Downloaded 859 times
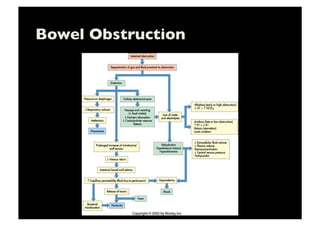

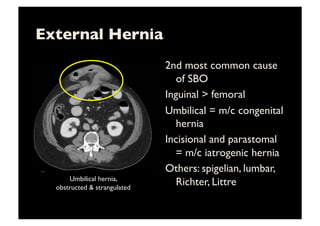
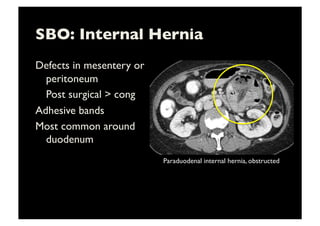
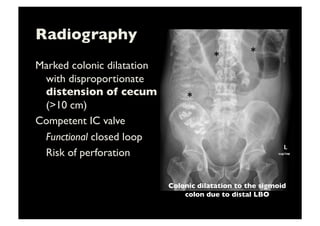
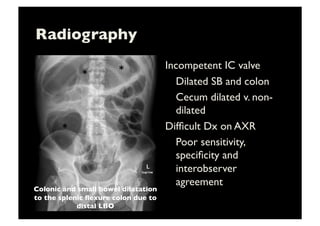
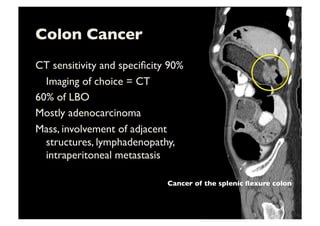


This document discusses imaging techniques for evaluating bowel obstruction, including radiography and CT. It covers the clinical presentation, imaging features, and causes of gastric, small bowel, and large bowel obstruction. Key points include using CT to identify the location and cause of obstruction, assess for complications like strangulation or closed loop obstruction that may require emergent surgery. The most common causes of small bowel obstruction are adhesions, hernias, and malignancies, while large bowel obstruction is usually due to malignancy, volvulus, or diverticulitis in older patients.




























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




