Download to read offline



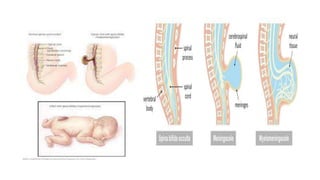


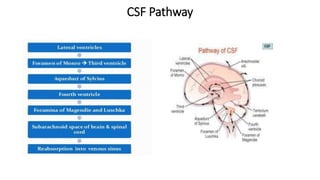




Spina bifida is a neural tube defect where there is an incomplete closure of the vertebrae and neural tube. It can range from mild forms where there are no symptoms to more severe forms with neurological deficits depending on the location and severity of the defect. Management involves surgery to close the defect early in life as well as lifelong multidisciplinary care to address issues like bowel and bladder dysfunction, mobility, skin integrity, and neurodevelopment. Hydrocephalus is an excess of cerebrospinal fluid in the brain that can be congenital or acquired and may require surgical treatment like shunt placement to drain the fluid.



































































