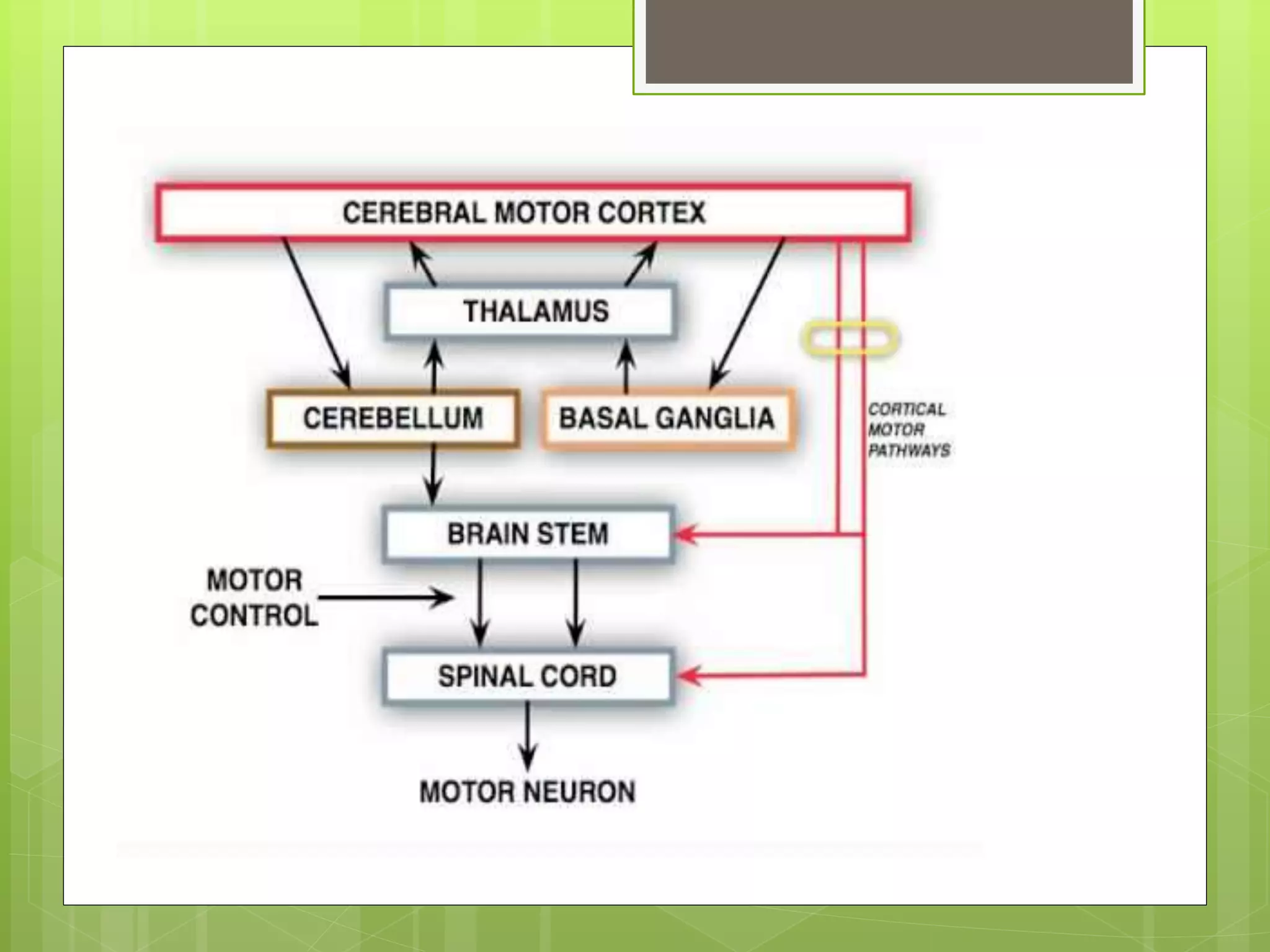
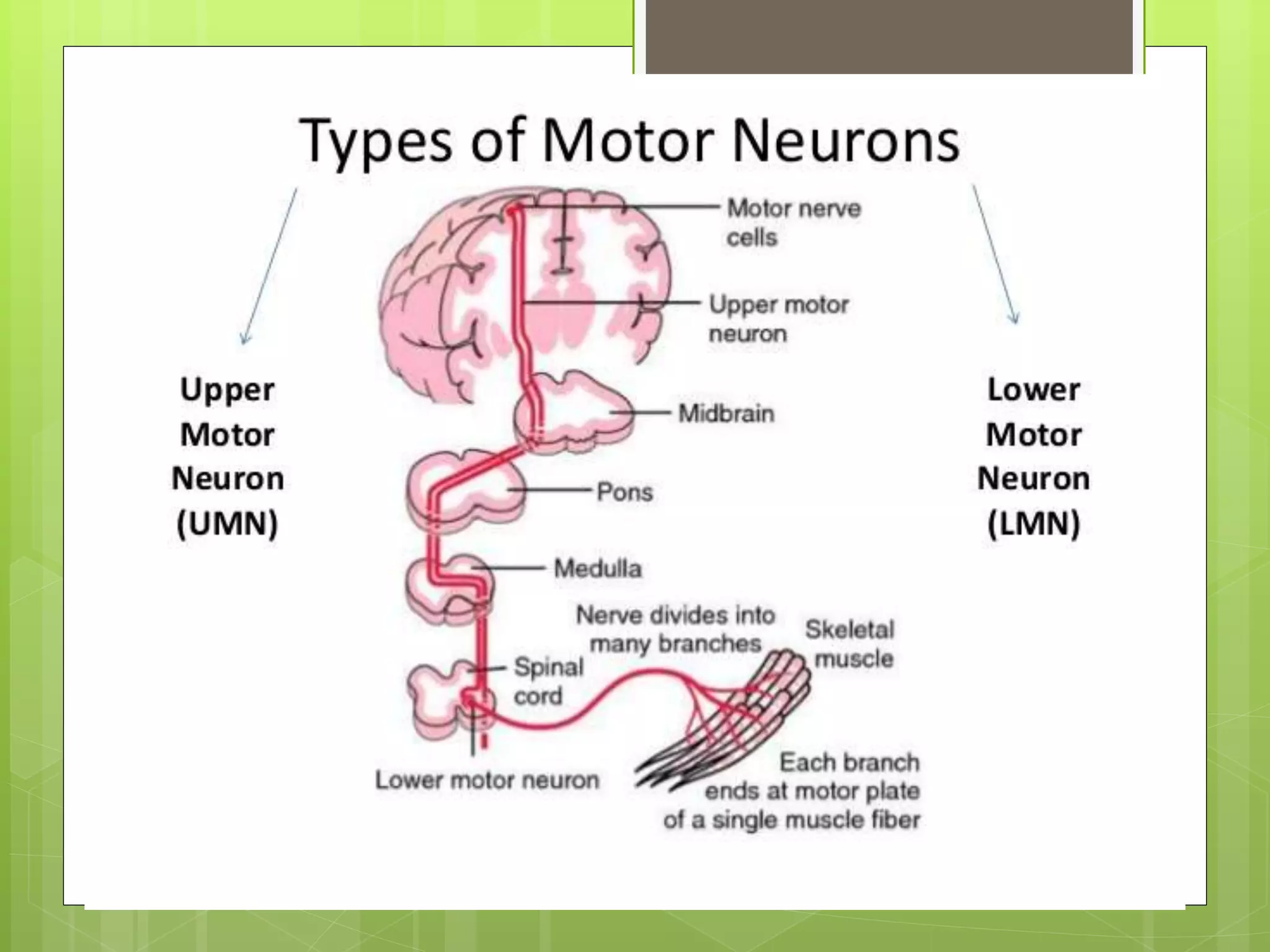
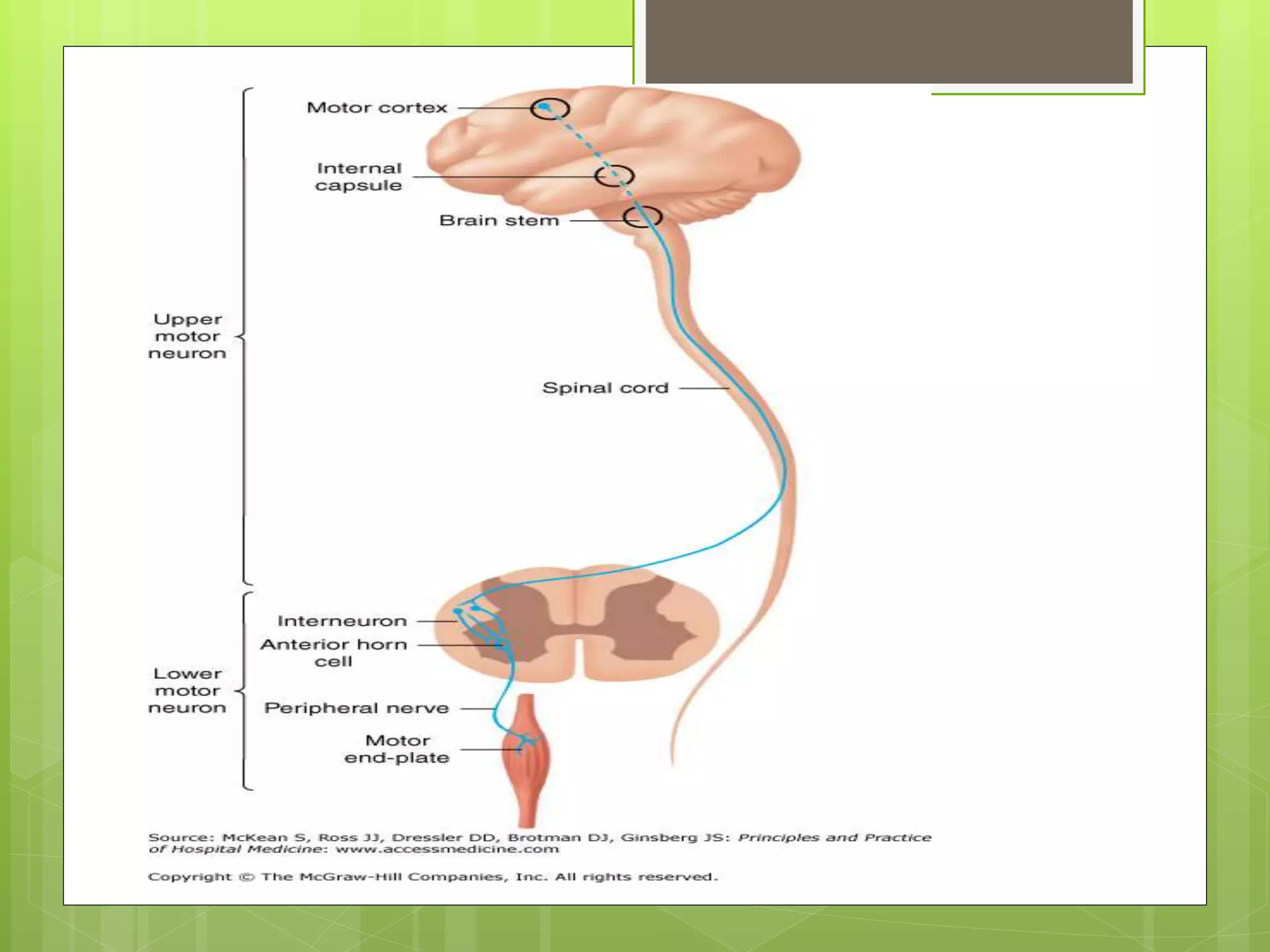
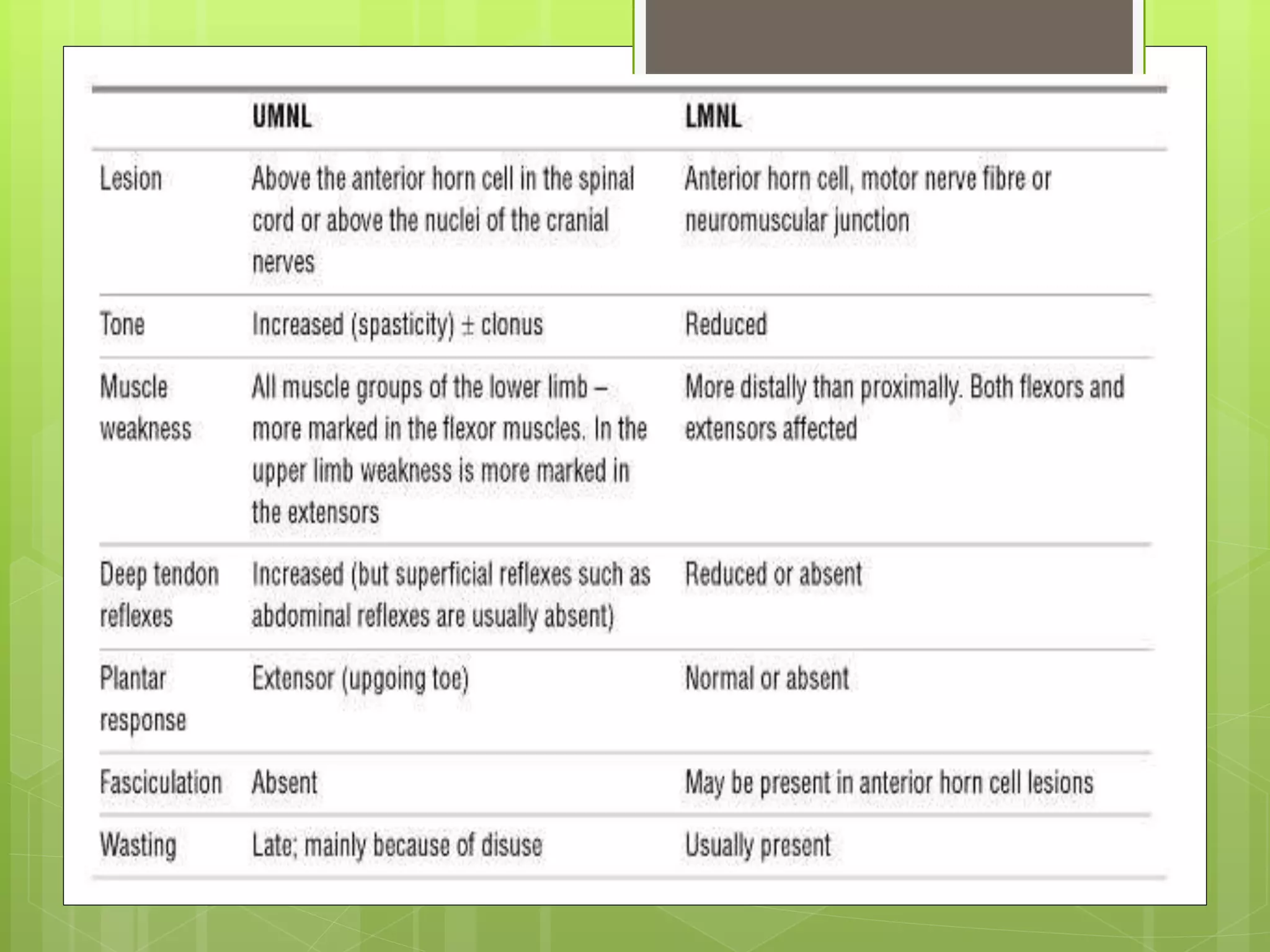
1. The document discusses the motor system and different types of motor neurons. It describes upper motor neurons that originate in the brain and carry signals to lower motor neurons.
2. Lower motor neurons are located in the spinal cord and brainstem and innervate skeletal muscles. Lesions or damage to lower motor neurons or their axons result in flaccid paralysis, muscle wasting, and loss of reflexes.
3. Specific conditions that damage lower motor neurons or their connections to muscles are also mentioned, including polio and peripheral neuropathies. Tests for lower motor neuron lesions include assessing for muscle fasciculations and reactions to electric stimulation.