3. Introduction
• Recognized birth defect since the time of Hippocrates
• Most common birth defect involving the CNS
• Open spina bifida
• Incidence of NTD: 0.7 – 6.1 / 100 000
• Myelomeningocele is the most complex congenital abnormality that
is compatible with long term survival
4. Terminology
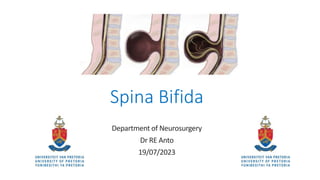
• Spina Bifida:
• Congenital developmental disorder caused by the
incomplete closure of the embryonic neural tube.
• Spina Bifida Occulta
• Range of rare but characteristics features:
• Tethered spinal cord
• Lipoma
• Spinal cord malformation
• Cutaneous stigmata
• Subcutaneous lipoma. Naevus, Hypertrichosis
6. Embryology
• Neuroectoderm thickens into the neural plate.
• Folds over and closes in the midline – primary
neurulation (Day 28)
• Cranial: Anencephaly
• Spinal: Myelomeningocele
• Lower sacral segments form through caudal
regression or secondary neurulation
• Spina Bifida Occulta
• Caudal lipoma
7. Risk Factors
• Role of folate (DNA synthesis)
• Genetic predisposition
• Anticonvulsants
• Esp Epilim during first trimester
• Maternal diabetes
• Fumonisins
• Fungi found mostly in maize
• Oncogenetic activity
• Folate consuming
8. Antenatal Diagnosis + Rx
• Maternal serum alpha protein
• Prenatal U/S
• Detects 90% of cases
• 18 -23 weeks
• Counselling, screening of family
• Risk for subsequent pregnancies
• MOMs trial and subsequent
evolution
9. Perinatal Management
• In SA – most cases are diagnosed at
birth
• Initial mx
• Airway (risk due to brain stem
dysfunction)
• Warmth
• Protection of the defect (prevent
dessication)
• Evaluate clinical level
• Associated Hydrocephalus
• Chiari II Malformation
10. Perinatal Management
• Measure size of defect
• Assess if ruptured or not
• ? Antibiotics
• Keep lesion wet with Normal Saline
dressings
• Keep baby prone with nappy open
(prevent fecal tracking)
• Surgical closure within 36 hours – 72
hours
11. Pre-op Neurological Assessment
• Lowest level of neurological function
• Documented clearly!
• Medico-legal reasons
• Continuous assessments
• Hydrocephalus
• Daily OFC
• Rate of growth
• Cranial U/S
• CT Brain
• High care/ICU setting
• Inspiratory stridor
• Central apneic spells
19. Long term quality of life
• Majority survive into adulthood (>50%)
• Focus on transition of care through adolescence
• Area of sexuality and reproduction
• Urinary and fecal incontinence
• Average IQ, poor social integration
• Emergence of support groups
• International Federation of Spina Bifida and
Hydrocephalus (IFSBH)
• ASBAH (Association of Spina Bifida and Hydrocephalus
20. Advances
• MOMs trial
• Prenatal surgery reduced the need for shunting and
improved motor outcomes
22. Summary
• MDT Team
• Prevention and antenatal diagnosis likely to have more of an impact
on outcome
• Women of child-bearing age to be on Folate
• As neurosurgeons we must stick to rigid principles of initial
management
23. References
• Adzick NS, Thom EA, Spong CY, Brock JW, 3rd , Burrows PK, Johnson MP,
Howell LJ, Farrell JA, Dabrowiak ME, Sutton LN, Gupta N, Tulipan NB,
D'Alton ME, Farmer DL; MOMS Investigators. A randomized trial of prenatal
versus postnatal repair of myelomeningocele. N Engl J Med 2011; 364:
993–1004.
• Greenberg, Handbook of Neurosurgery, 10th edition
• Oakeshott P, Hunt GM. Long‐term outcome in open spina bifida. Br J Gen
Pract 2003; 53: 632–636
• Erşahin Y, Yurtseven T. Delayed repair of large myelomeningoceles. Childs
Nerv Syst. 2004;20:427–9
24. Question 1
A neonate is born with an open myelomeningocele to a first-time mother.
Upon counselling on subsequent pregnancies, the risk of having another
baby with a myelomeningocele is approximately:
1. 0.1 – 0.2 %
2. 2 – 3 %
3. 6 – 8 %
4. 8 – 15 %
25. Question 2
You are consulted to review a neonate with a dimple on the lumbosacral
region. The child is fully neurologically intact with no obvious bony defect
palpable. This is likely to be:
1. Dermal sinus tract
2. Spina bifida occulta
3. Spina bifida aperta
4. Myeloschisis
26. Question 3
Myelomeningoceles result from a disorder at which stage of embryonic
development:
1. Primary neurulation
2. Gastrulation
3. Secondary neurulation
4. Somitogenesis
27. Question 4
The following is a complication that can occur if the junctional zone is not
adequately resected and remnants of epithelialized tissue remains in the
closure:
1. Epidermoid cyst
2. Dermoid inclusion tumour
3. Tethered cord
4. Teratoma
28. Question 5
The role of fetoscopic surgery in the intra-uterine repair of
myelomeningocele, as per the MOMs trial showed a potential benefit in:
1. Reducing the need for VP shunts for hydrocephalus
2. Reduced risk of urinary incontinence
3. Improvement in overall cognitive function
4. Reduced number of kyphotic deformity present at 6 months
The term occulta means “hidden”. It is the mildest form of SB. The splits in the vertebra are so small, usually just a spinous process or part of the lamina, that the spinal cord doesn’t protrude. The skin at the site may be normal, or have certain features like dimpling or hair around it.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.
Risk of MMC – 0.1%. Jumps to 2-3% after first pregnancy and then to 6-8% after two kids.