Downloaded 11,351 times



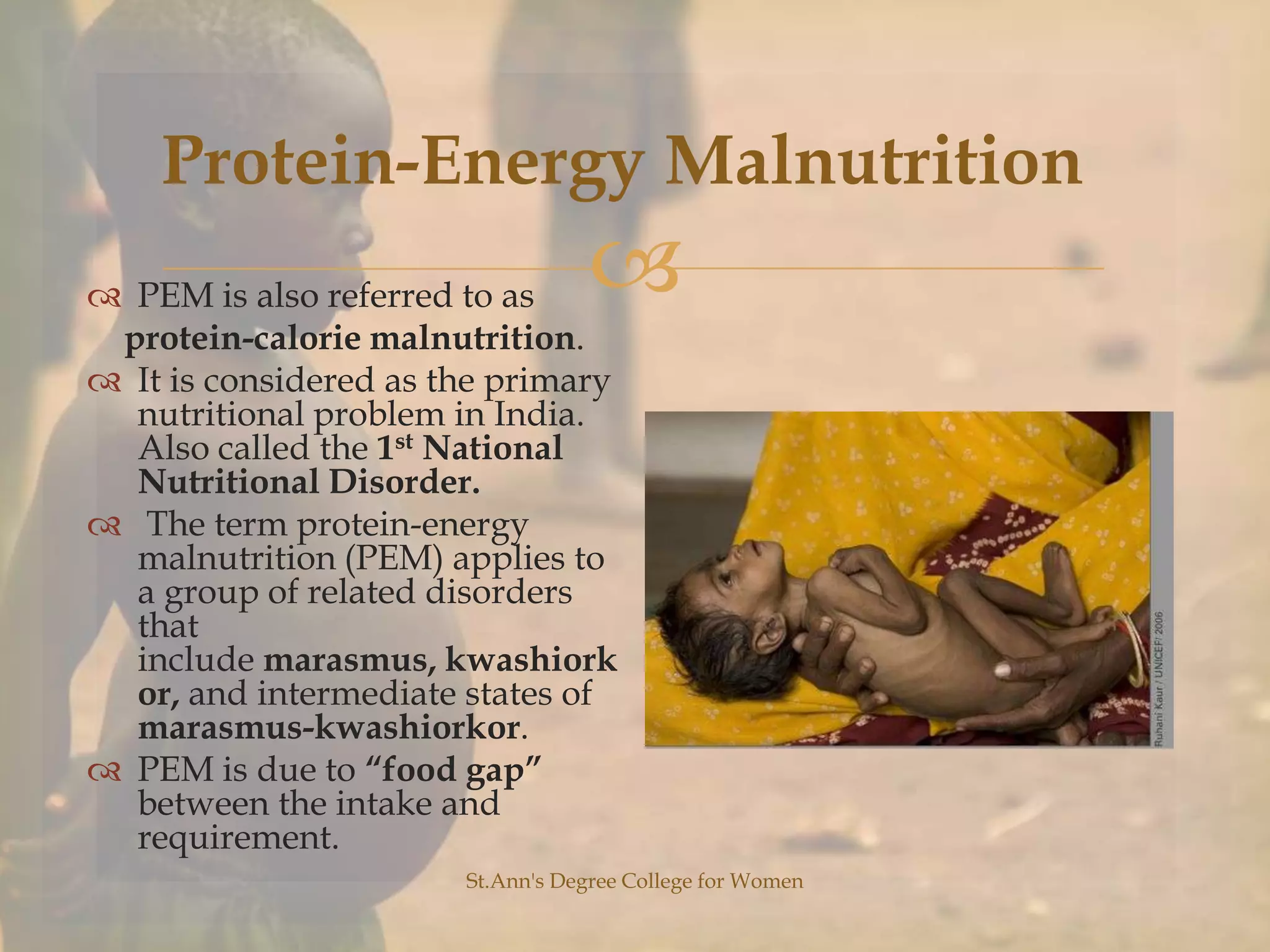




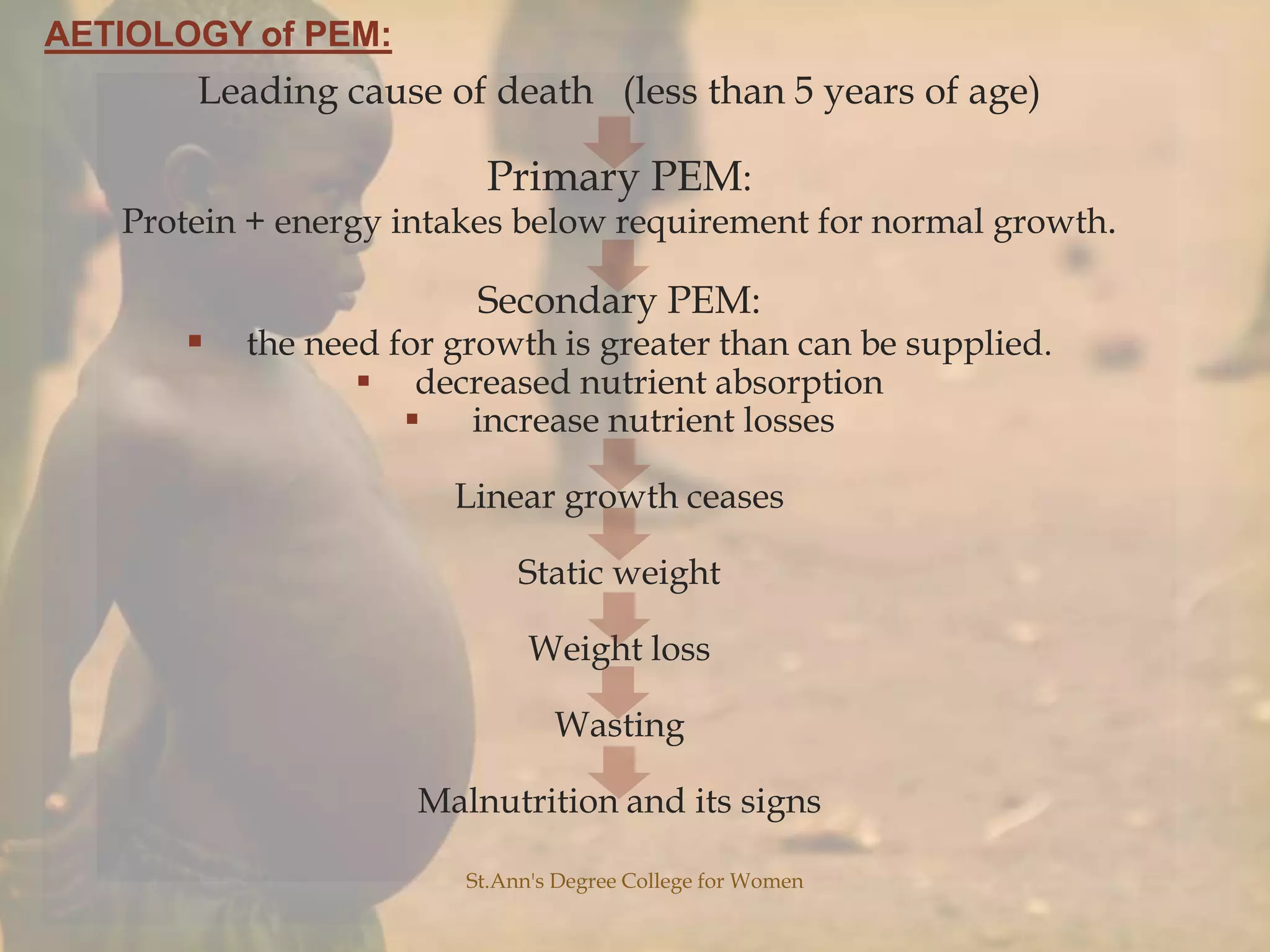




