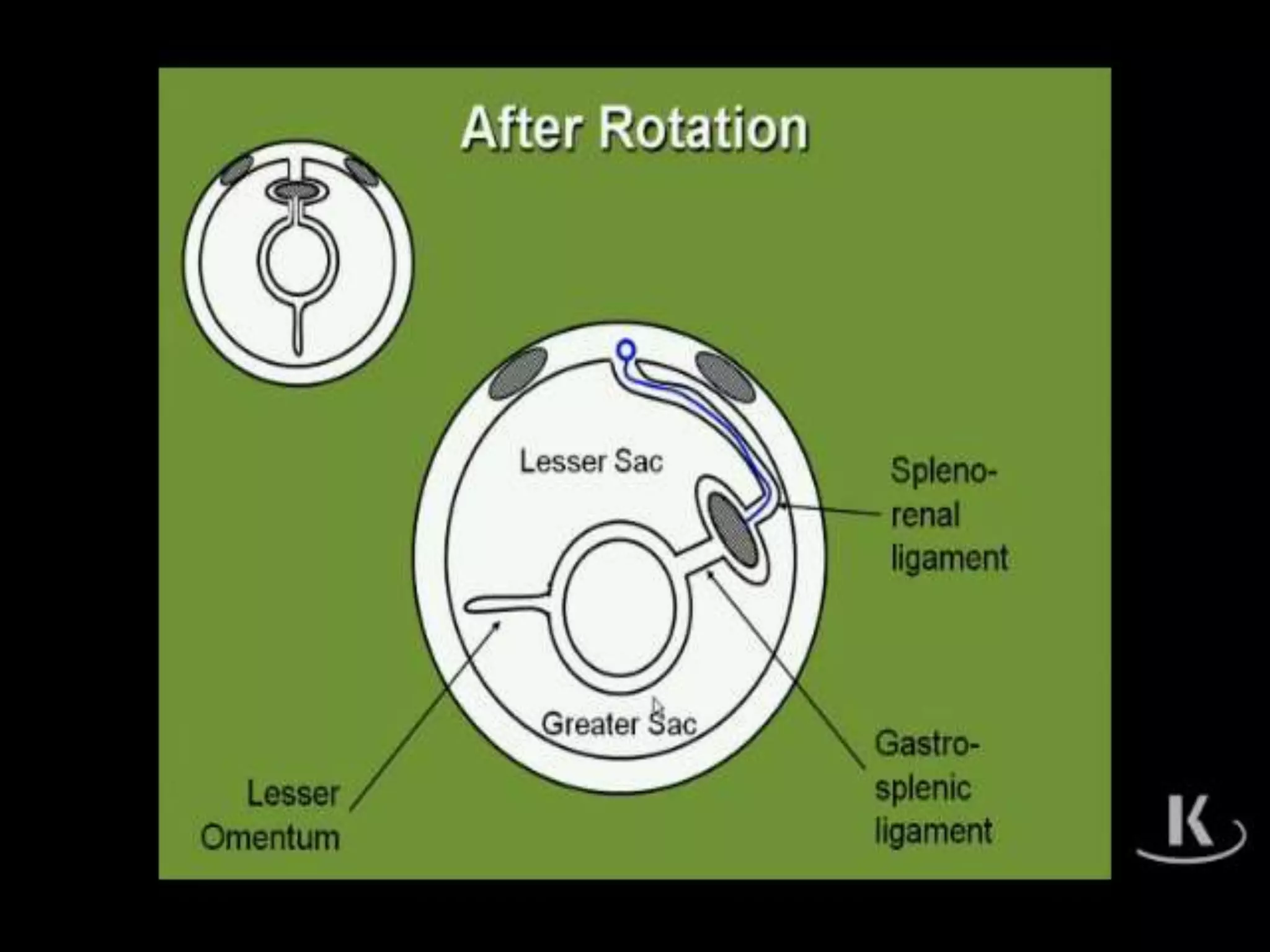
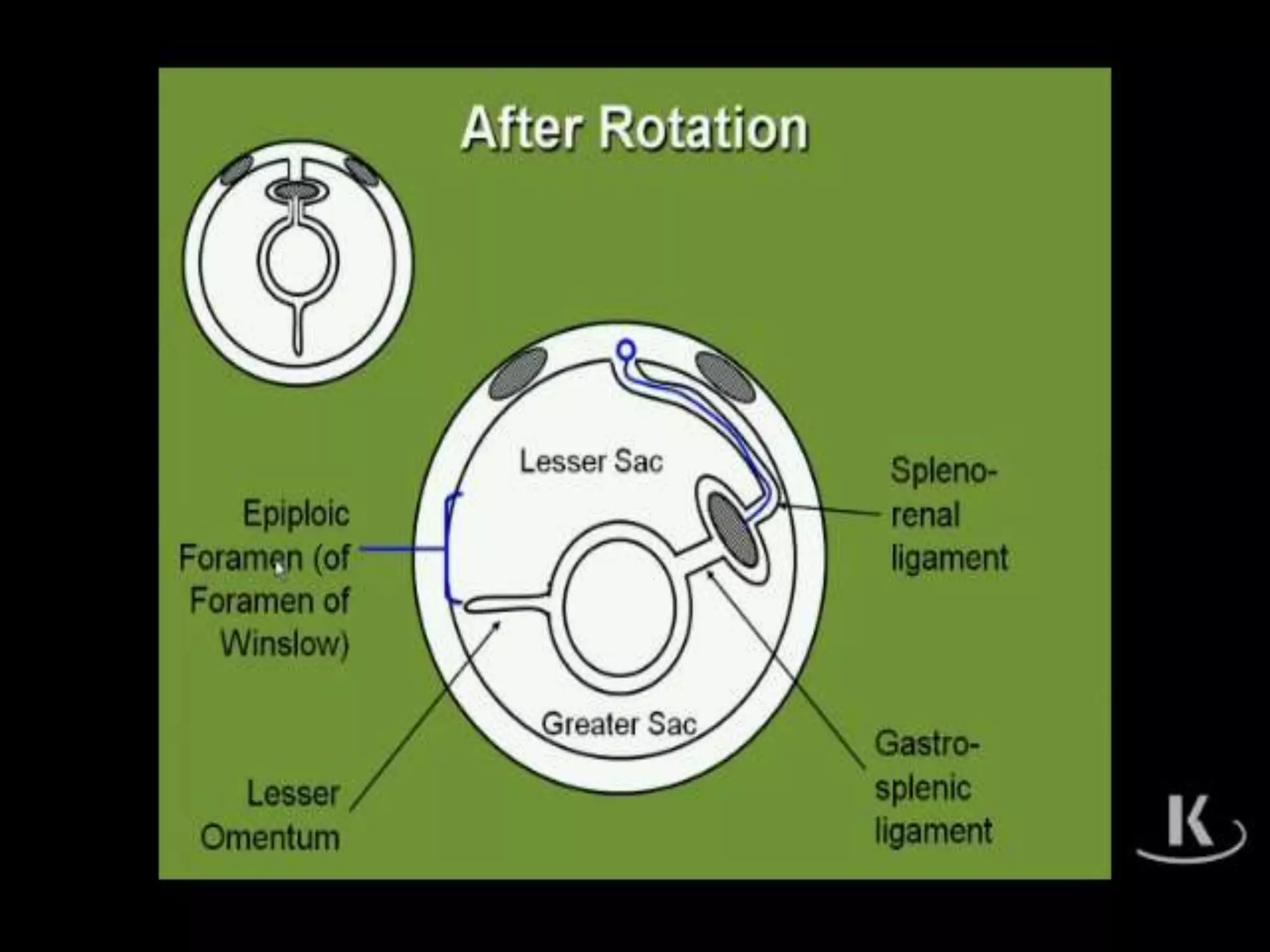
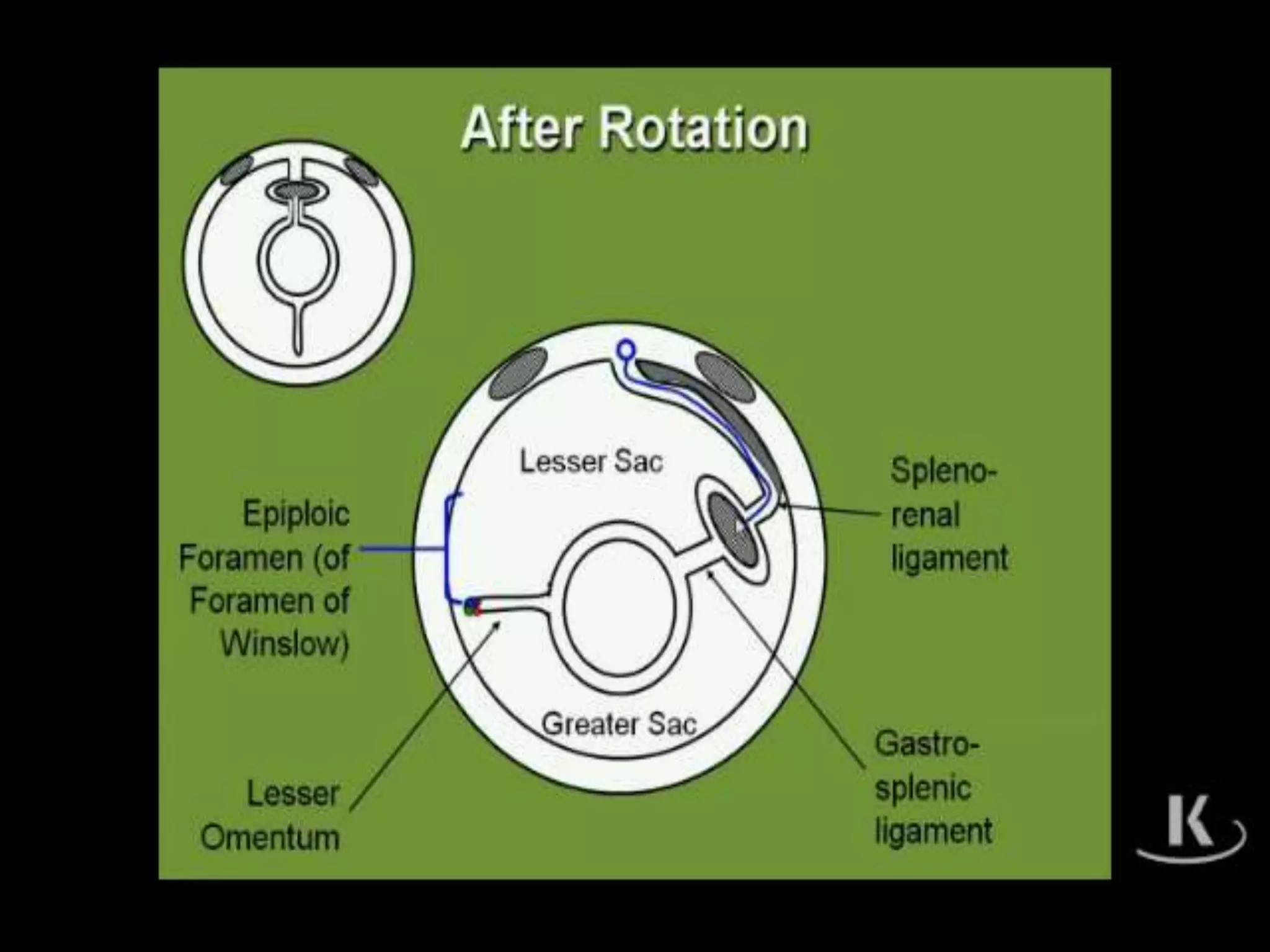
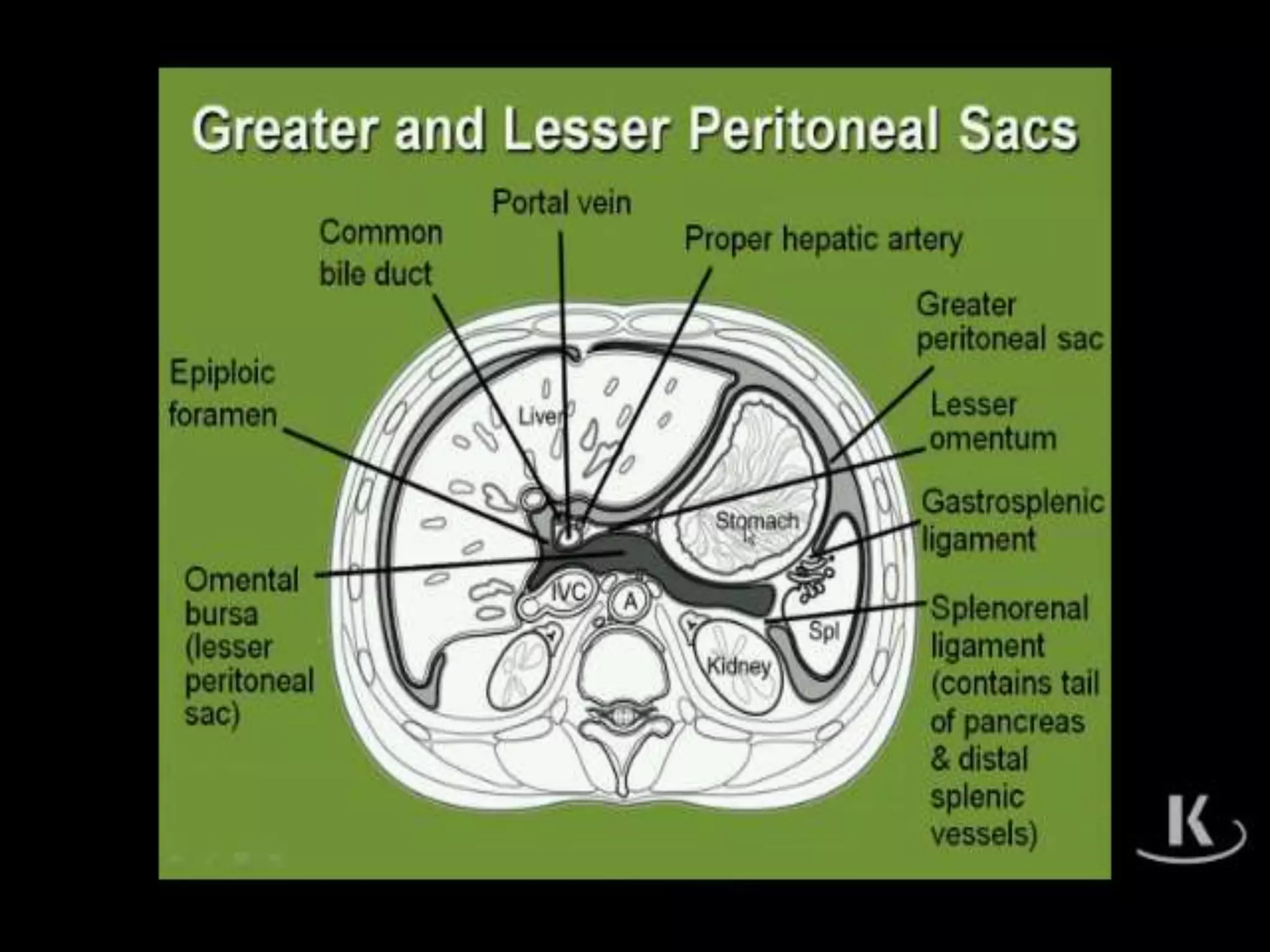
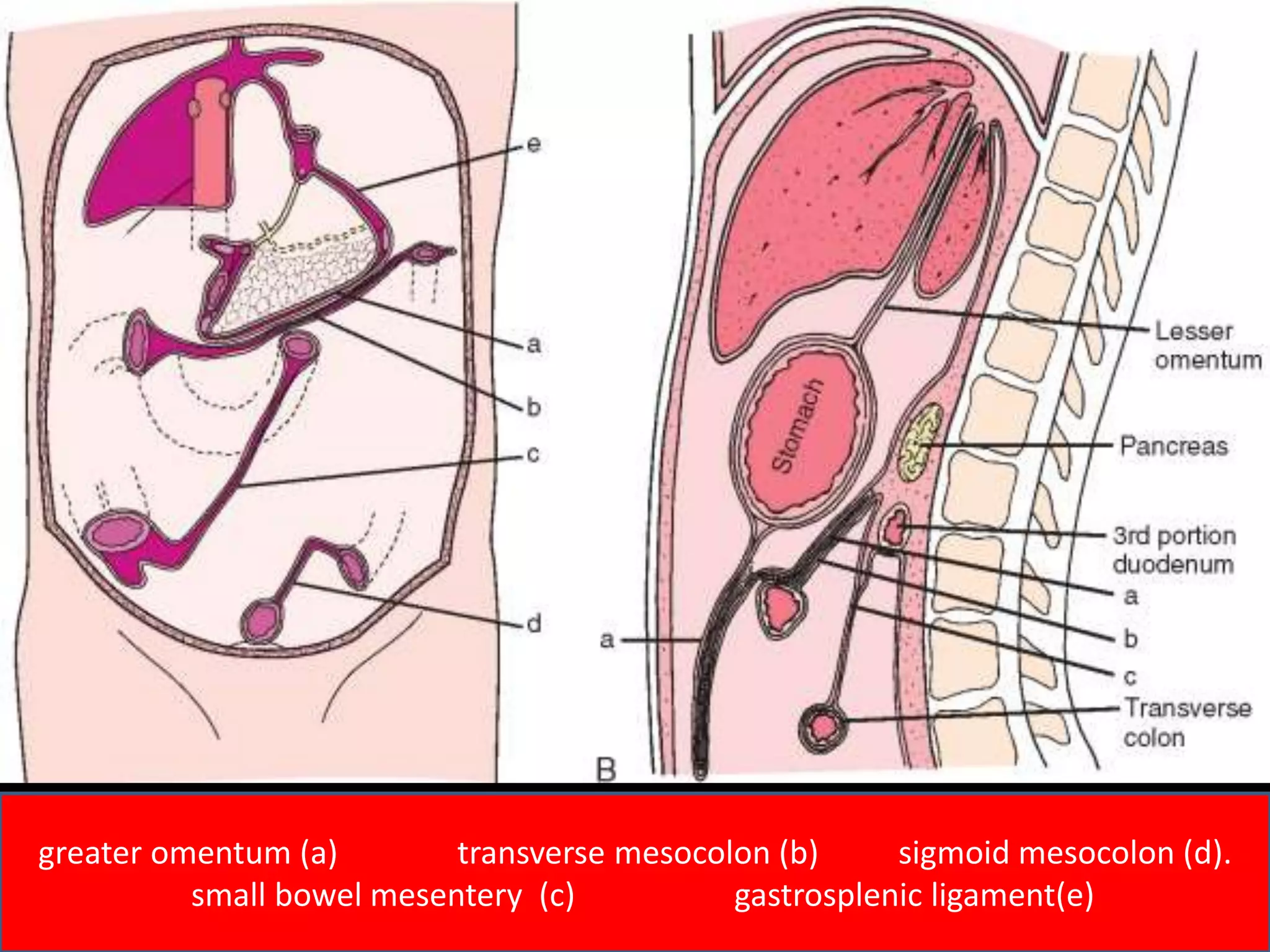
