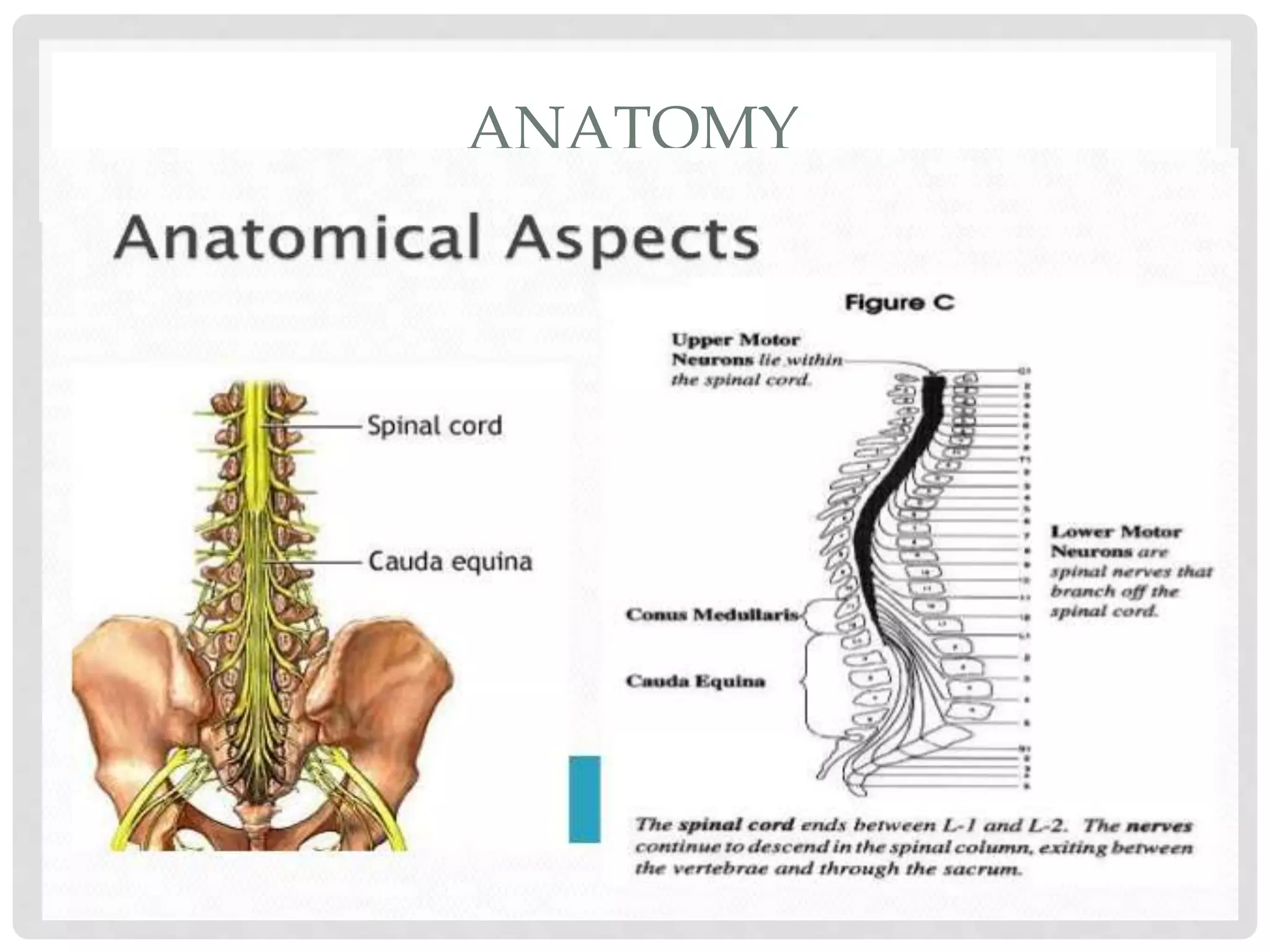
