Downloaded 134 times

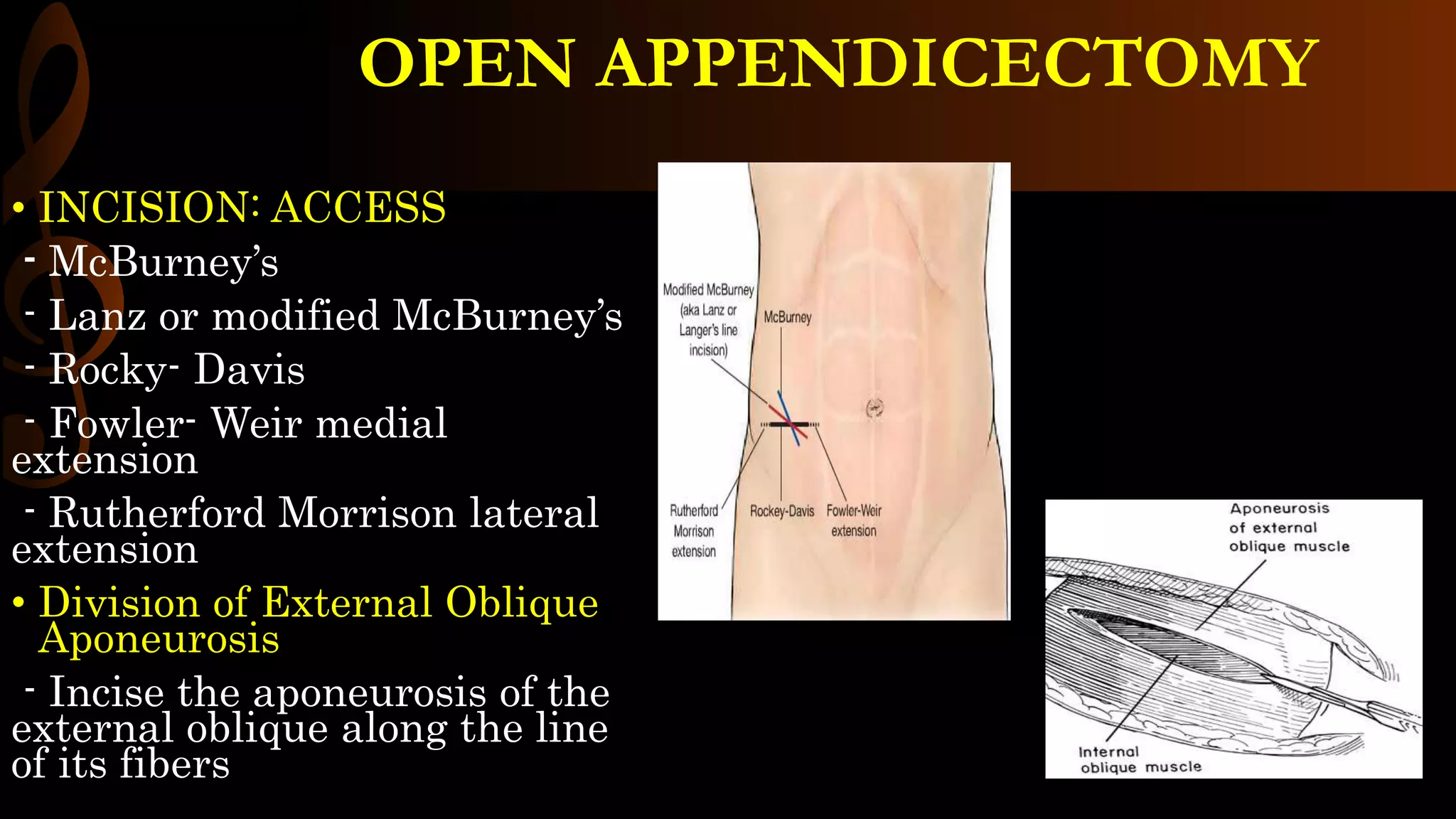


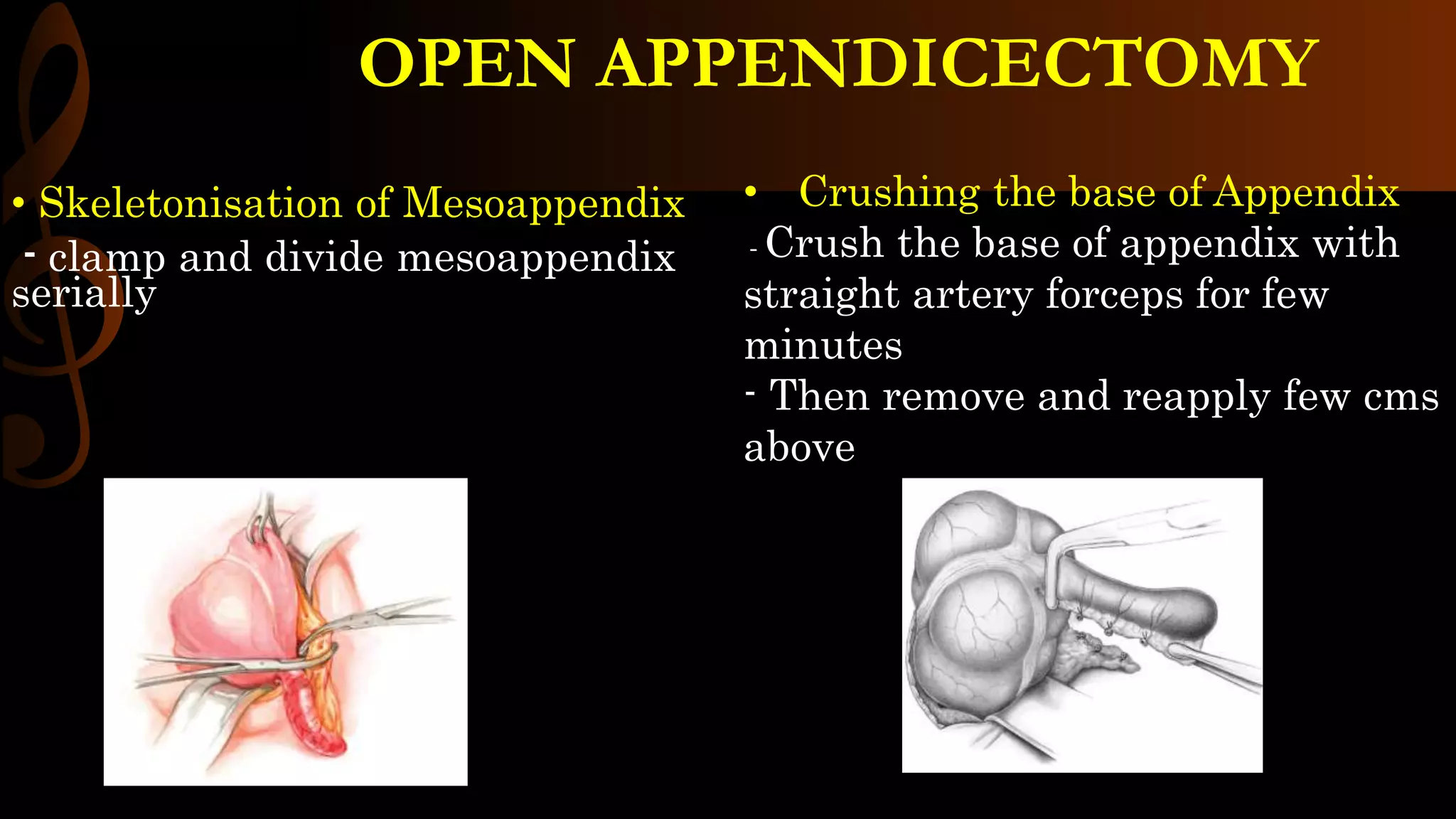

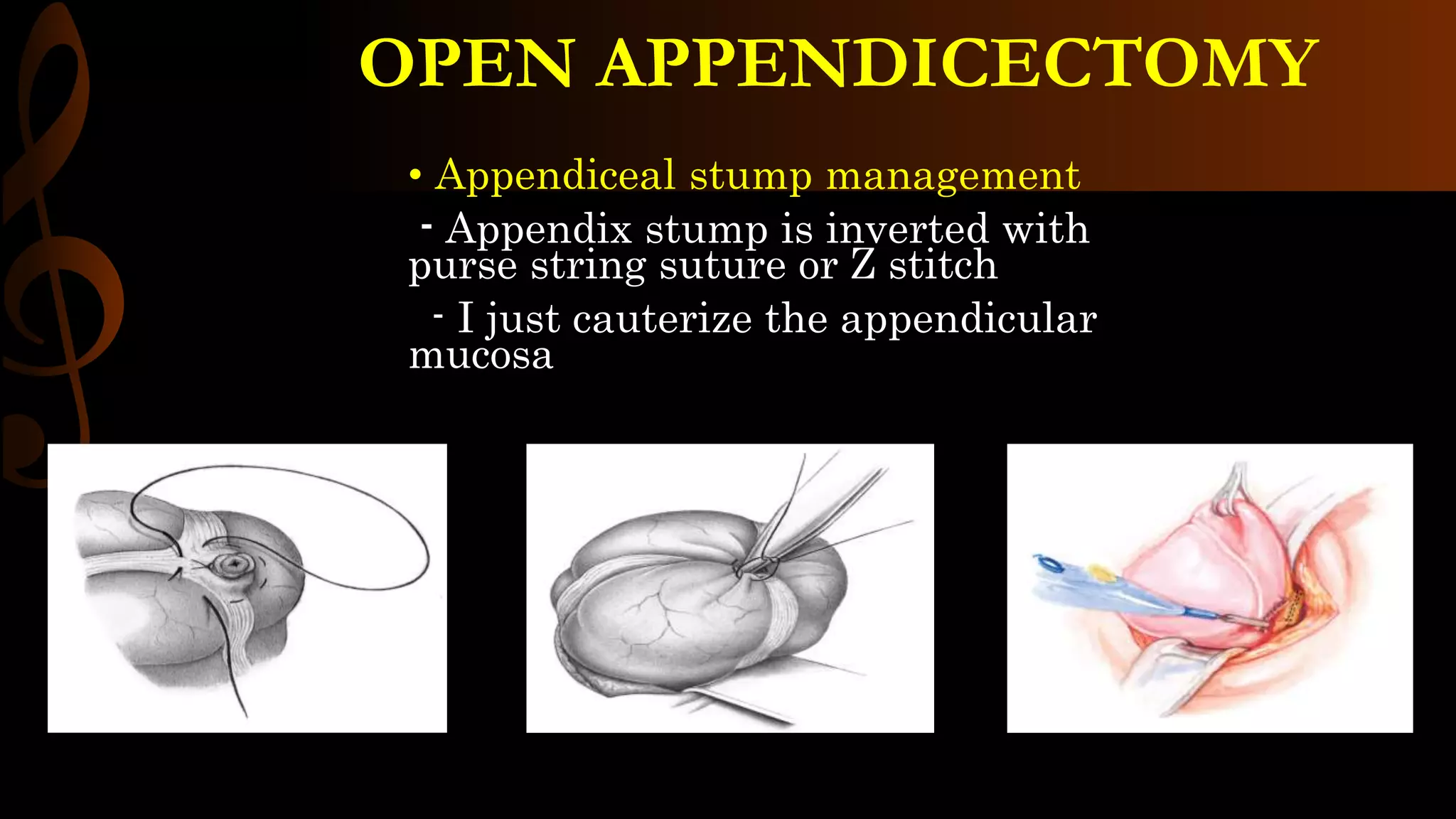