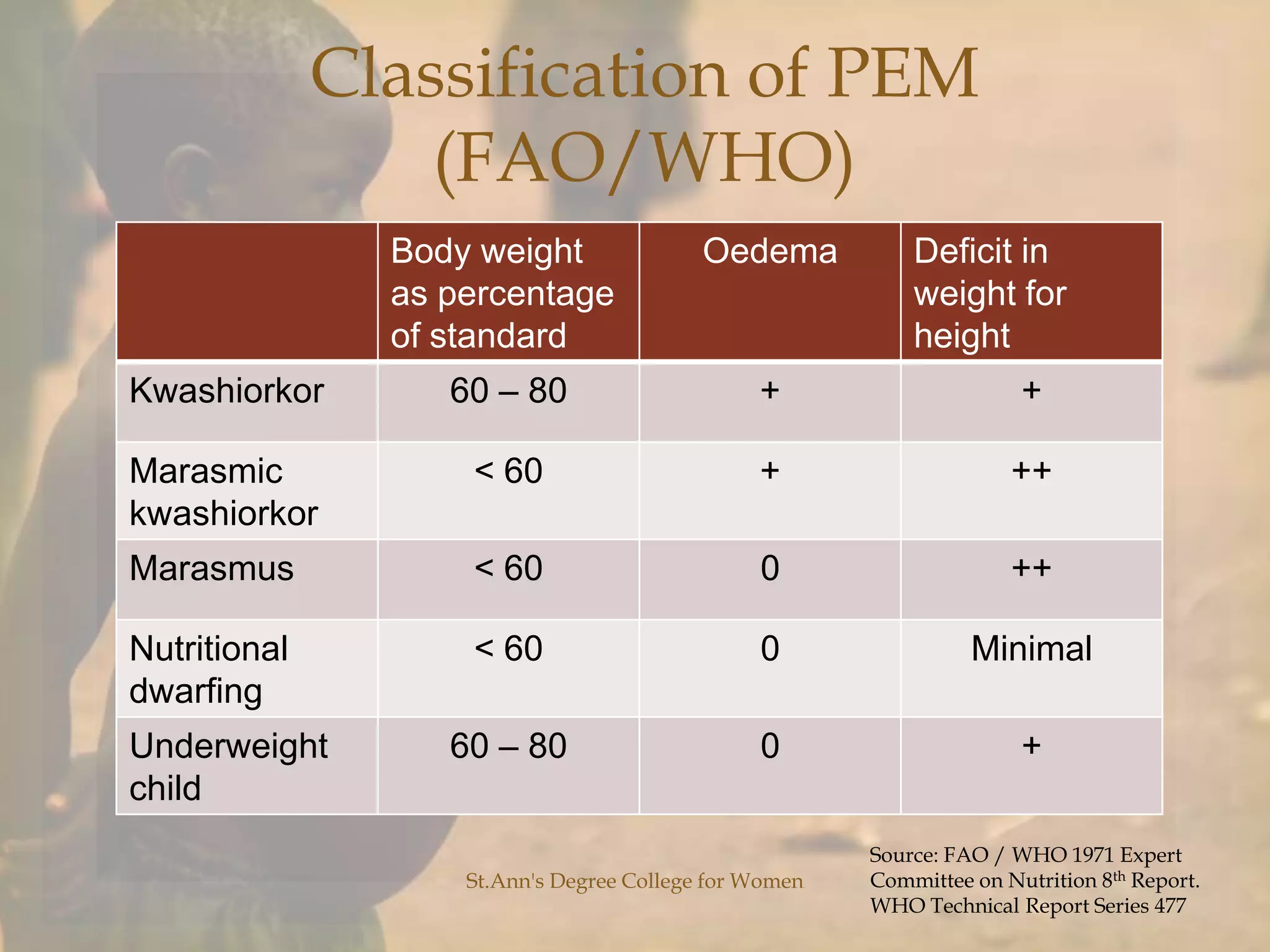

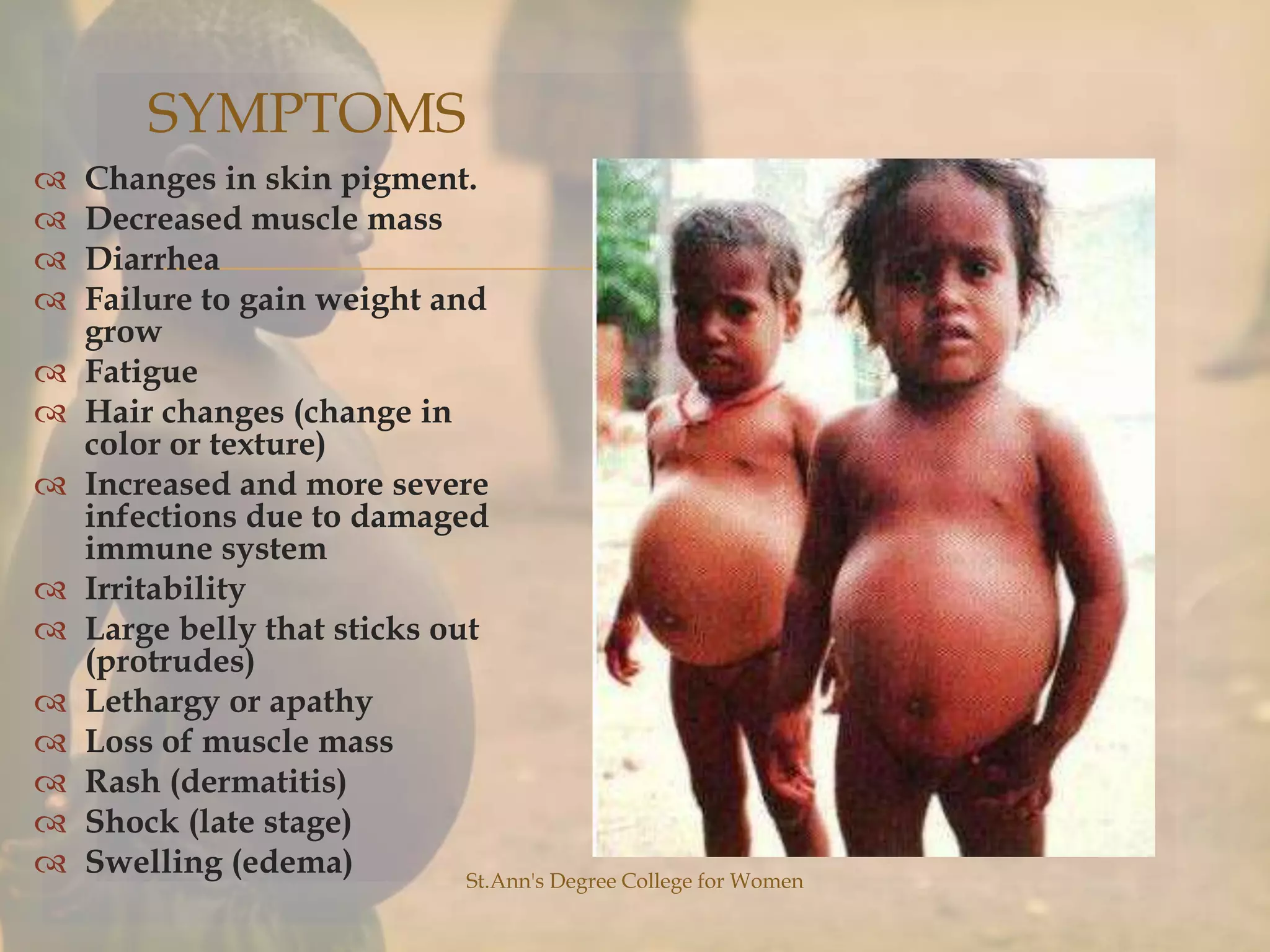

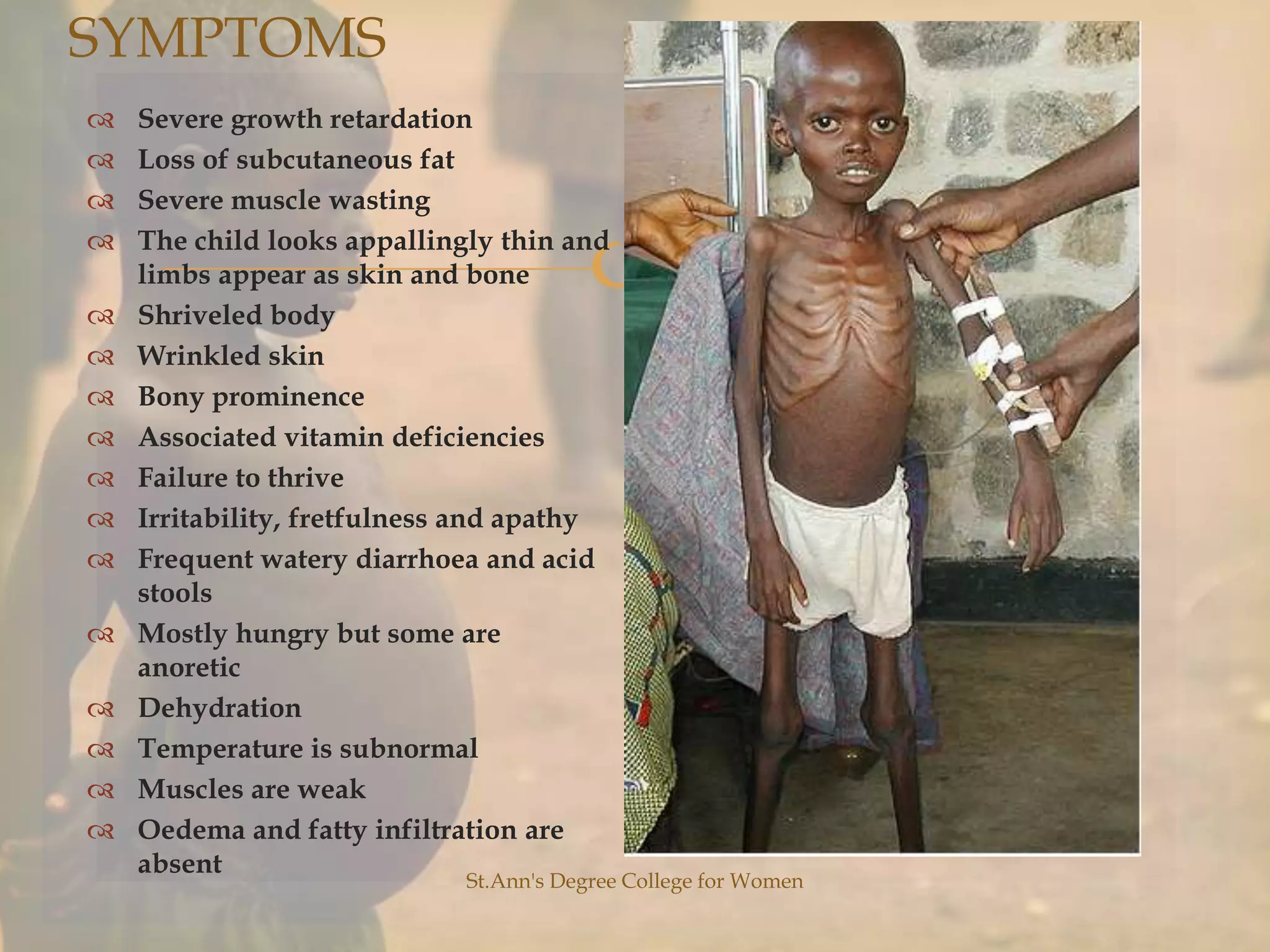

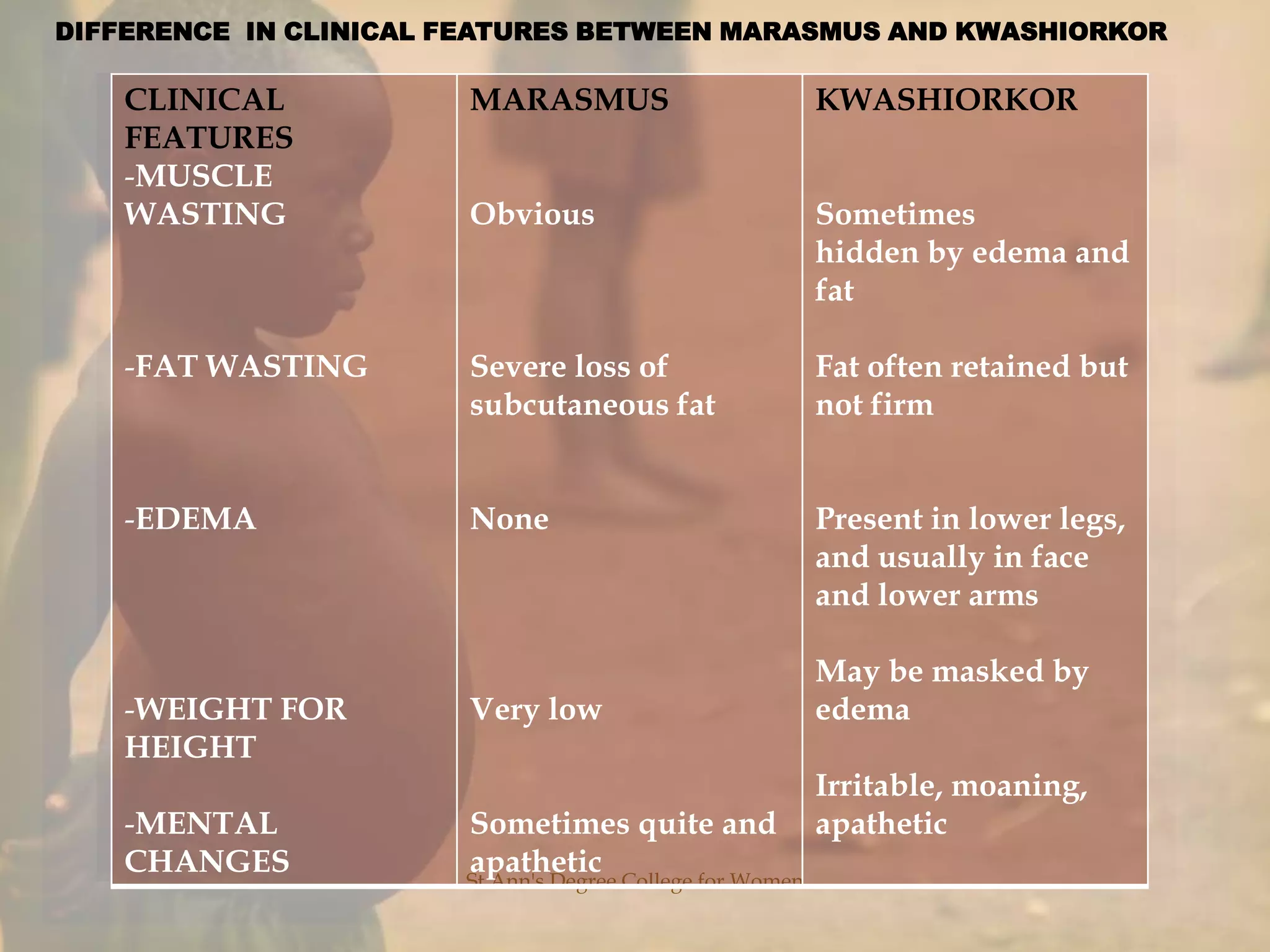