- The peritoneal cavity is divided by ligaments into the greater and lesser sacs
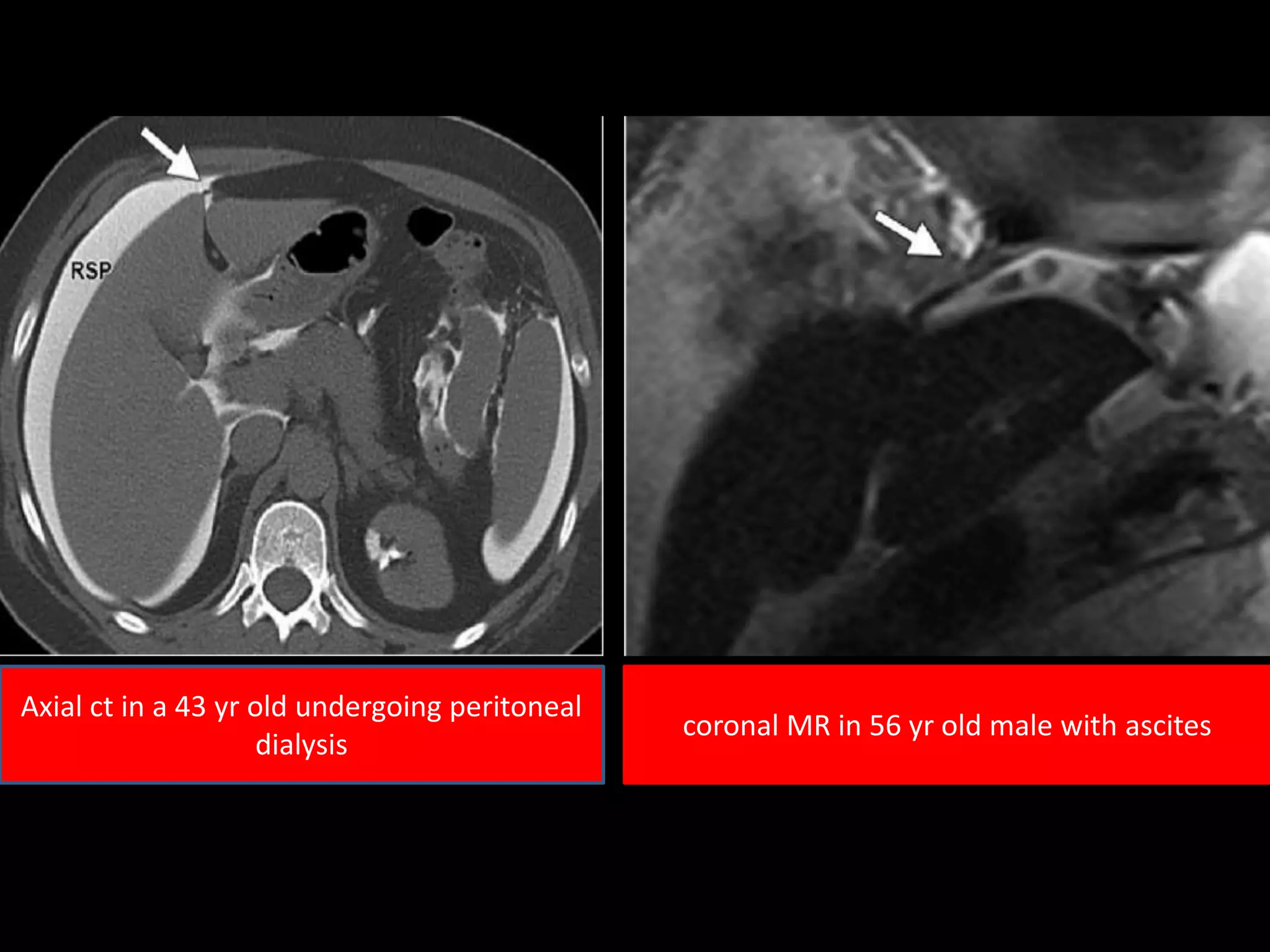
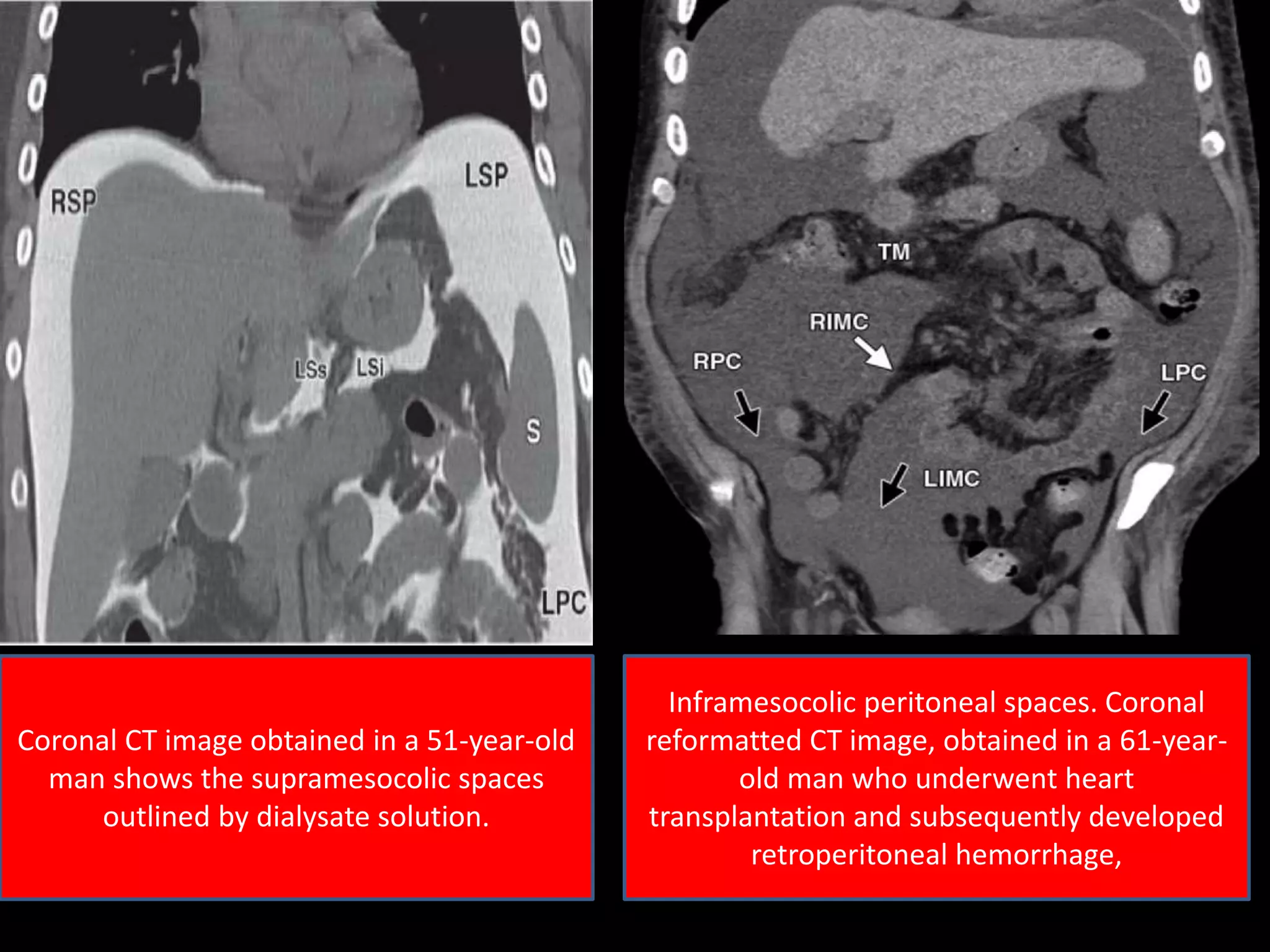
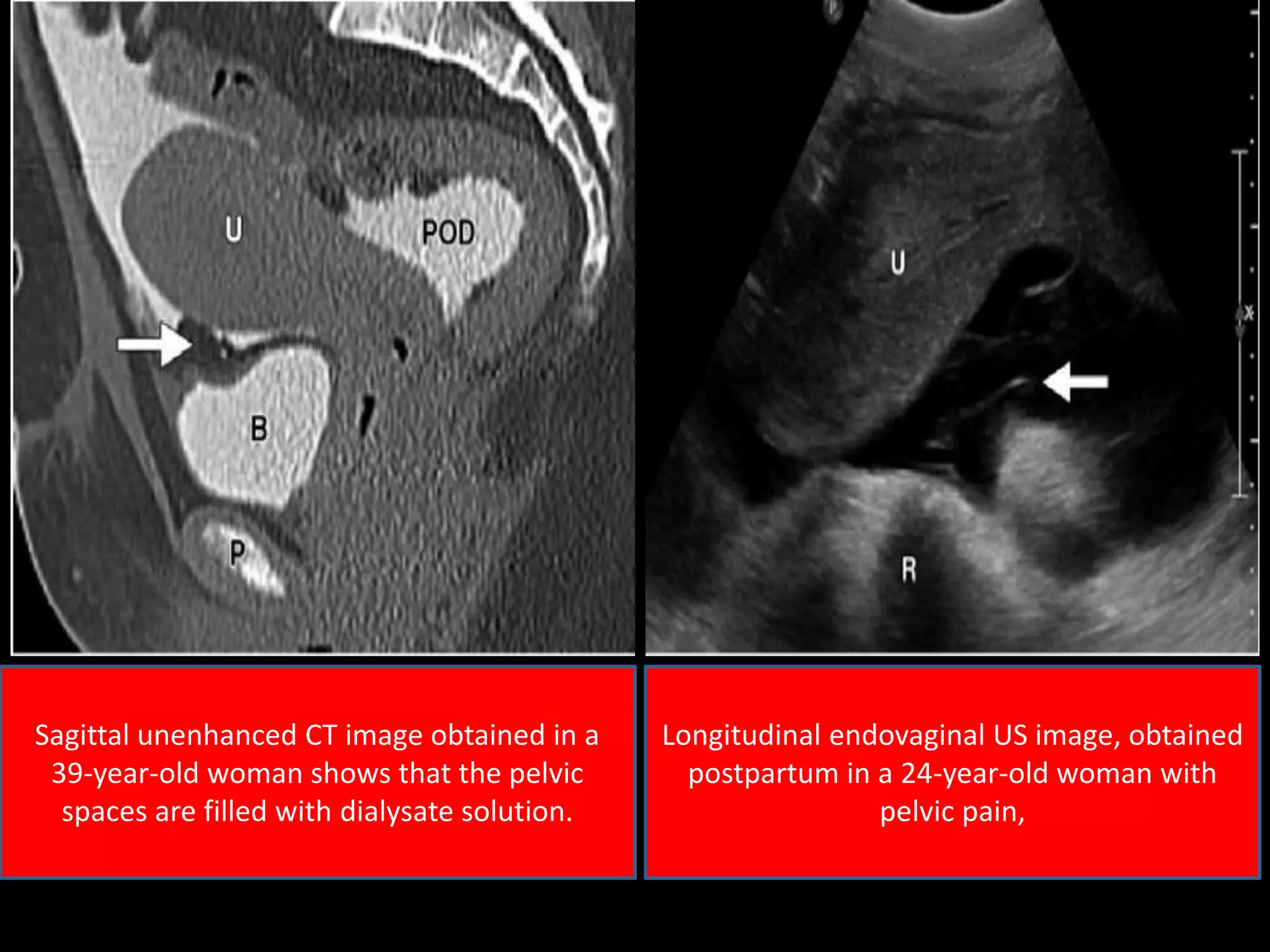
- Imaging modalities like CT are commonly used to evaluate peritoneal spaces