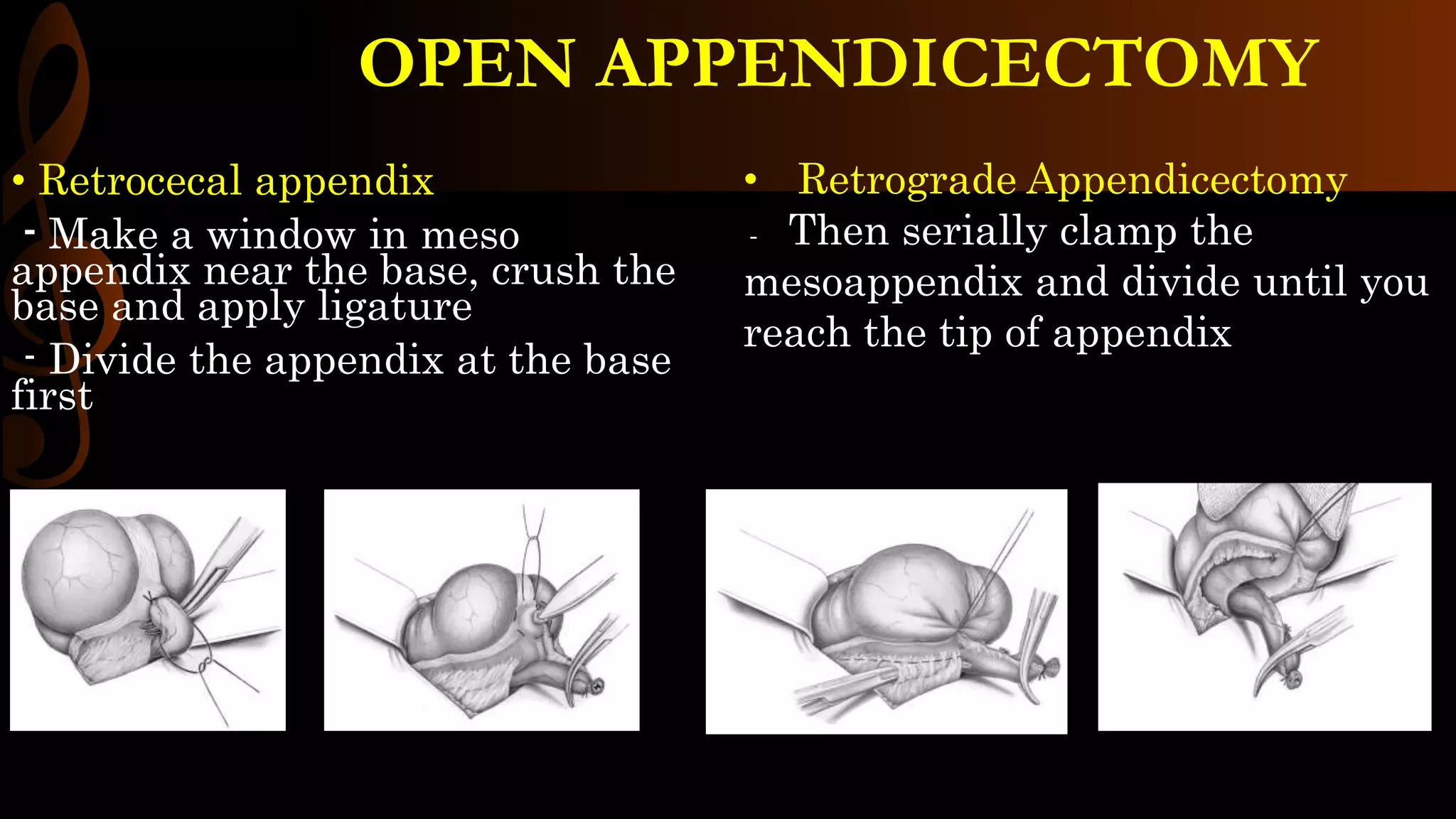



The document outlines the procedure for open appendicectomy, including indications, anesthesia options, patient positioning, and informed consent details. It details surgical steps such as incision techniques, muscle handling, cecal pole mobilization, mesoappendix handling, and appendix removal methods. It concludes with guidelines for managing the appendiceal stump and closing surgical wounds.