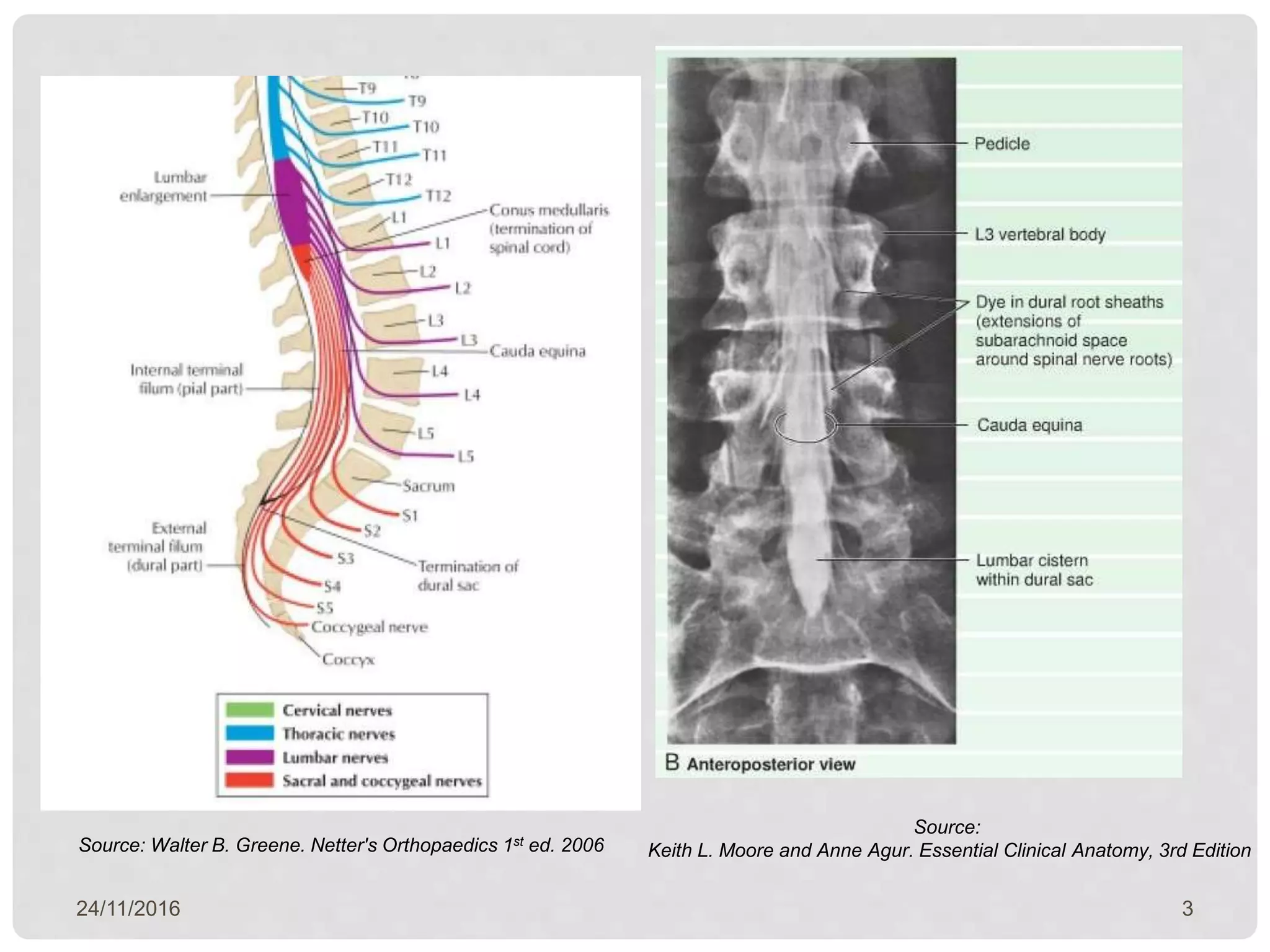
