Downloaded 1,695 times



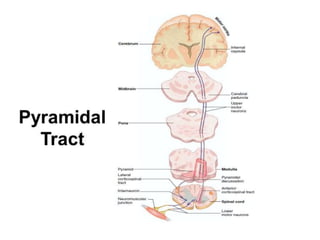
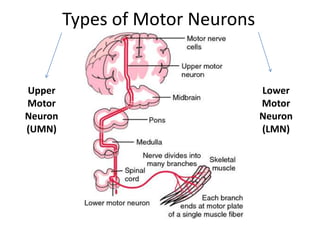

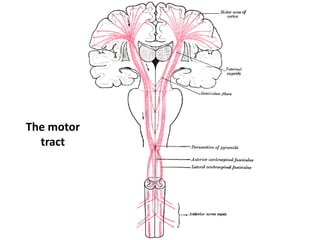

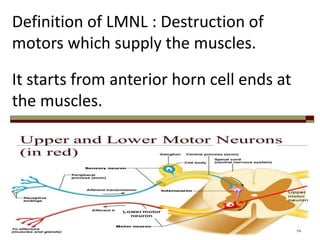









The document discusses the motor system, detailing upper motor neurons (UMN) and lower motor neurons (LMN), their functions, and lesions affecting them. It outlines the physiology of motor pathways, symptoms of motor neuron lesions, and the impact of various conditions on muscle movement and control. Treatment approaches for muscle impairment due to these lesions, including exercise, medical interventions, and rehabilitation are also covered.










































































