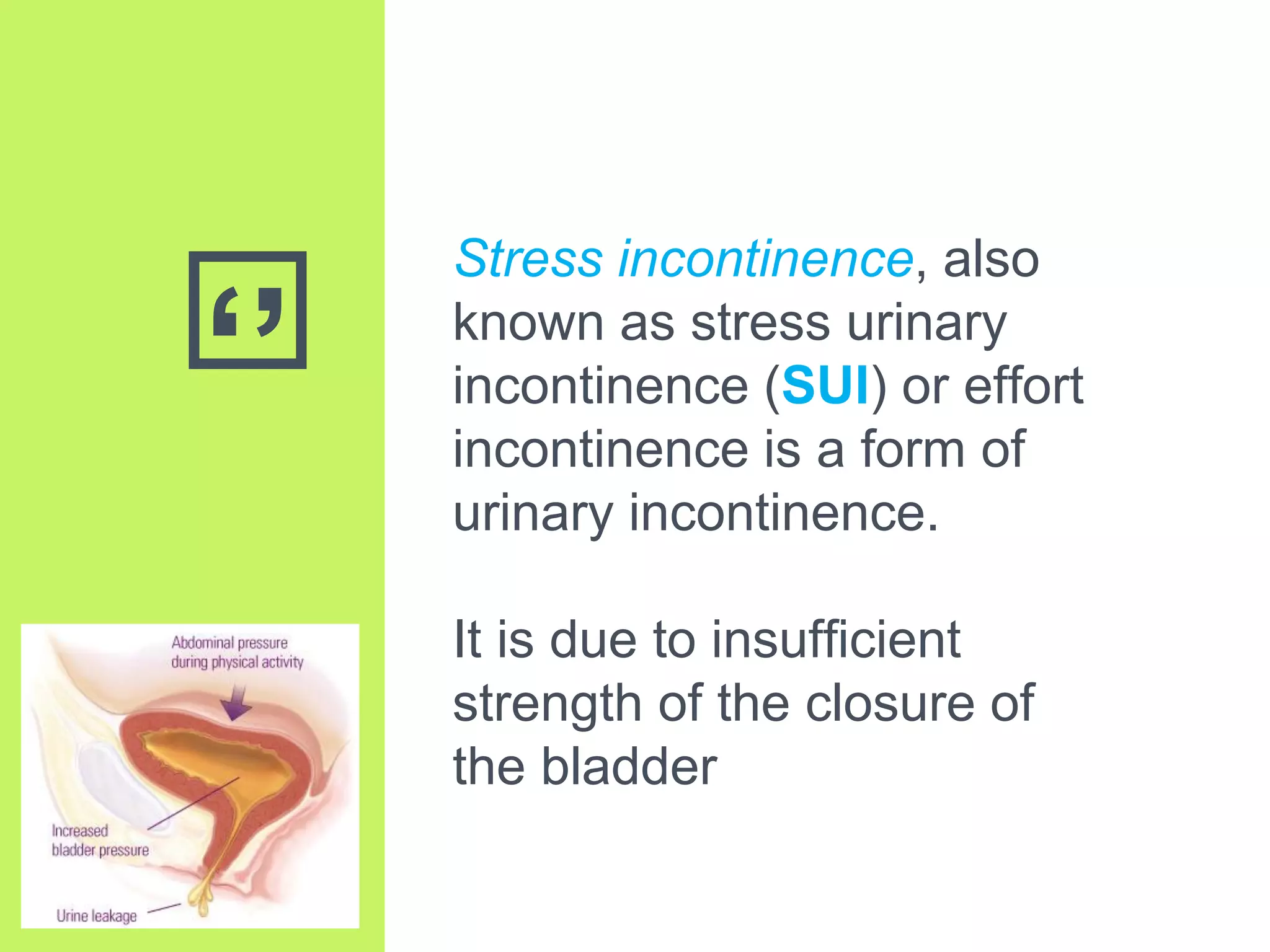
Stress urinary incontinence (SUI) is a prevalent condition in women characterized by involuntary urine leakage during physical exertion, with the most common risk factors including pregnancy, age, and obesity. The document covers the etiology, symptoms, diagnostic approaches, and both non-surgical and surgical management options for SUI. It highlights the importance of conservative management, including pelvic floor muscle training, before considering surgical interventions.






























































































![Newer drugs in management of copd [2018 update]](https://cdn.slidesharecdn.com/ss_thumbnails/newerdrugsinmanagementofcopd2018update-180309071249-thumbnail.jpg?width=640&height=640&fit=bounds)
























