Downloaded 463 times
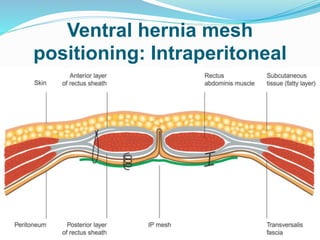
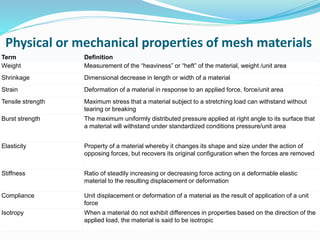
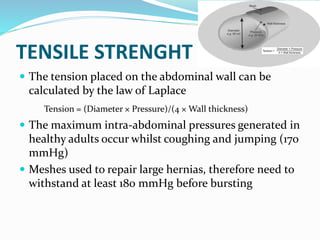
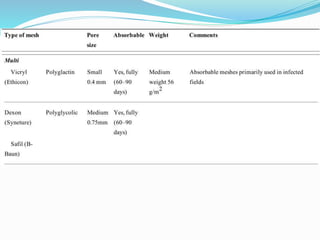

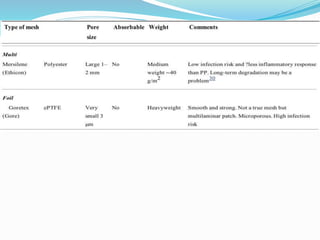

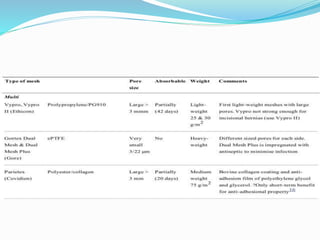

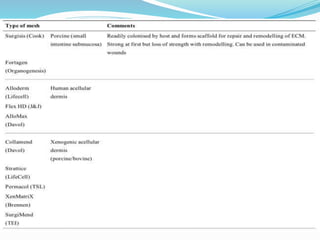






The document discusses properties that surgeons should consider when choosing a mesh for hernia repair. Ideal meshes are lightweight, with large pores to reduce foreign body reaction and chronic pain. Monofilament meshes have the lowest risk of infection. For intraperitoneal placement, composite meshes may reduce adhesions by providing an absorbable surface. Overall, lightweight polypropylene or polyester meshes are generally suitable in most contexts by balancing strength, flexibility and biocompatibility.



































