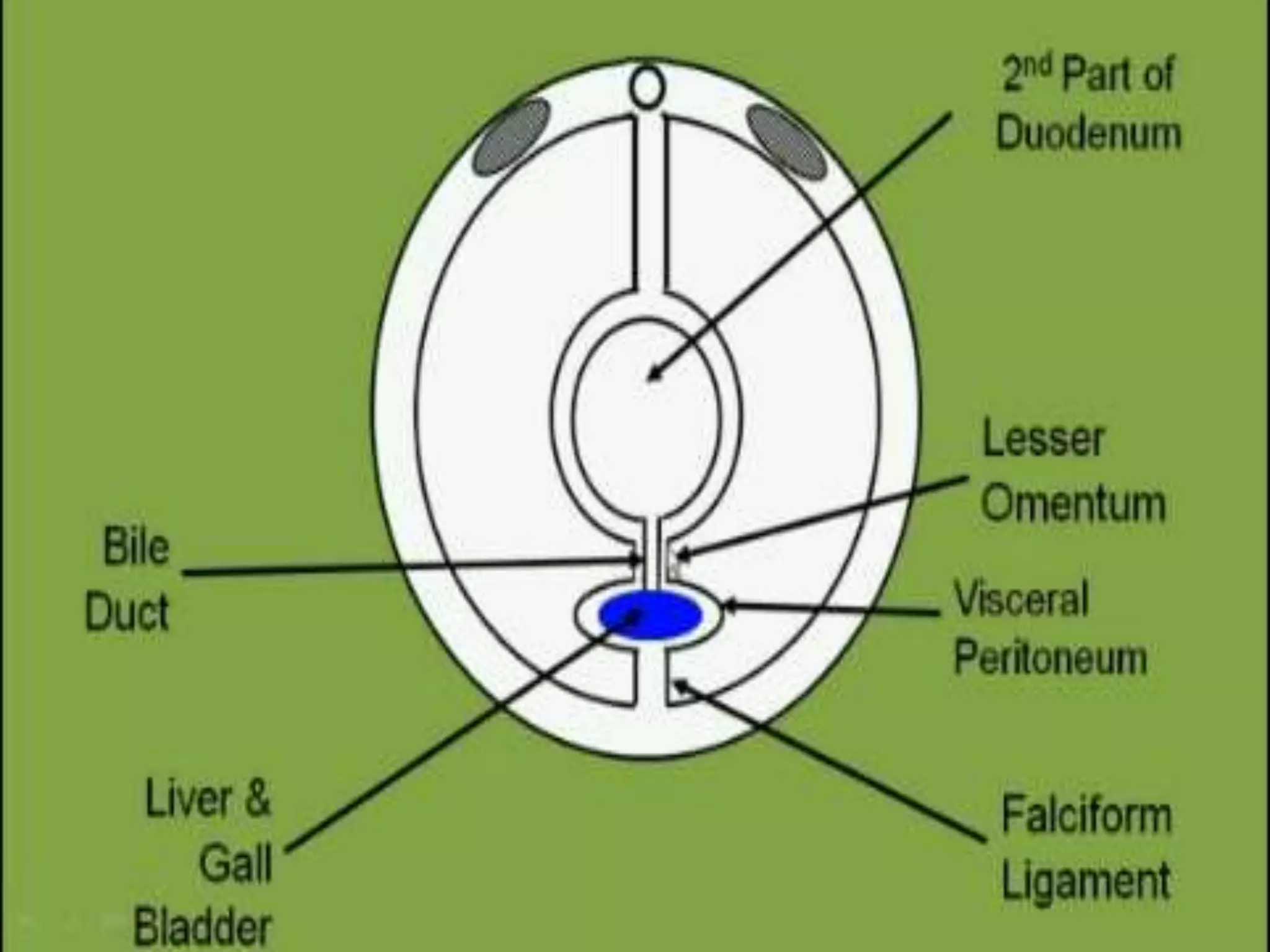
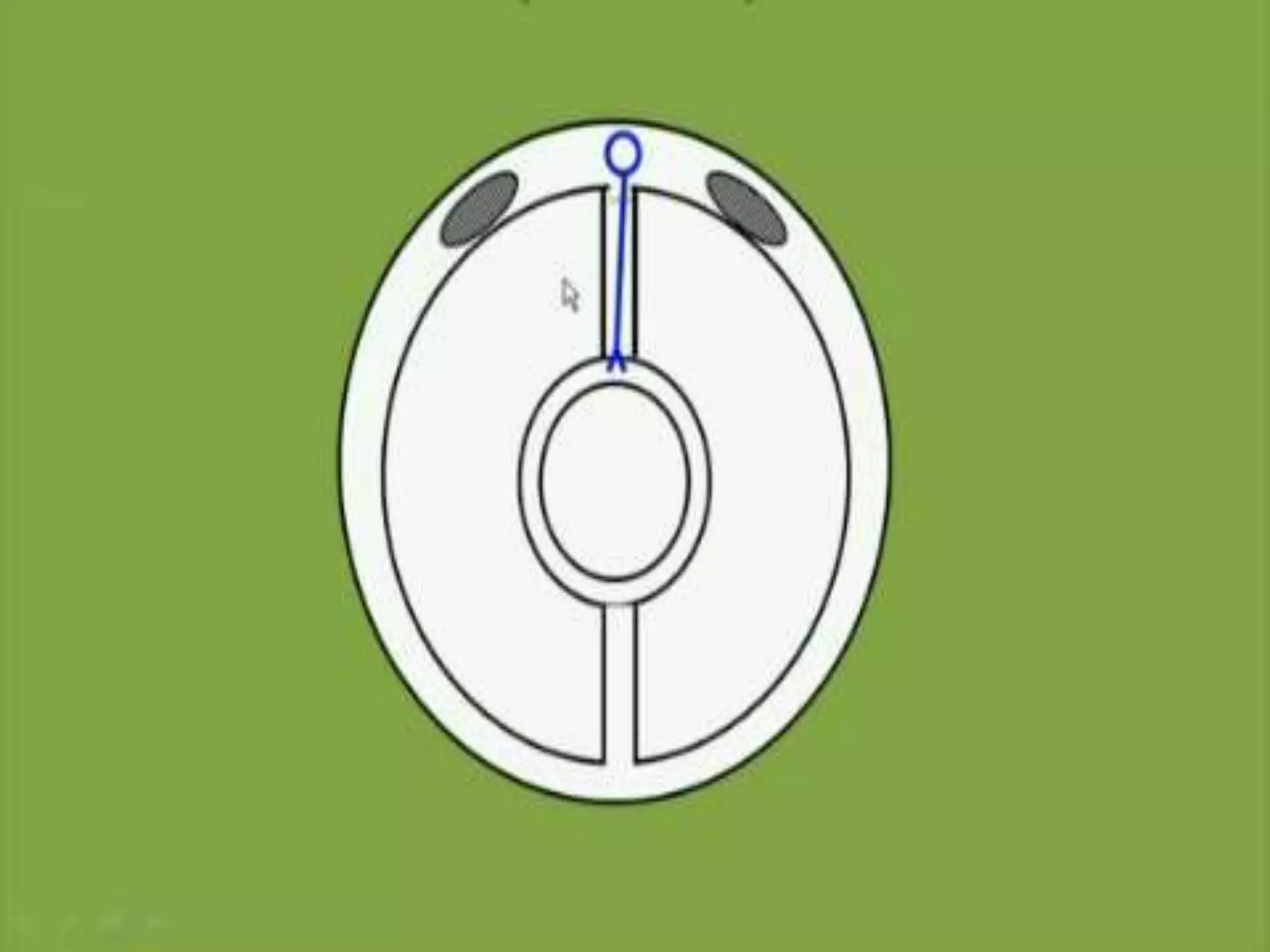
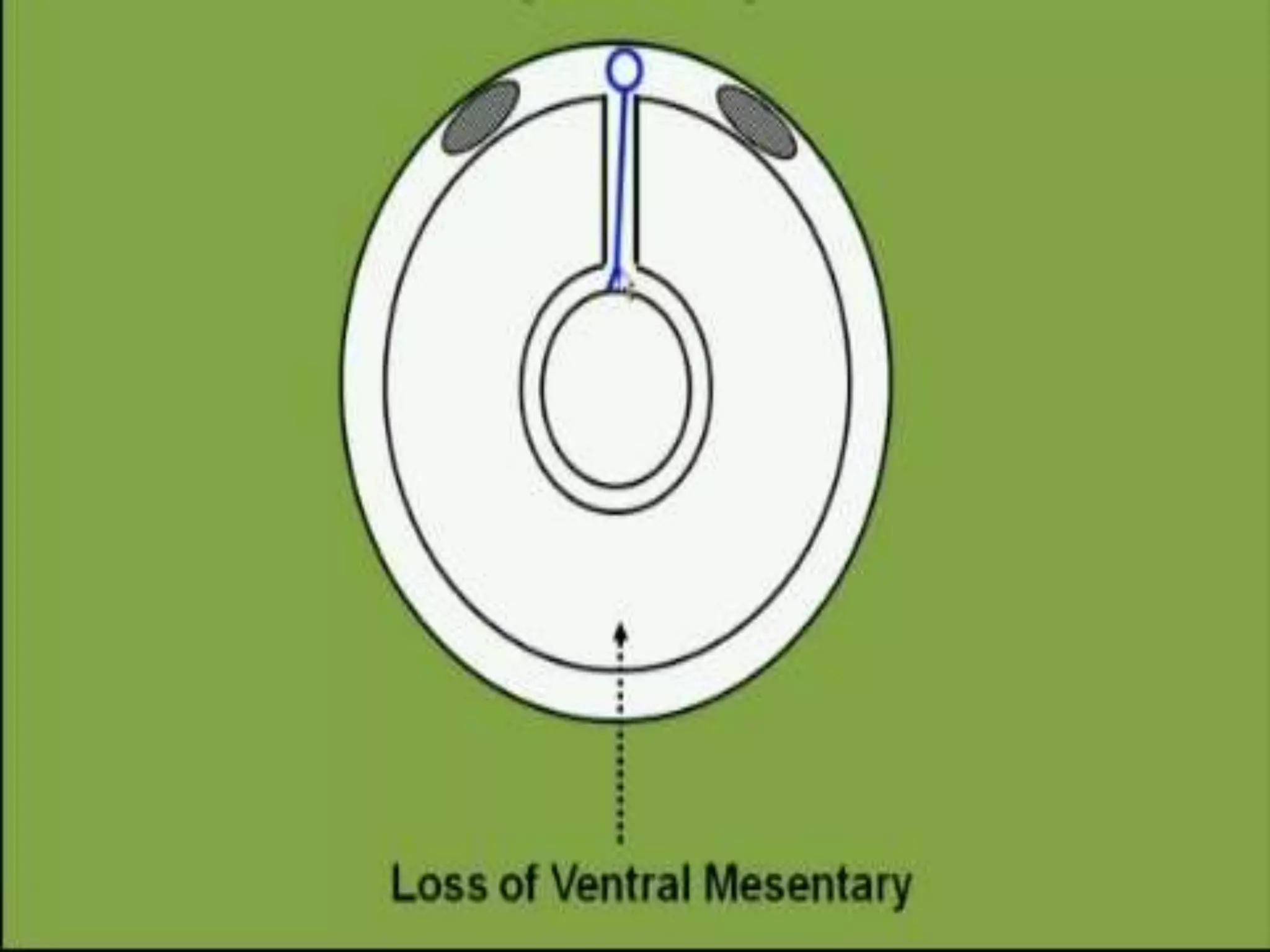
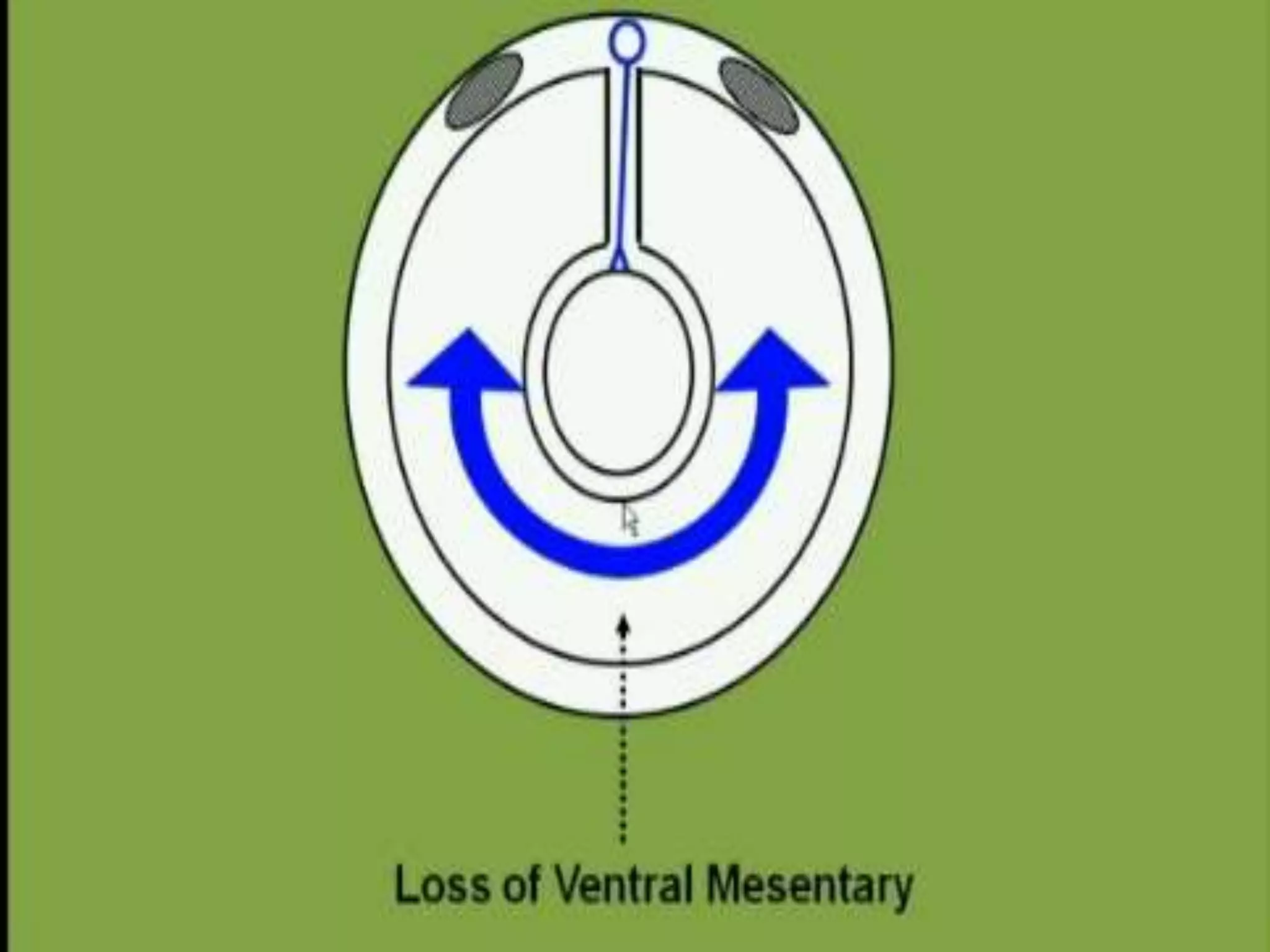
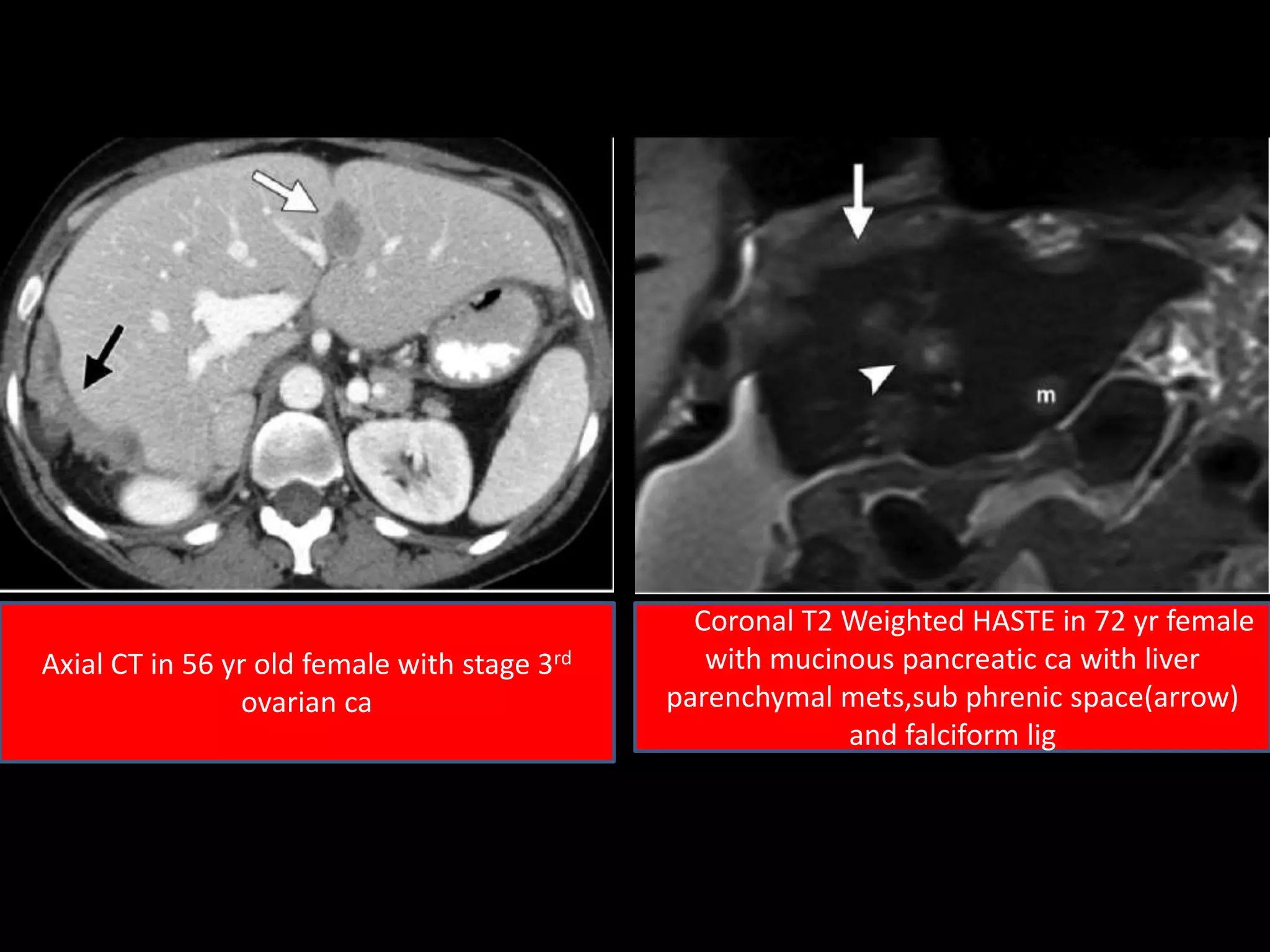