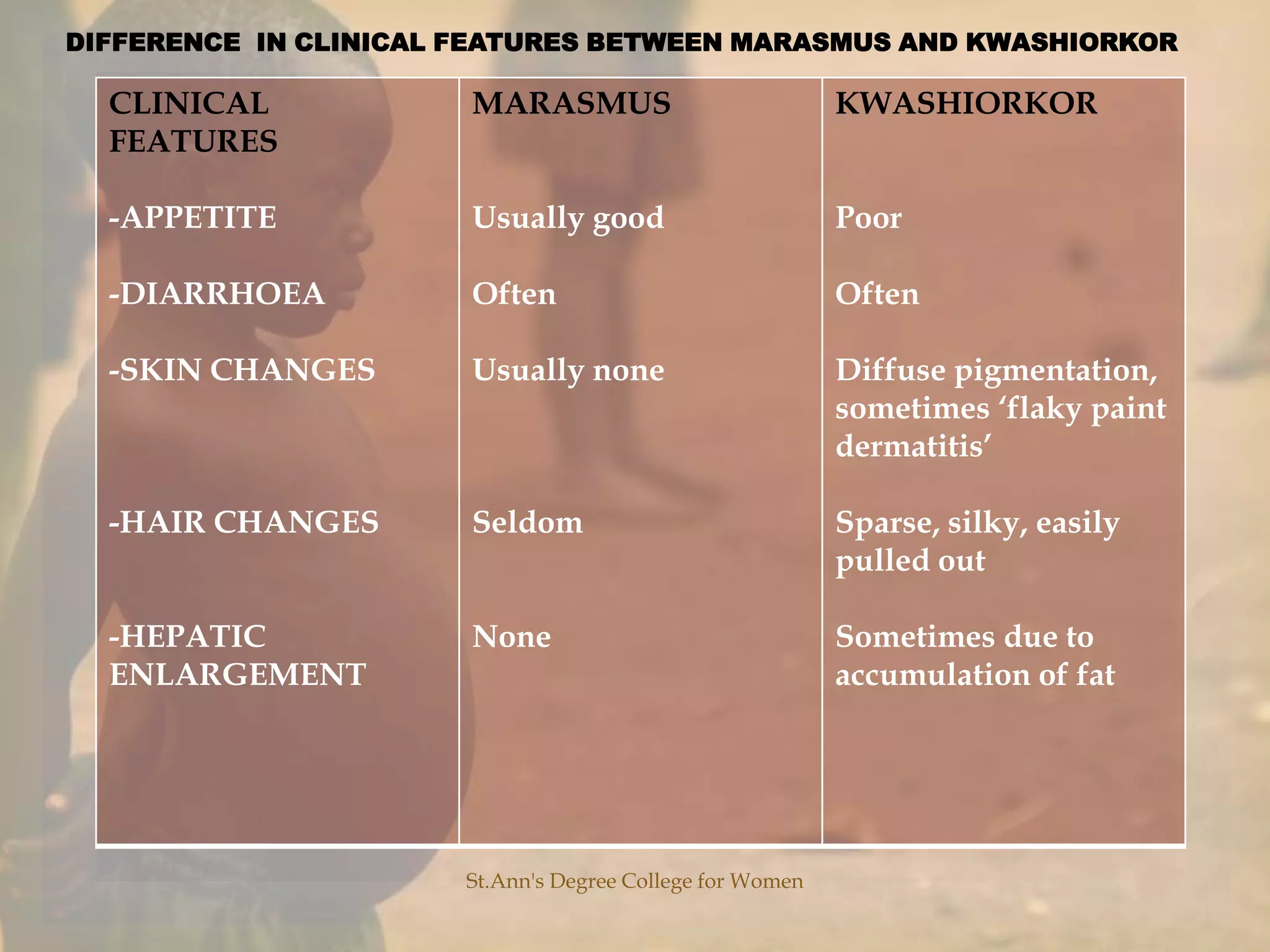












This document discusses malnutrition and provides definitions and descriptions of different types. It begins by defining malnutrition and protein-energy malnutrition. It then describes marasmus and kwashiorkor, two types of protein-energy malnutrition. Marasmus is characterized by energy deficiency and emaciation, while kwashiorkor is caused by protein deficiency and causes fluid retention. The document also discusses the prevalence of malnutrition in India, clinical features, symptoms, differences between marasmus and kwashiorkor, and etiological factors of protein-energy malnutrition.