Downloaded 521 times


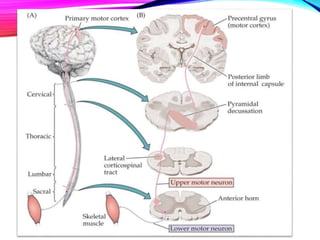
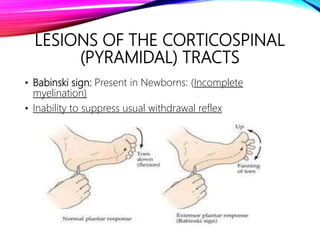
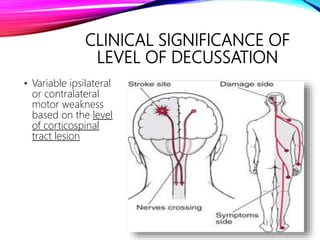
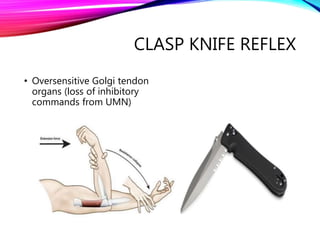
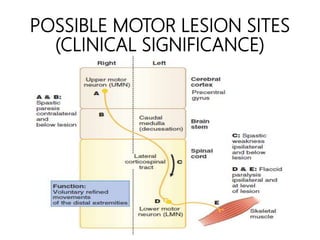
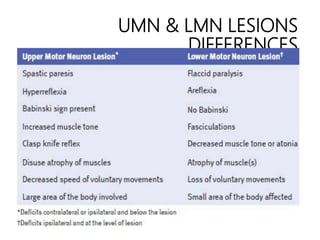


Upper and lower motor neurons control skeletal muscle contraction through a two-neuron pathway. Upper motor neurons originate in the brain and direct the activity of lower motor neurons in the spinal cord and brainstem. Lesions of upper motor neurons cause spastic weakness, hyperreflexia, and loss of fine motor skills. Lesions of lower motor neurons result in flaccid paralysis, loss of reflexes, and muscular atrophy. Differentiating between upper and lower motor neuron lesions is important for determining the neurological level and prognosis.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