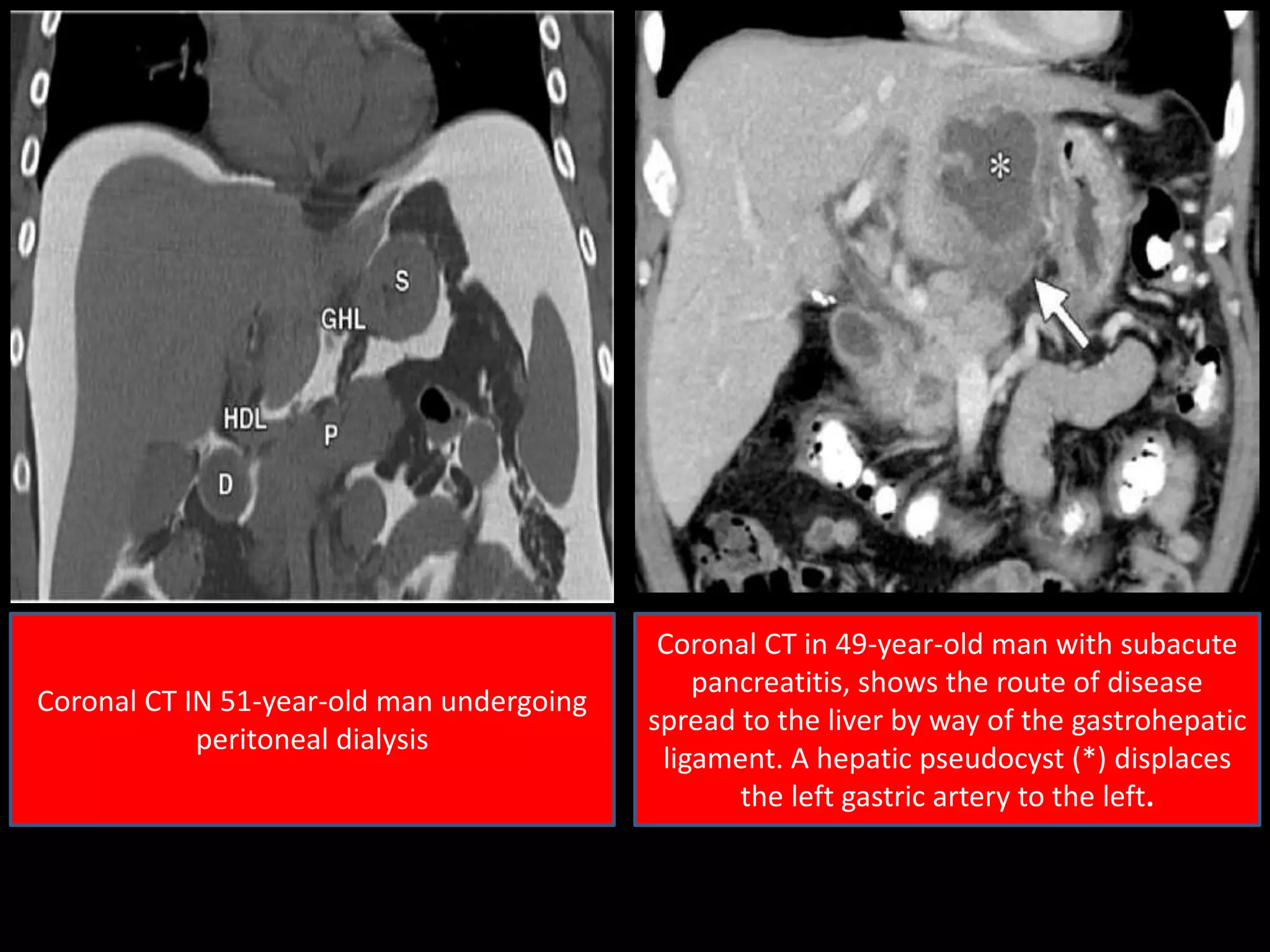
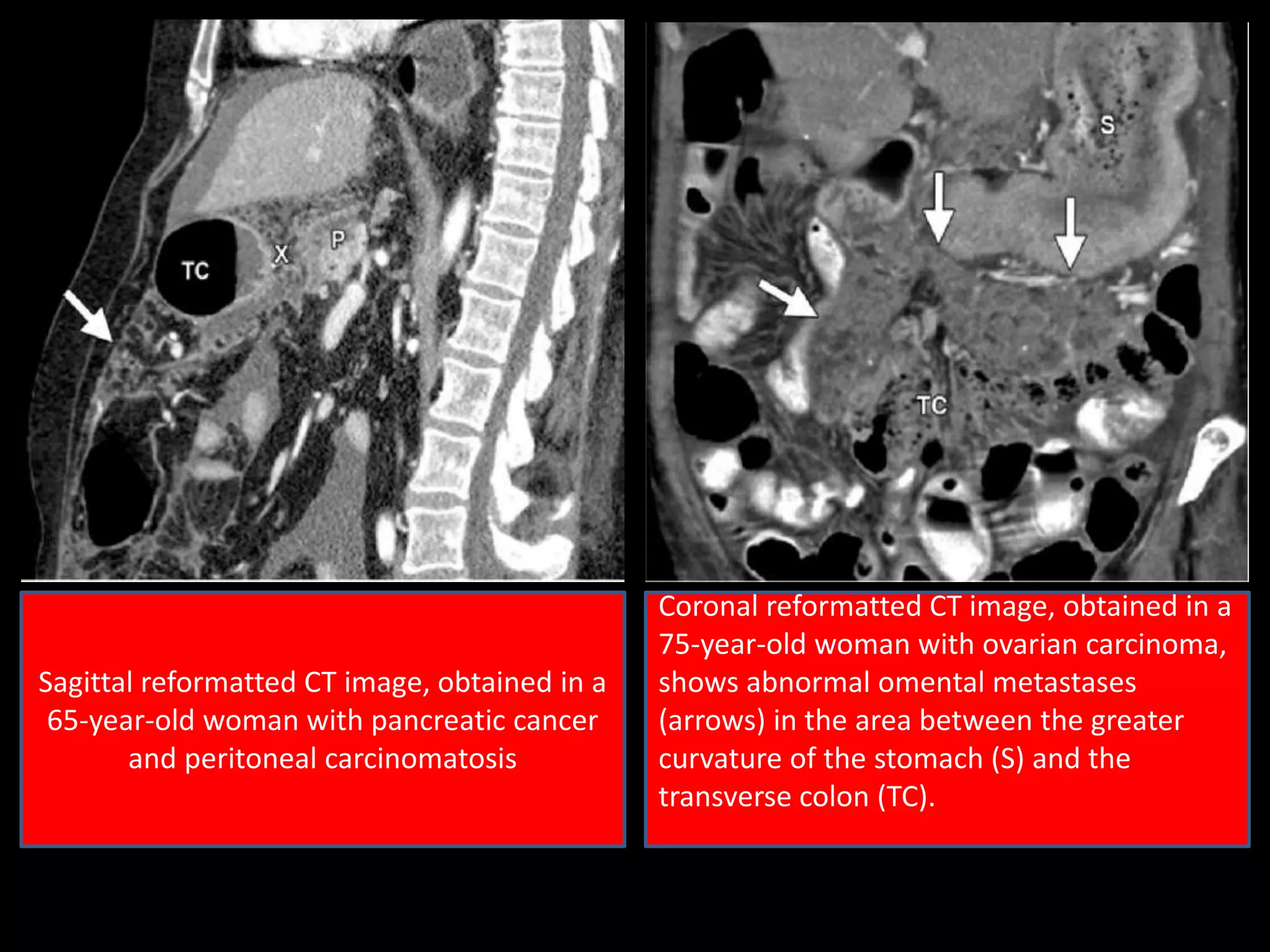
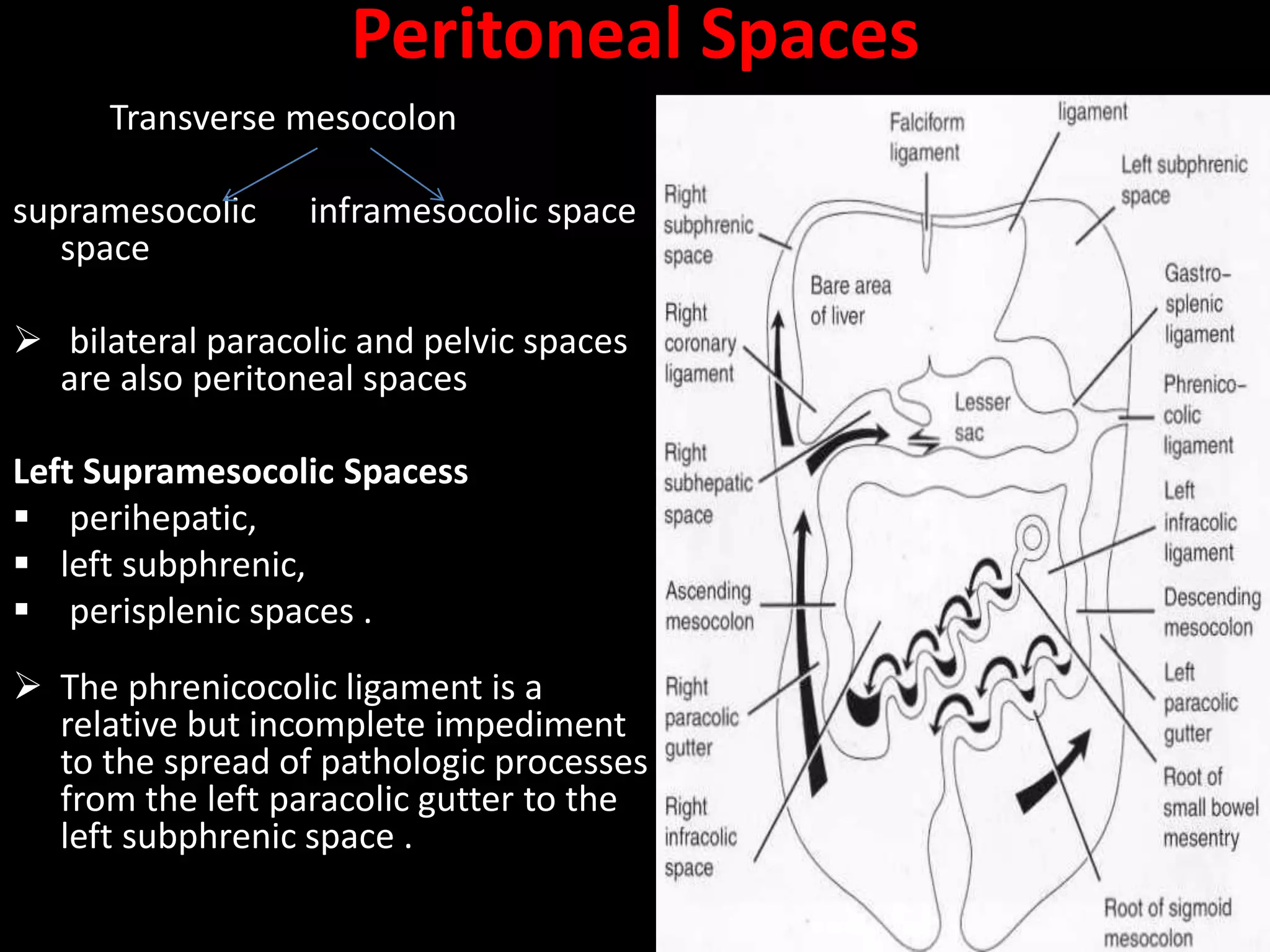
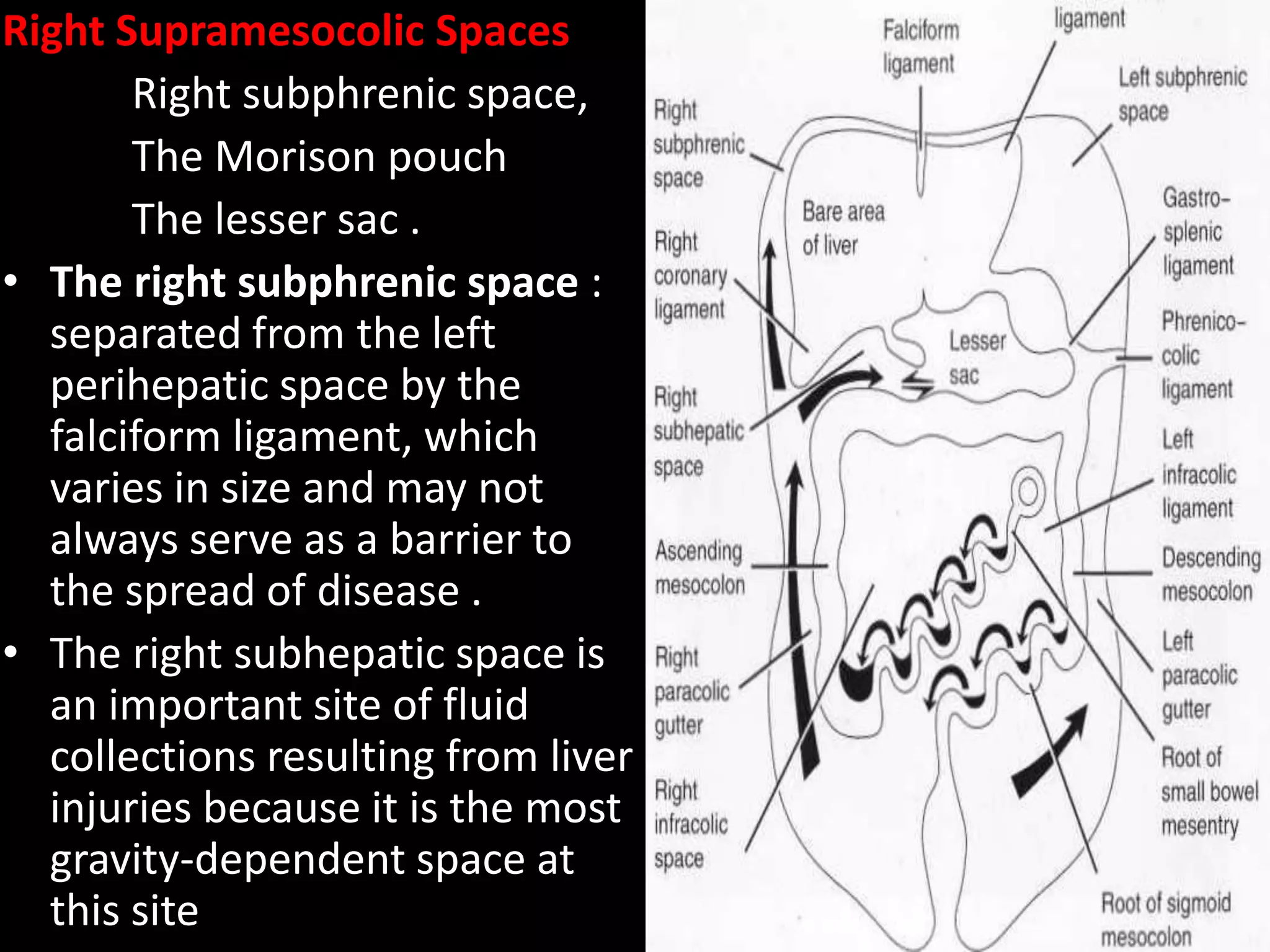
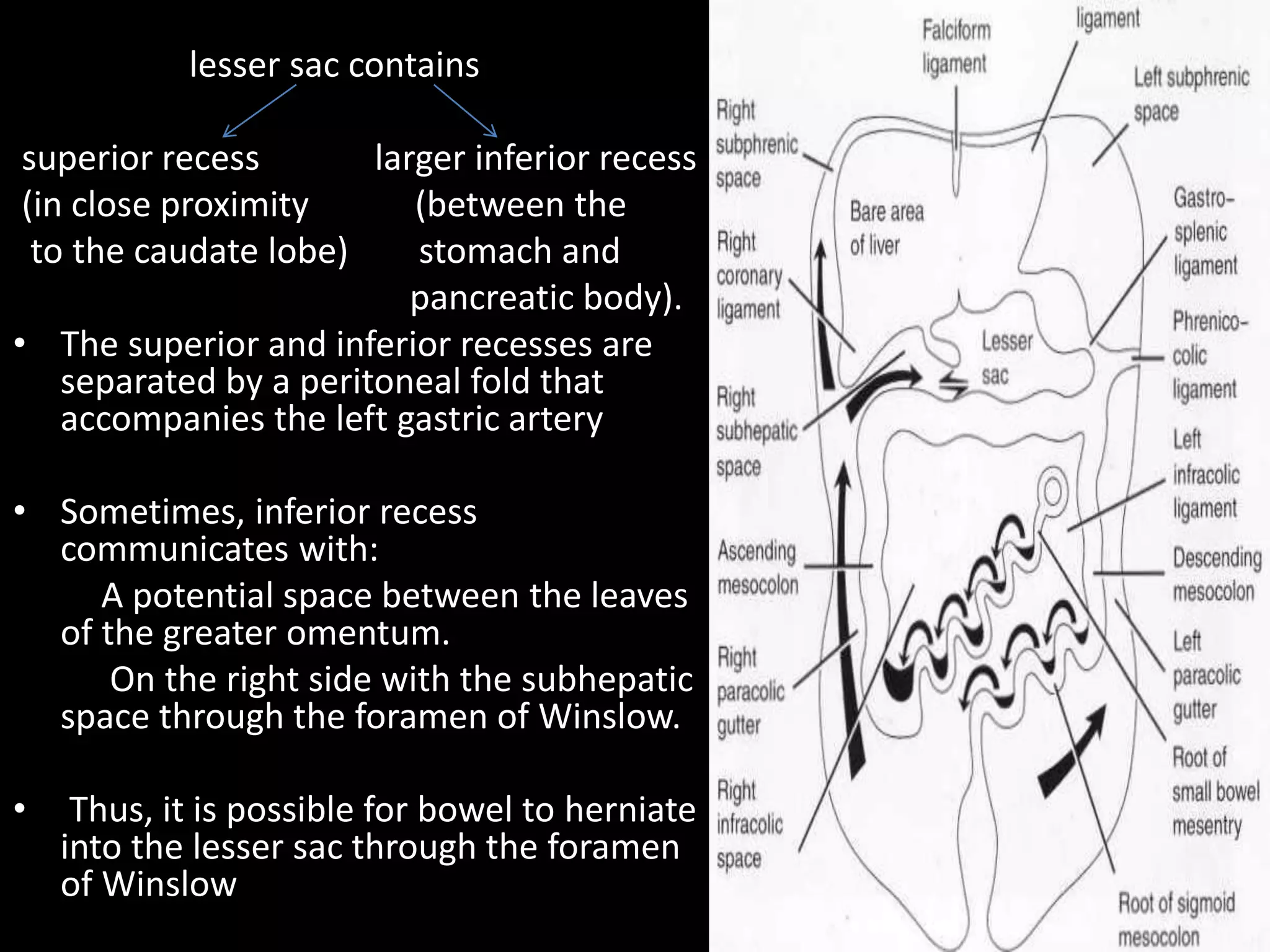
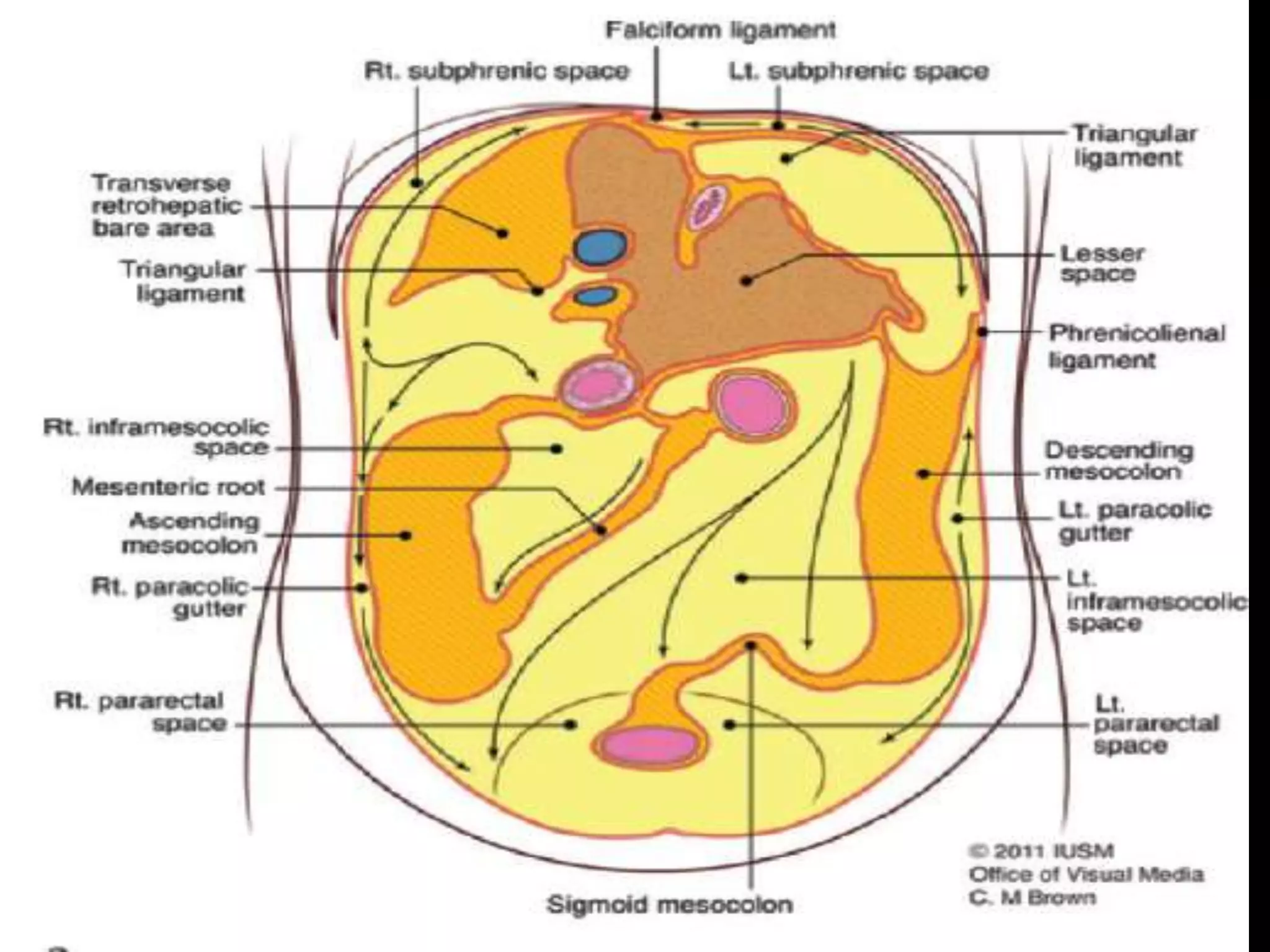
