Downloaded 88 times


















![TAPP: STEP 1: Tips
• The intra-abdominal cavity is visualized with the Telescope
and intraabdominal findings are reported [intra-abdominal
pathology and inguinal hernia defects and sacs].
• If an asymptomatic hernia sac is identified on the
contralateral side, consider repair.
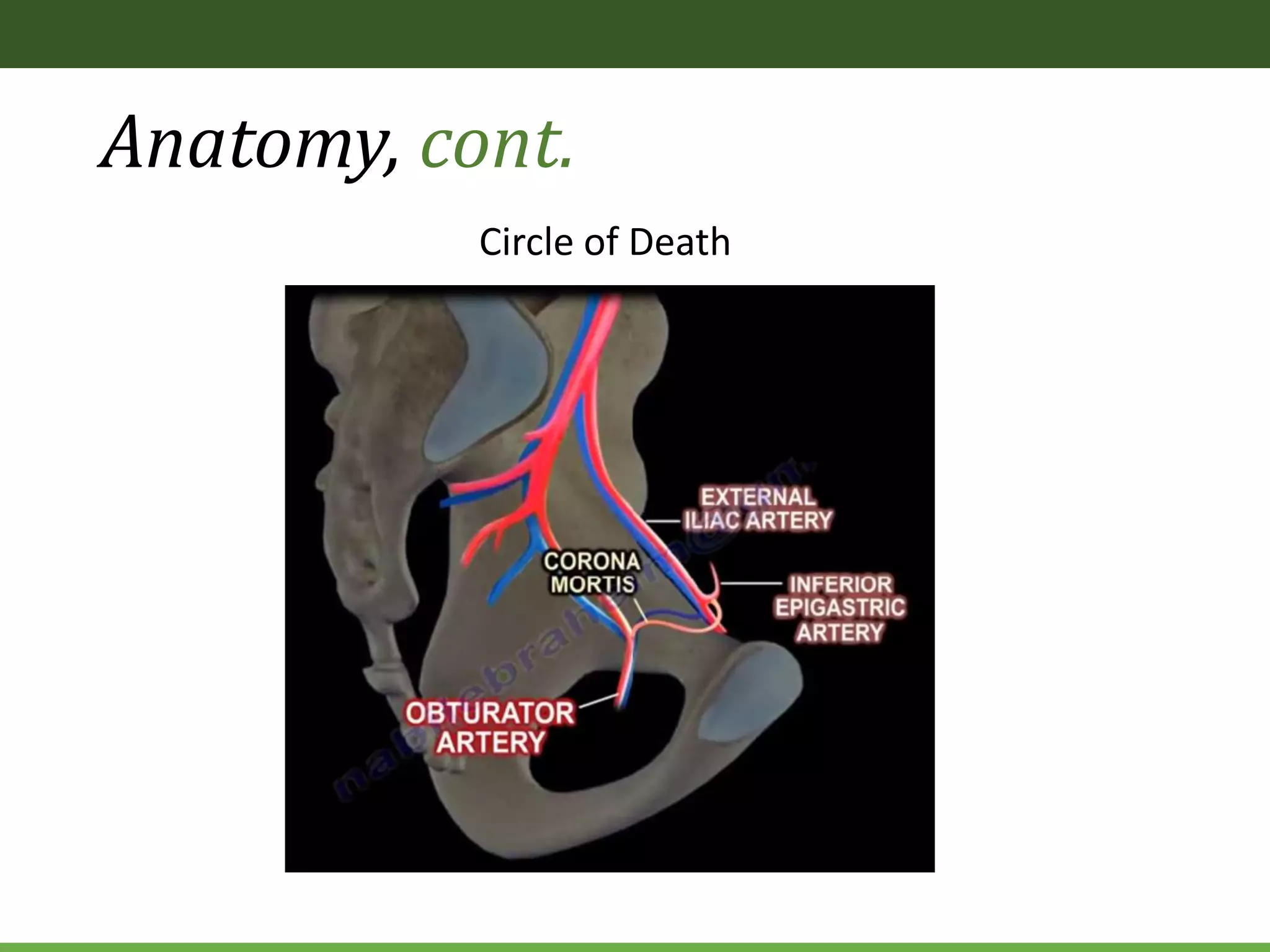
• The bladder, median and medial umbilical ligaments, external
