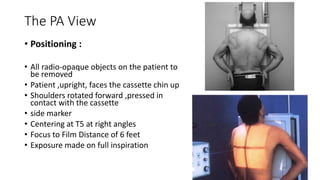
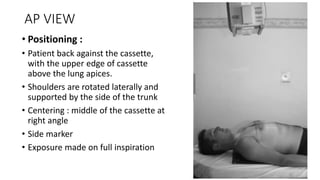
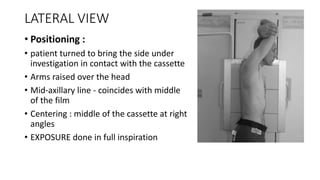
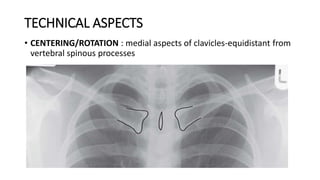
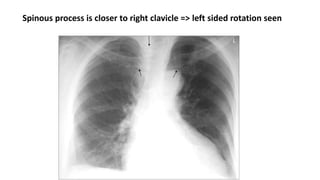
- The document describes the positioning and technical aspects of performing a normal chest x-ray. It discusses the positioning of the patient for PA, AP, and lateral views. It also describes how to assess the quality of the x-ray image and what structures to evaluate, including the bones, heart, lungs, diaphragm and soft tissues. Anatomical variations are also discussed. The goal of the chest x-ray is to evaluate the lungs, heart, bones, and soft tissues for any abnormalities.