- Various peritoneal ligaments like the falciform ligament divide spaces in the abdomen
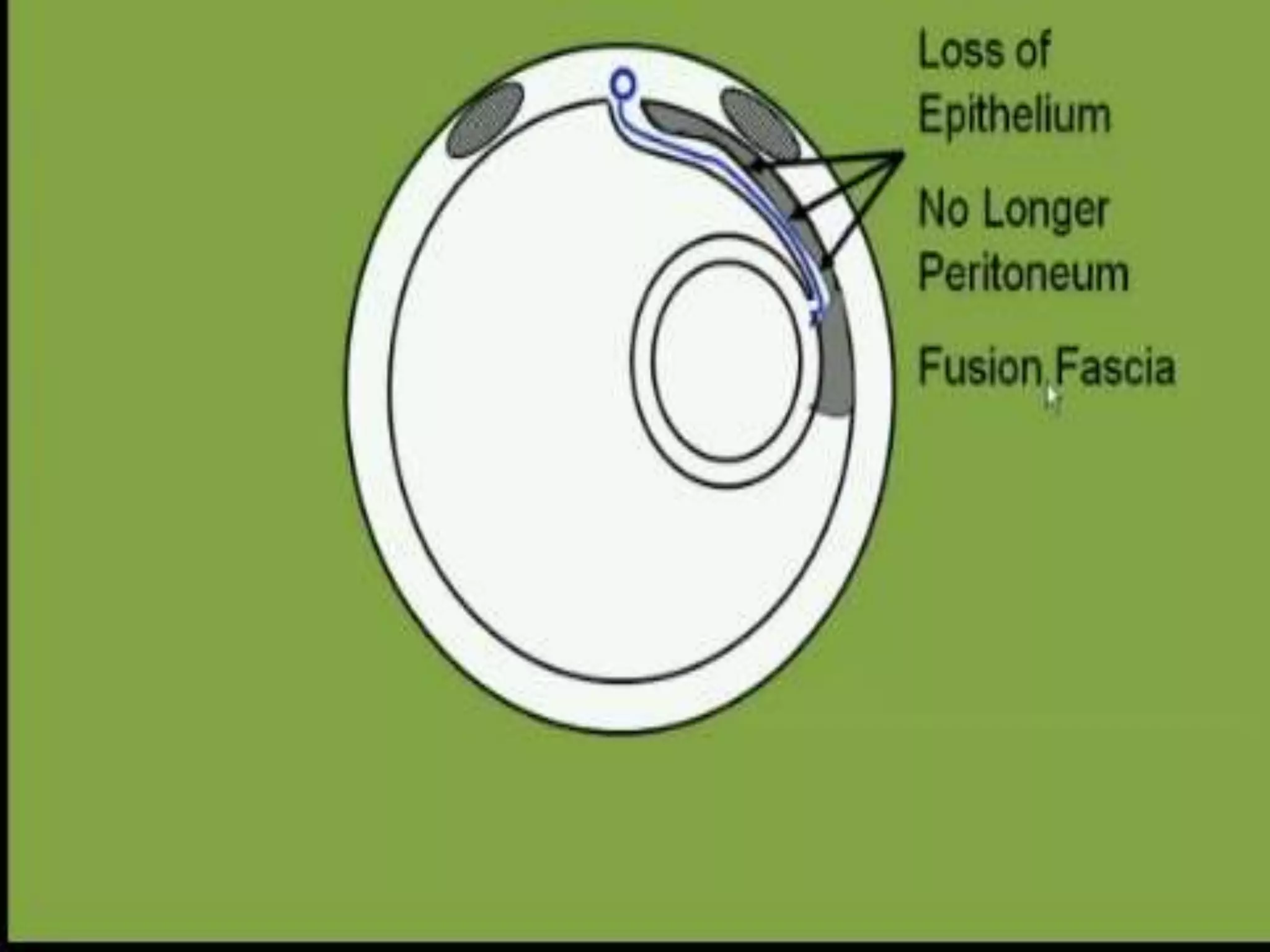
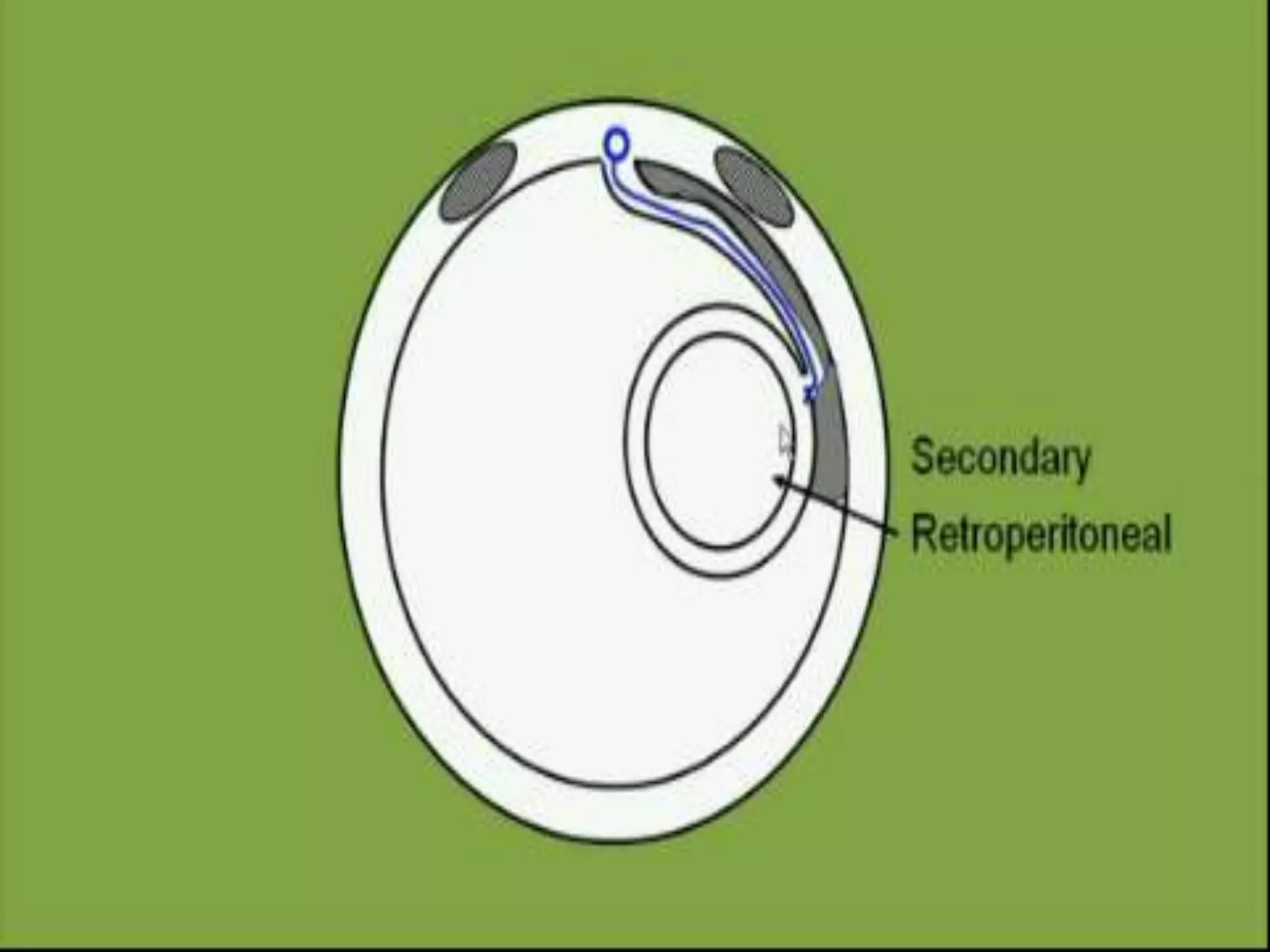
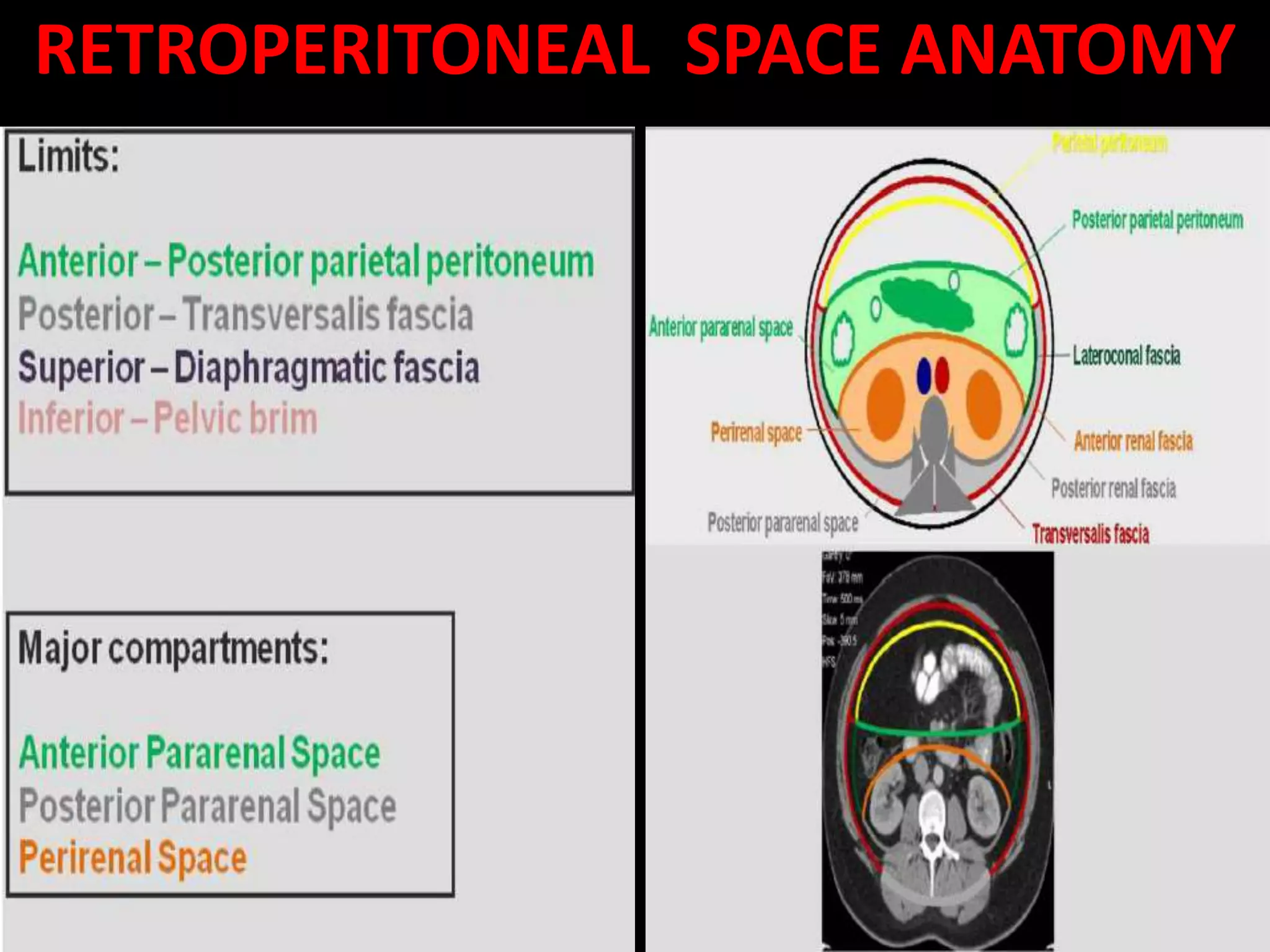