iliac, and inferior epigastric vessels are visualized.](https://image.slidesharecdn.com/differenttypesoflaparoscopicherniarepair-191208184939/75/Different-types-of-laparoscopic-hernia-repair-36-2048.jpg)












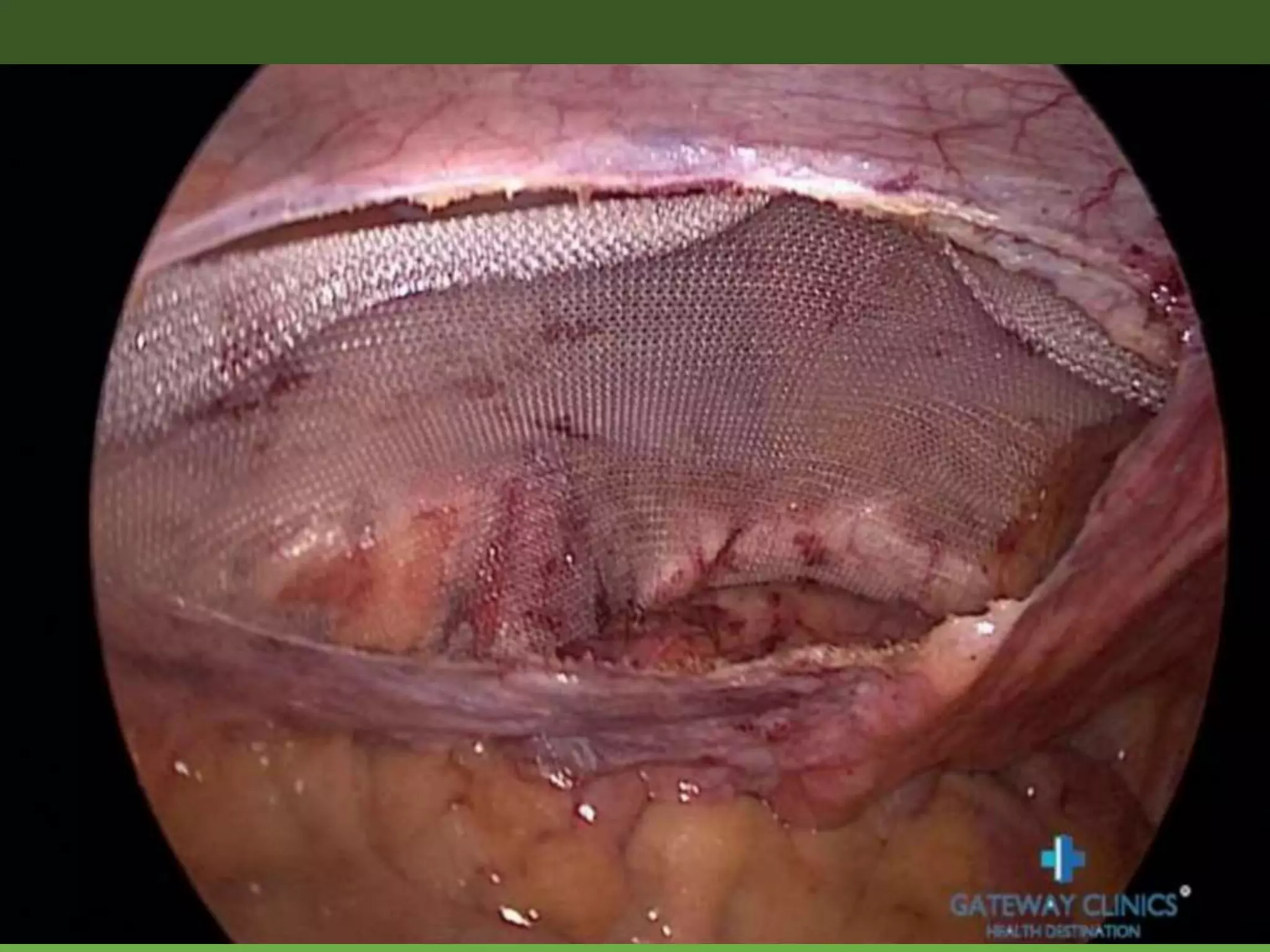



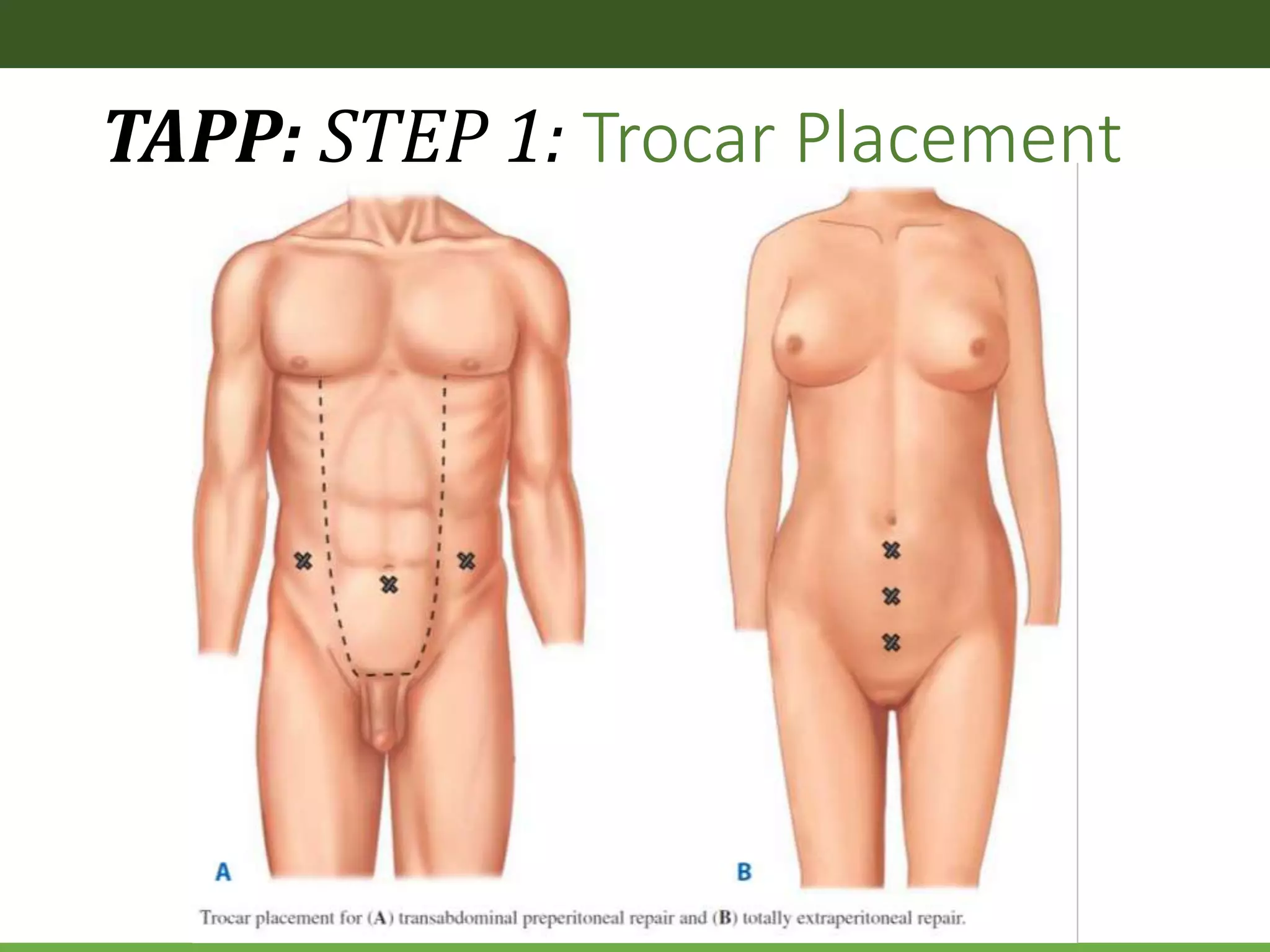
The document discusses laparoscopic hernia repair, including definitions of hernias, types of hernias, and laparoscopic repair options. It focuses on the transabdominal preperitoneal (TAPP) technique for laparoscopic inguinal hernia repair. The TAPP procedure involves entering the abdominal cavity laparoscopically, incising the peritoneum to access the preperitoneal space, dissecting and removing hernia sacs, placing mesh to reinforce the defect, and closing the peritoneum. Key anatomical structures are identified including the triangles of doom and pain. The steps of TAPP repair and important technical considerations are described in detail.























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















