
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Transverse myelitis
Similar to Transverse myelitis (20)
More from PRADEEPA MANI
Recently uploaded
Recently uploaded (20)
Transverse myelitis
- 1. MRS. M.PRADEEPA MPT (Neuro) VICE PRINCIPAL PPG COLLEGE OF PHYSIOTHERAPY COIMBATORE, TAMILNADU, INDIA
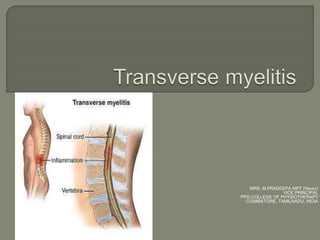
- 2. Acute transverse myelitis (ATM) is an inflammatory condition affecting both halves of the spinal cord and associated with rapidly progressive motor, sensory, and autonomic dysfunction. Spinal cord involvement is usually central, uniform and symmetric Longitudinally extensive transverse myelitis (LETM) is defined as a TM with a spinal cord lesion that extends over three or more vertebral segments. The causes of LETM are also heterogeneous and the presence of MOG auto-antibodies has been proposed as a biomarker for discrimination.
- 3. 1-4 /million/per Affecting all ages, peaks at ages 10 – 19 years and 30 – 39 years No sex or familial predisposition
- 4. Acute infection – mostly viral, bacterial, fungal and parasities Post infectious – respiratory or gastrointestinal infections within 3 to 8 weeks Post vaccination Direct invasion of spinal cord Systemic autoimmune diseases – SLE, MS Systemic malignancy Atopy and allergy (atopic myelitis) Vascular disorders – AVM, disk embolism, intra spinal cavernous malformations.
- 5. Complete or Incomplete/Partial TM: 1. Complete involvement of spinal cord segment leading to severe paralysis 2. Partial involvement or section of the spinal cord involvement Acute or subacute TM: 1. Depends on progression – time of occurance to maximal disability is more than 4hr and fewer than 21 days 2. Acute TM – Over minutes to hours 3. Subacute TM – Over days to weeks
- 6. Progressive loss of the fatty myelin sheath surrounding the nerves in the affected spinal cord which may be due to 1. Cell mediated autoimmune response 2. Autoimmune vasculitis 3. Direct viral invasion of the spinal cord Inflammation may lead to presence of perivascular lymphocytic infiltrates, necrosis, and demyelination
- 8. Lesions may occur anywhere within the cord, with the thoracic cord being the most frequently involved site. Three phases 1. Initial phase – motor and sensory preceding sphincter dysfunction usually over 2 to 3 days 2. Plateau phase – mean duration 1 week 3. Recovery phase
- 9. Four classic features 1. Motor 2. Pain 3. Sensory alterations 4. Bladder and bowel dysfunction 5. Later stages ANS involvement Disturbances in sensory, motor and dysfunction of the autonomic nervous system at the level of the lesion or below, are noted.
- 10. Weakness of the legs and arms: Weakness in the legs progresses rapidly. If the myelitis affects the upper spinal cord it affects the arms as well. Individuals usually may develop paraparesis that may progress to paraplegia. If high cervical lesion – respiratory failure companies UMN Lesion – increased tone, spastic weakness usually symmetric, legs more than arms Reflexes – brisk, positive Babinski sign
- 12. Initially lower Back pain – sharp, shooting pain can occur at the site of inflammed spinal cord Radiating down the legs or arms or around the torso
- 13. The degree and type of sensory loss will depend upon the extent of the involvement of the spinal cord and various sensory tracts Paraesthesias - abnormal sensations such as burning, tickling, pricking, numbness, coldness, or tingling in the legs. Abnormal sensations in the torso and genital region are common. Lhermitte’s phenomenon Sensory ataxia – posterior column involvement Spinothalalmic tract – contralateral pain and temperature loss
- 14. Initially – Urinary retention Later – Incontinence, constipation
- 15. Autonomic dysreflexia Hypertension Bradycardia Headache(severe and pounding) Profuse sweating Increased spasticity Restlessness Vasoconstriction below the level of lesion Vasodilation(flushing) above the level of the lesion Constricted pupils Nasal congestion Pilo erection (goose bumps) Blurred vision
- 16. CT variable enlargement of the spinal cord and contrast enhancement patterns MRI Up to 40% of cases have no findings on MRI and in 60 % of cases the appearance is variable and non-specific: Large variation in lesion size occupy greater than two-thirds of the cross-sectional area of the cord, most commonly extend for 3-4 spinal segments Typical signal characteristics include: T1: isointense or hypointense T2: poorly delineated hyperintense signal T1 C+ (Gd): variable enhancement patterns (none, diffuse, patchy, peripheral)
- 18. Blood test: Presence of autoantibodies – (anti- aquaporin-4, anti-myelin oligodendrocyte) and a host of antibodies associated with cancer (paraneoplastic antibodies) may be found Lumbar puncture: More protein and leukocytes in CSF and elevation of IgG index
- 20. Multiple sclerosis • plaques are shorter than two vertebral body segments in length and involve less than half the cross-sectional area of the cord • plaques are characteristically peripherally located in the dorsal and lateral columns ADEM • similar appearance to spinal MS plaques (however younger age at presentation, monophasic clinical course and more often associated with thalamic lesions) Spinal cord infarct • spinal cord is usually enlarged • abnormality typically extends over multiple vertebral body segments • can occur at any location in the cord but has a propensity for the upper thoracic or thoracolumbar regions Intramedullary neoplasm • invariable spinal cord expansion • commonly associated with cysts and syringohydromyelia • may have evidence of prior hemorrhage • slowly progressive clinical course
- 21. Intravenous corticosteroid drugs : Decrease swelling and inflammation. Methylprednisolone or dexamethasone usually administered for 3 to 7 days and sometimes followed by a tapering off period. Plasma exchange therapy (plasmapheresis) may be used for people who don’t respond well to intravenous steroids. Intravenous immunoglobulin (IVIG) is a treatment thought to reset the immune system.
- 22. Analgesics: Acetaminophen, ibuprofen, and naproxen. Nerve pain may be treated with certain antidepressant drugs (such as duloxetine), muscle relaxants (such as baclofen, tizanidine, or cyclobenzaprine), and anticonvulsant drugs (such as gabapentin or pregabalin). Antiviral medications may help those individuals who have a viral infection of the spinal cord. Medications can treat other symptoms and complications, including incontinence, painful muscle contractions called tonic spasms, stiffness, sexual dysfunction, and depression
- 23. Physical therapy Occupational therapy Vocational therapy Psychotherapy
- 24. Spontaneous recovery in 40 – 50 % of cases. Children recovery is better than adults Most people have partial recovery taking place within the first 3 months after the attack. For some people, recovery may continue for up to 2 years Individuals may have moderate disability such as trouble walking, nerve sensitivity, and bladder and bowel problems or may have permanent weakness, spasticity, and other complications. May people experience only one episode although recurrent or relapsing transverse myelitis does sometimes occur, particularly when an underlying cause such as MS or NMOSD can be found. Some people recover completely and then experience a relapse. Others begin to recover and then suffer worsening of symptoms before recovery continues.