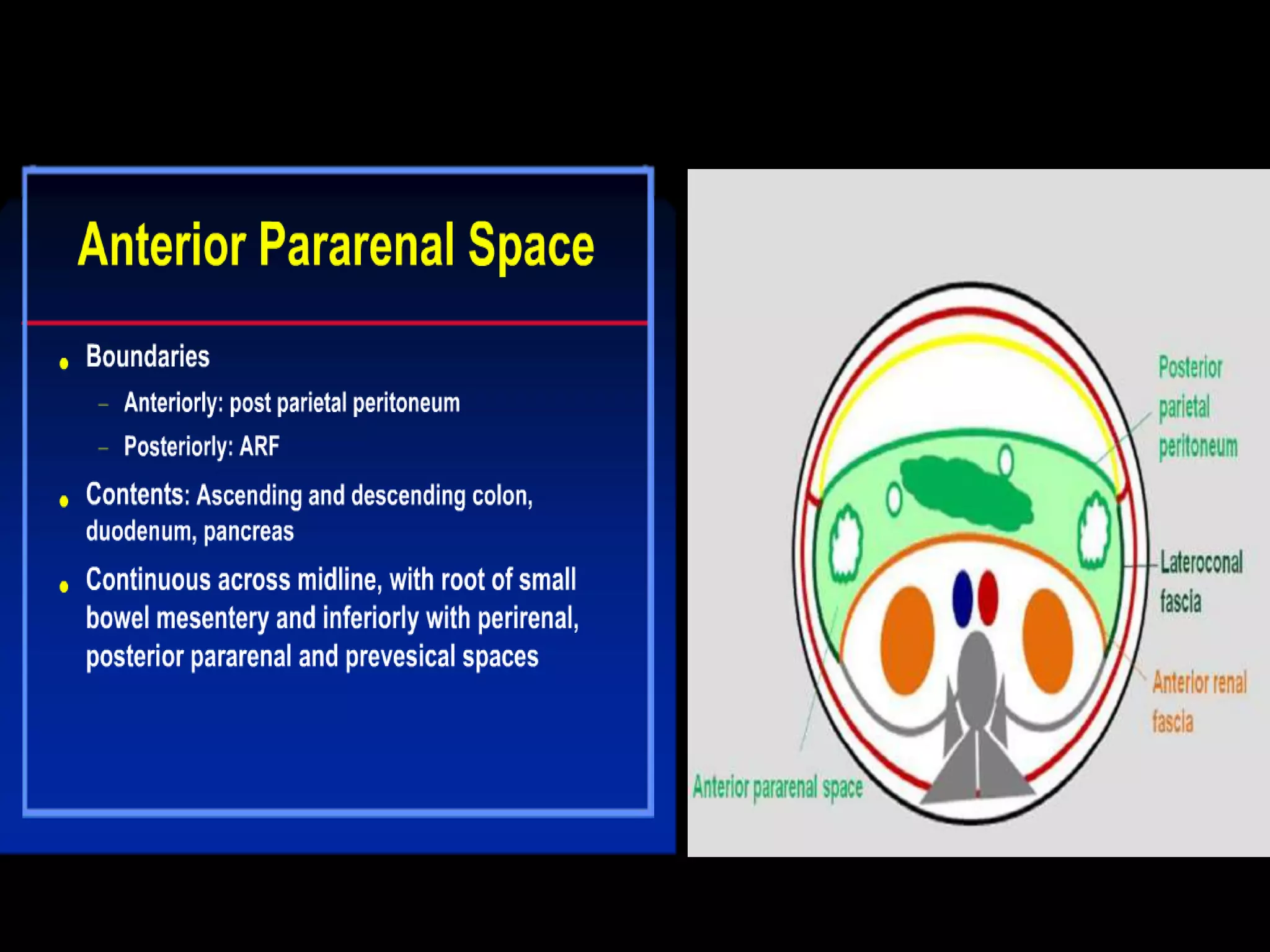
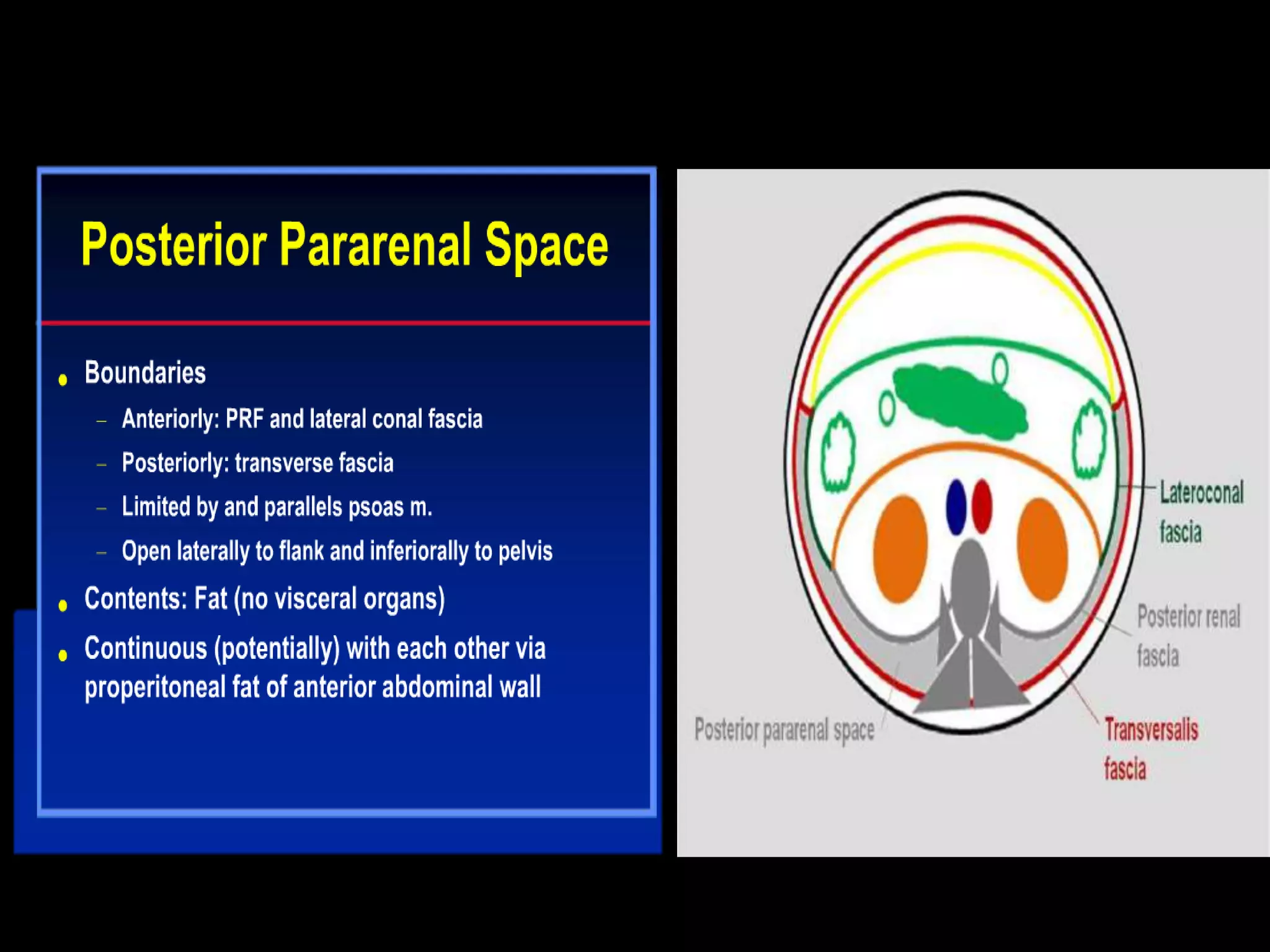
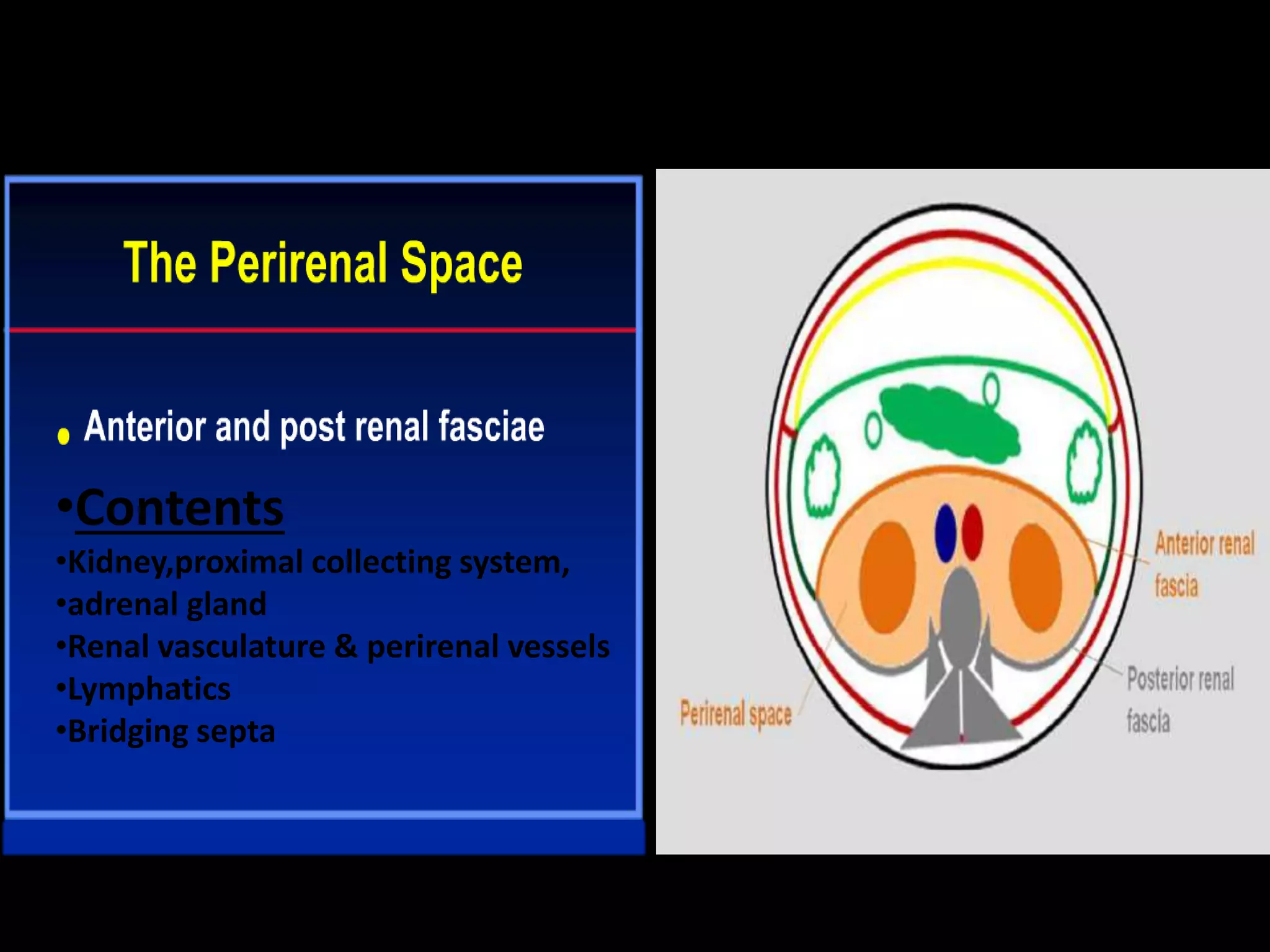
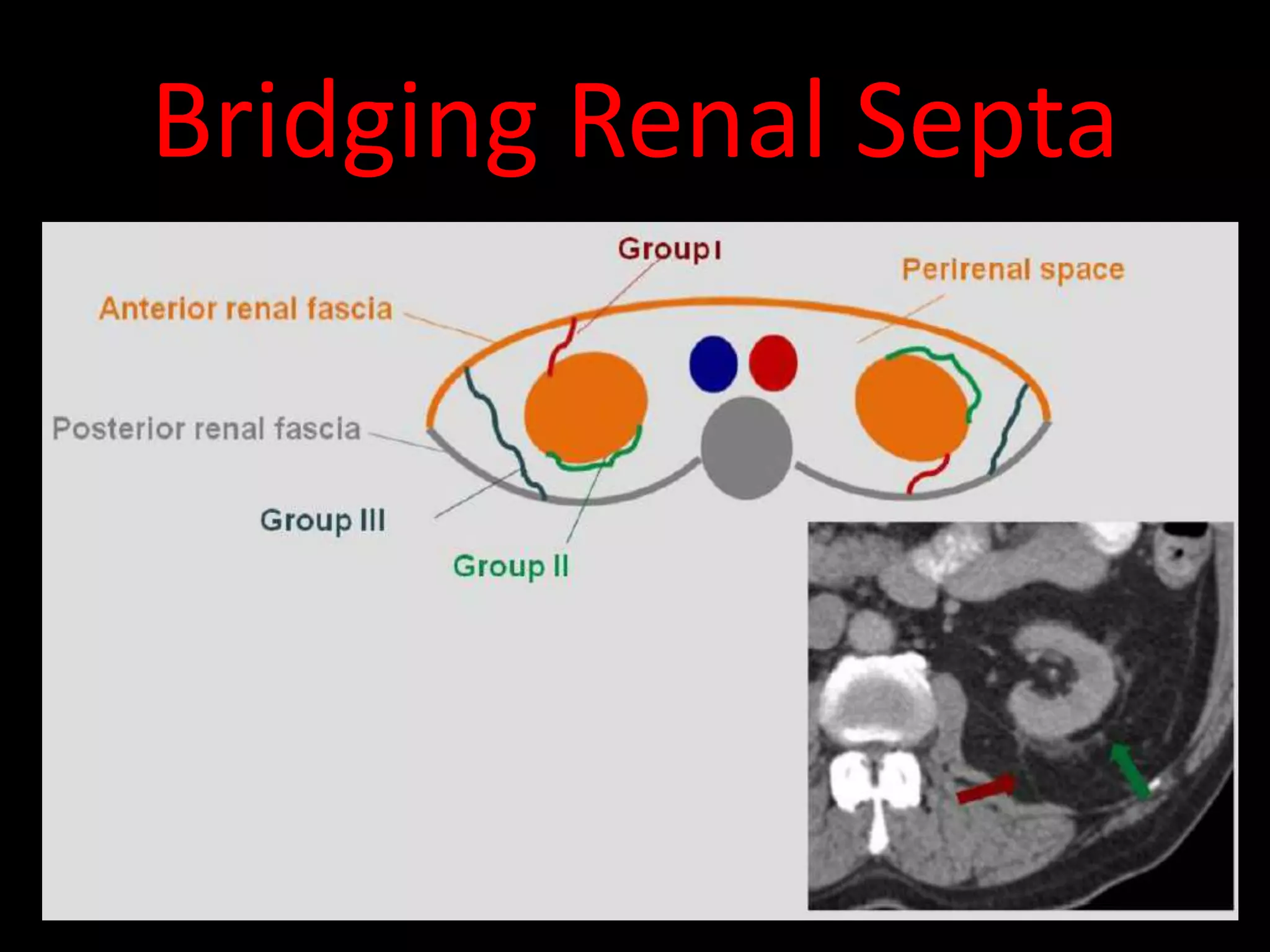
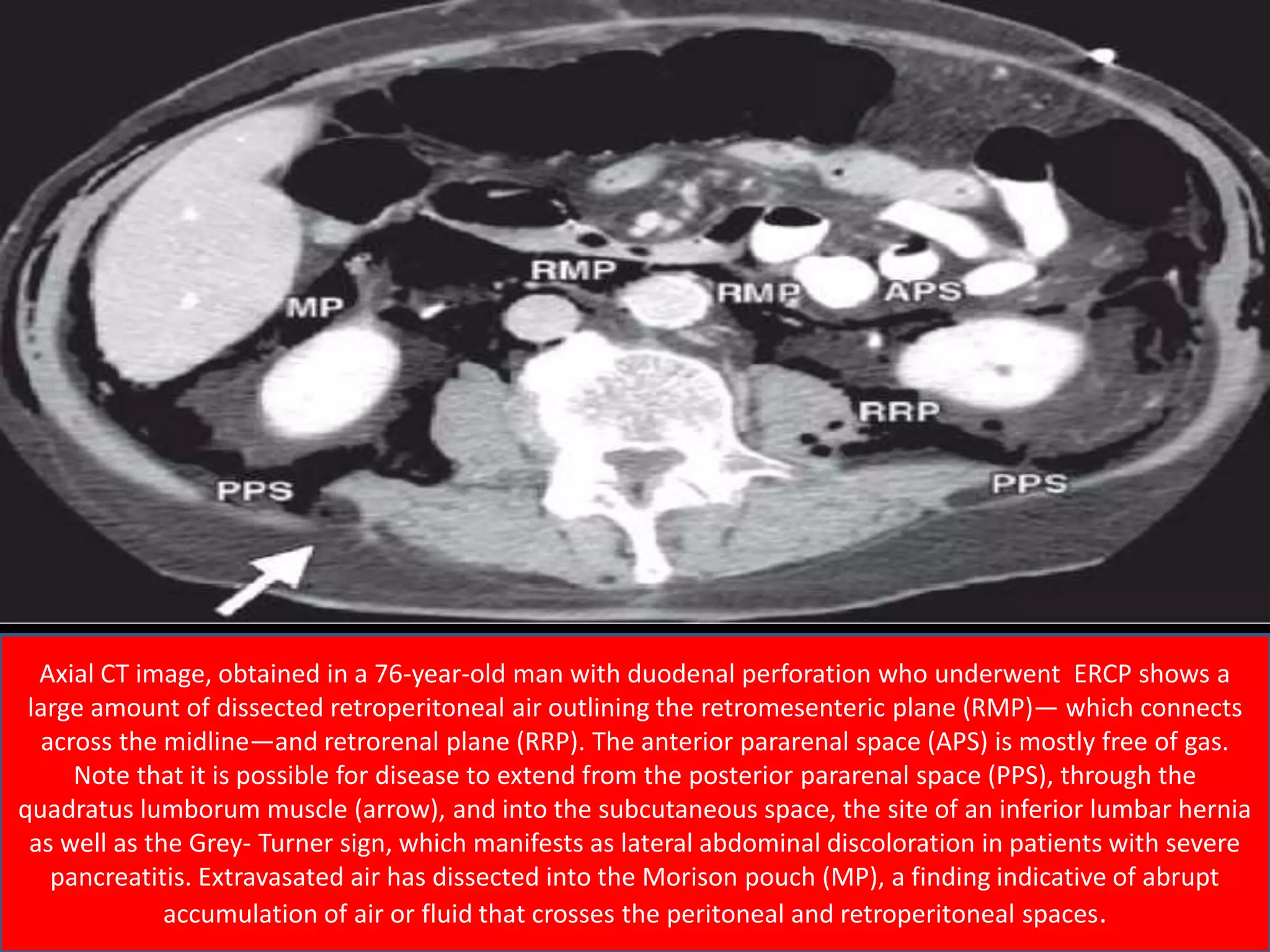
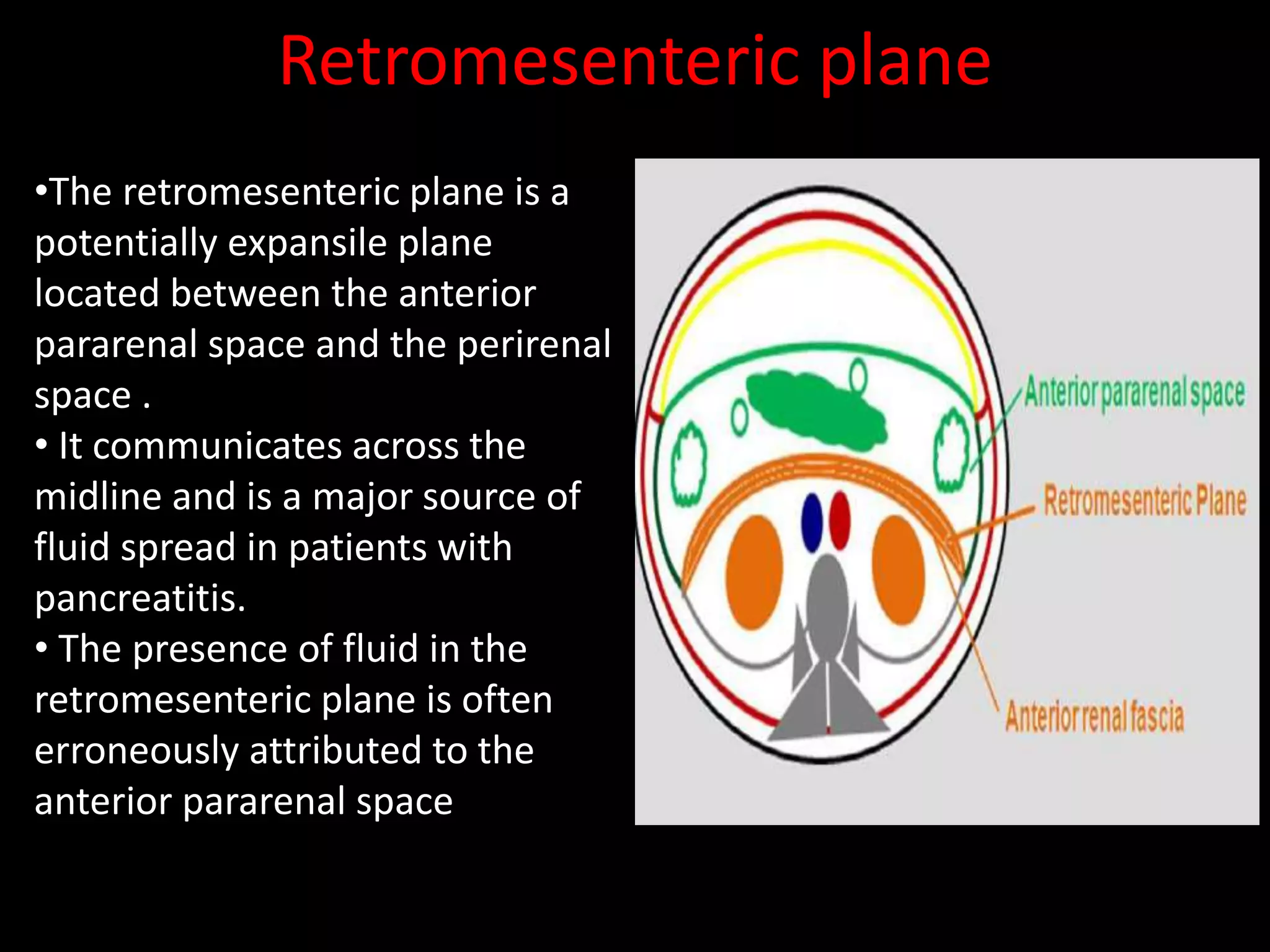
