Downloaded 715 times

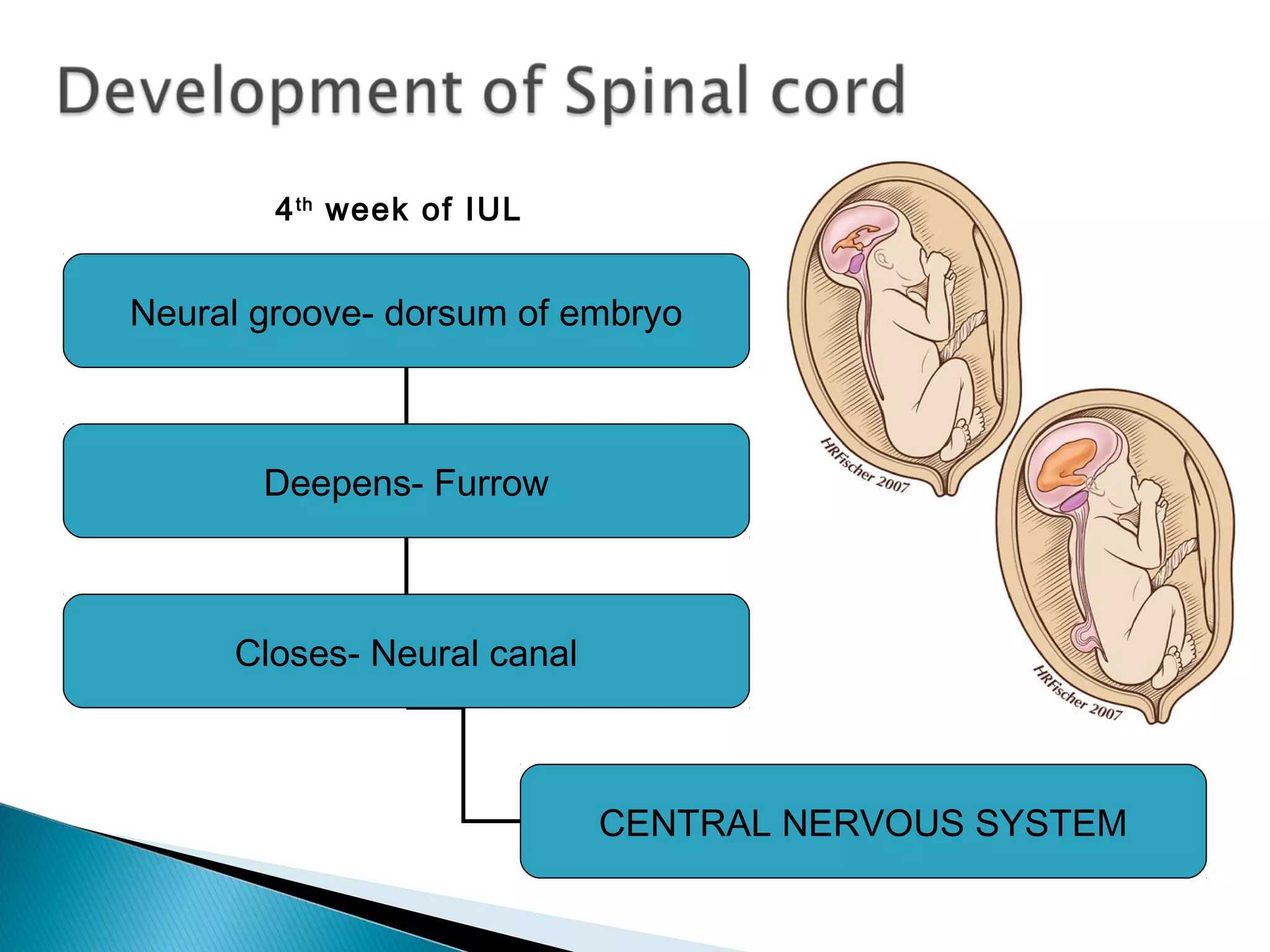

































This document summarizes the development of the central nervous system during the 4th week of gestation. It describes how the neural groove deepens and closes to form the neural tube. Cells within the neural tube then differentiate into neuroblasts and neurons. The meninges develop from surrounding mesenchyme. Vertebral bodies form around the notochord and projections extend around the neural canal to form the vertebral arches. Failure of these arches to fuse can result in spina bifida. The document further describes the types and causes of spina bifida and approaches to management.