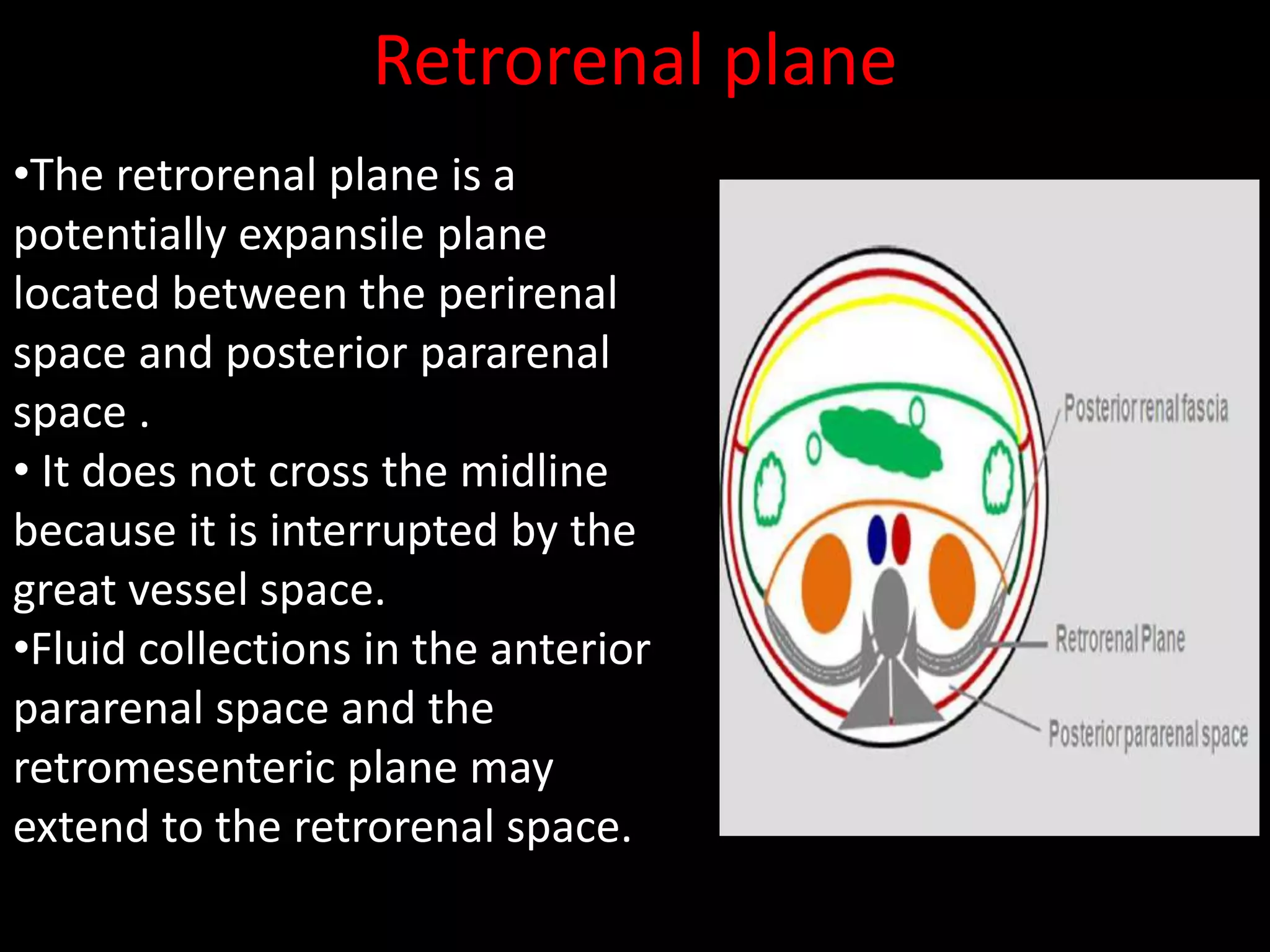
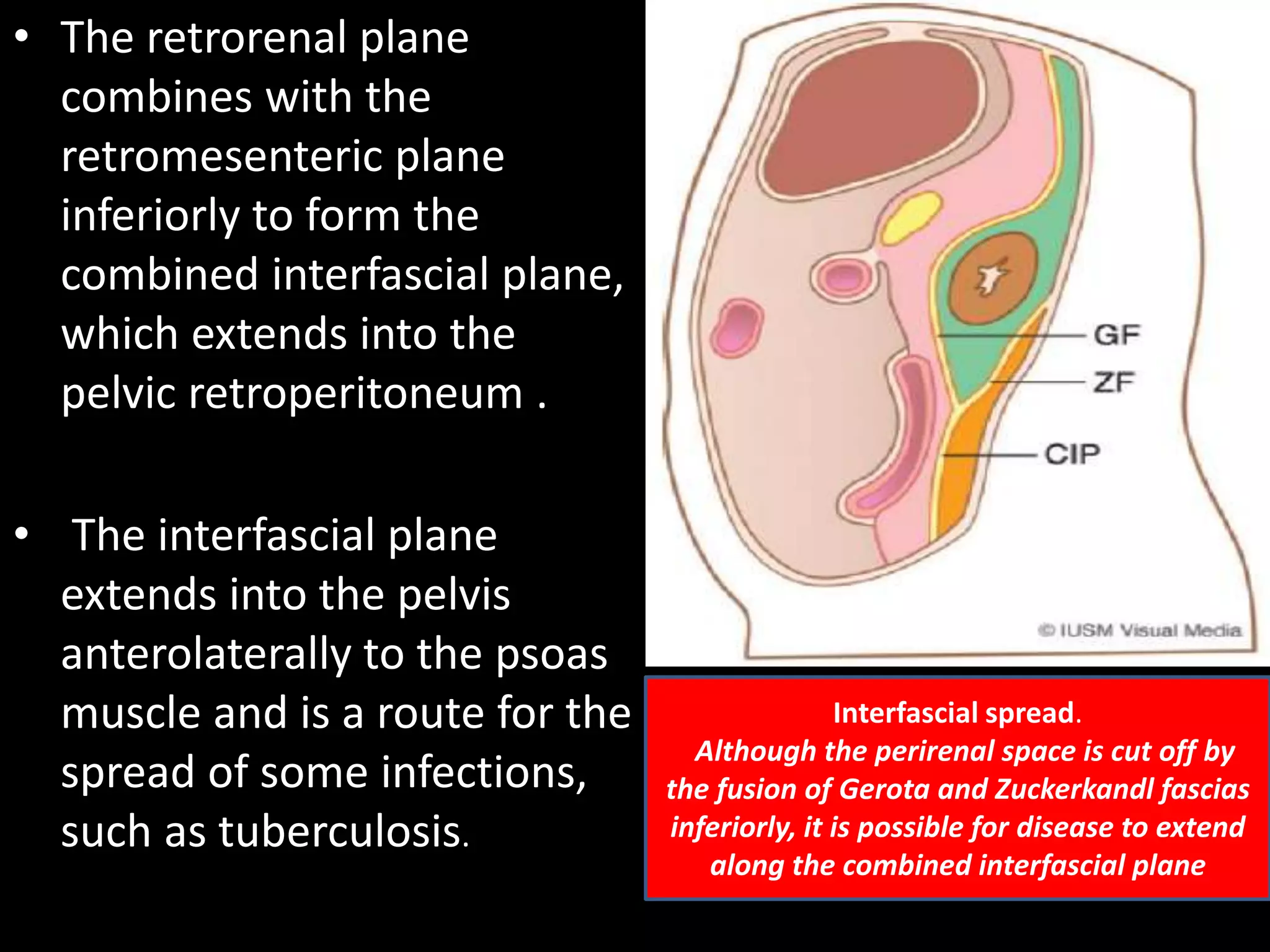
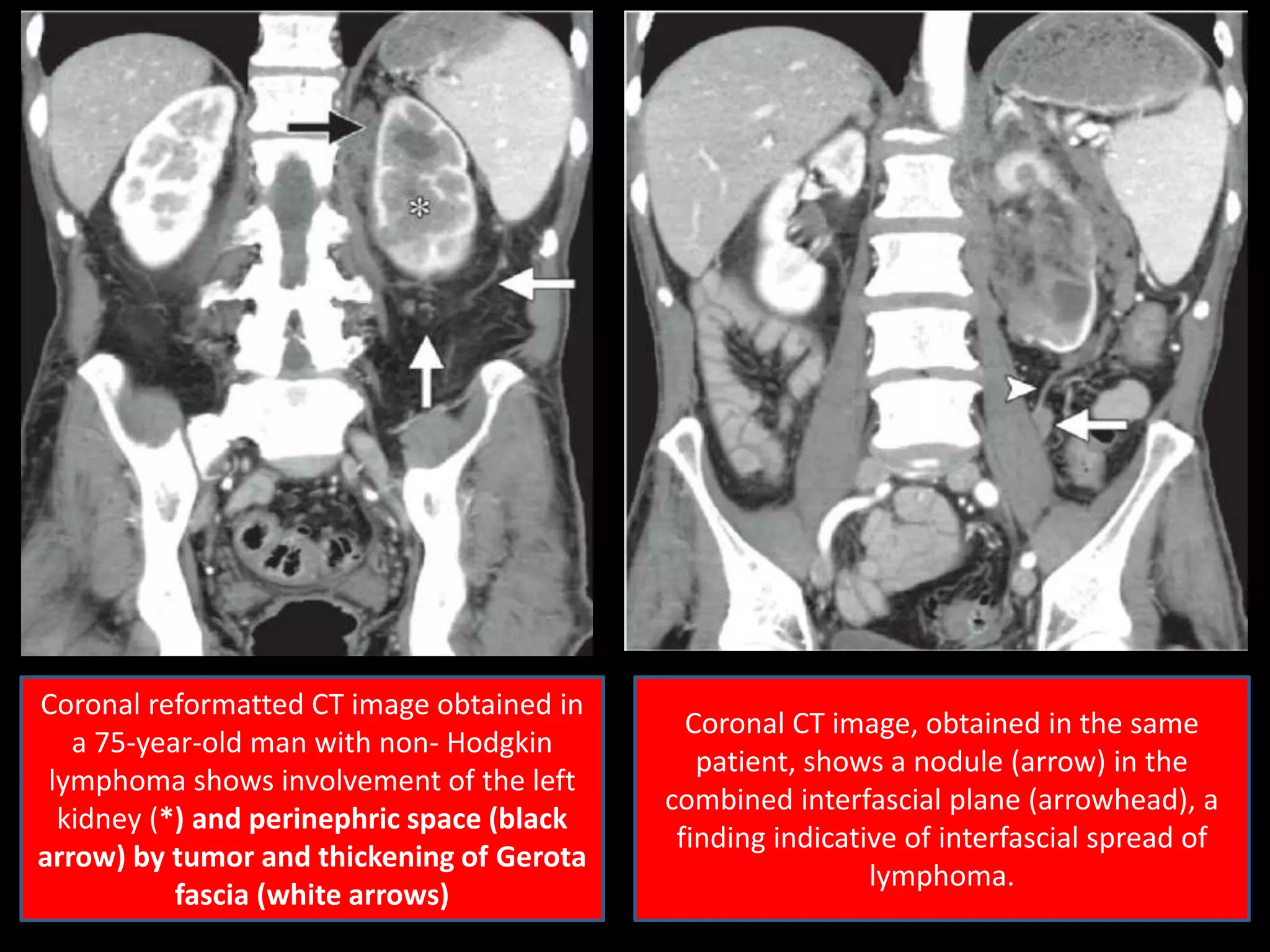
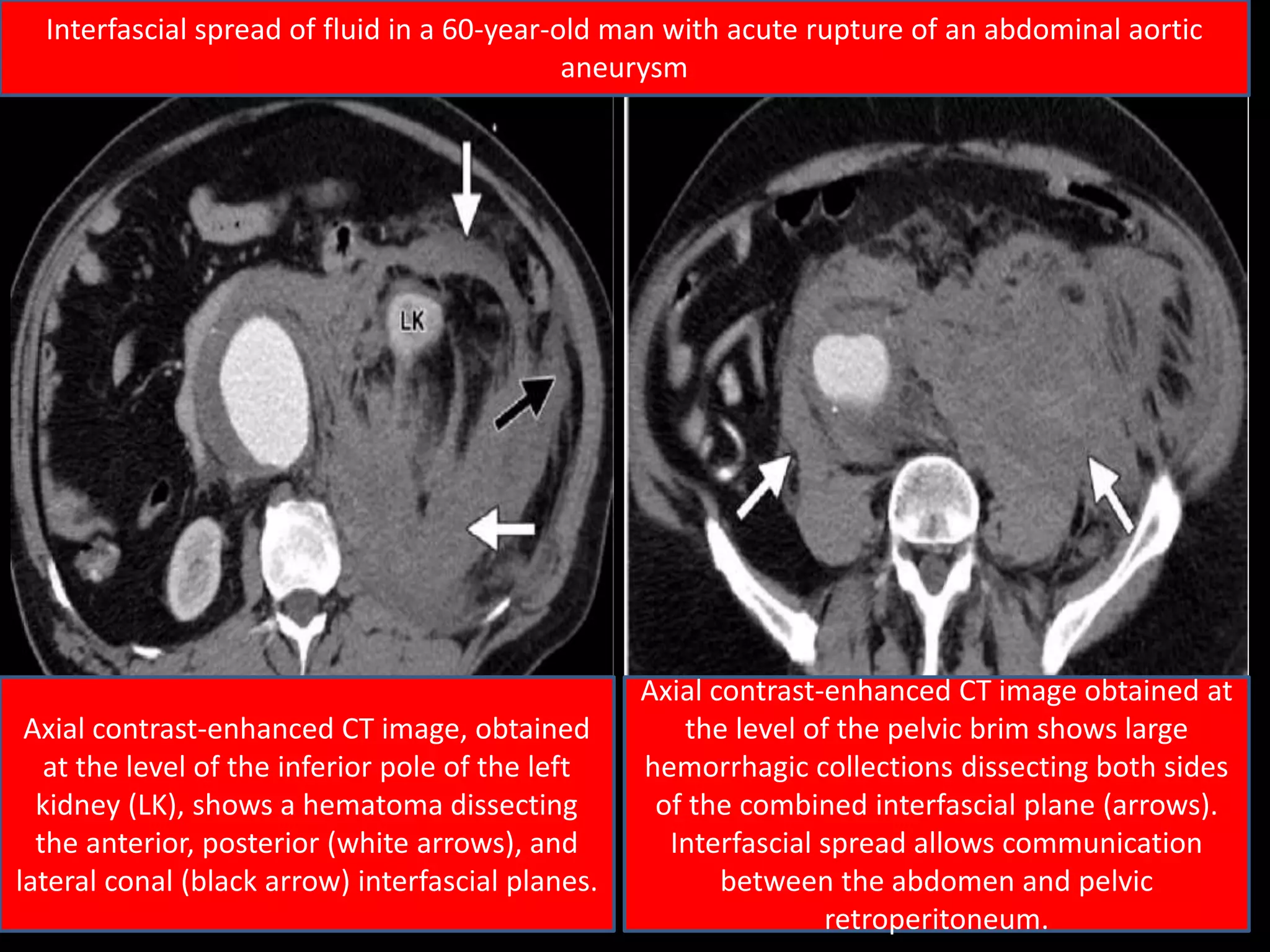
- Disease can spread along fascial planes between retroperitoneal spaces
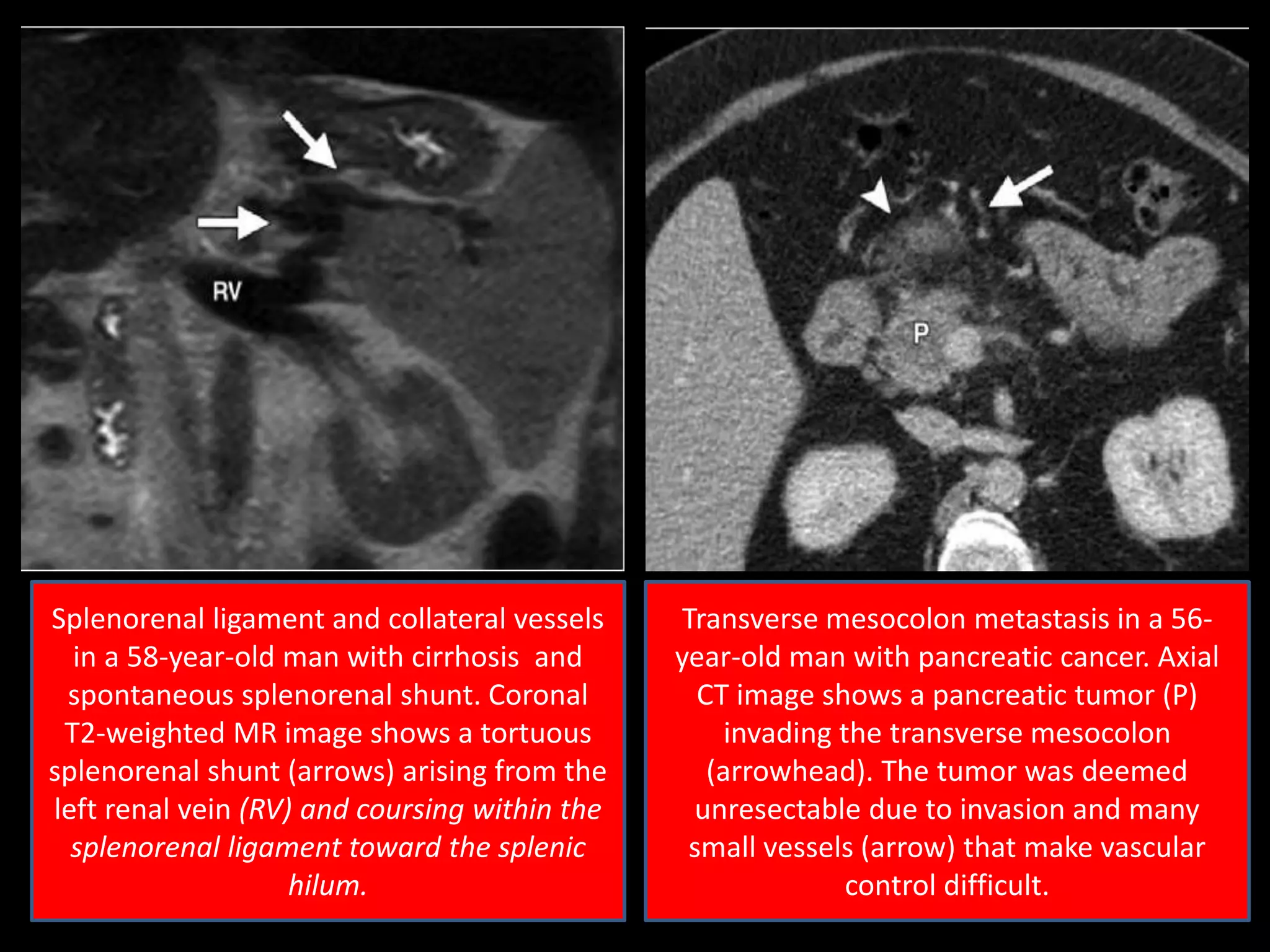
The document then proceeds to describe individual peritoneal spaces, ligaments, fascial planes and provides examples of their imaging appearance when involved by disease processes.