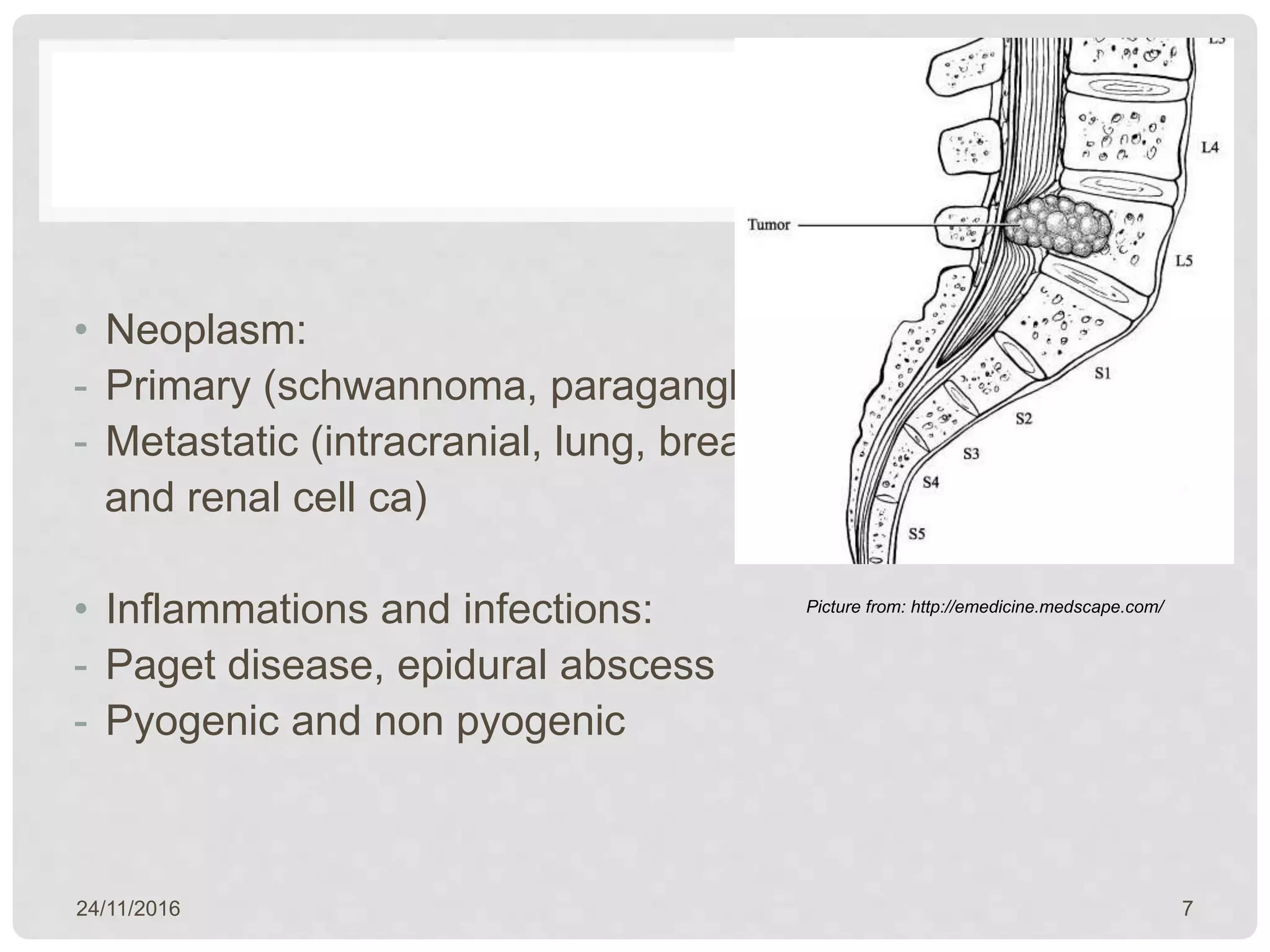
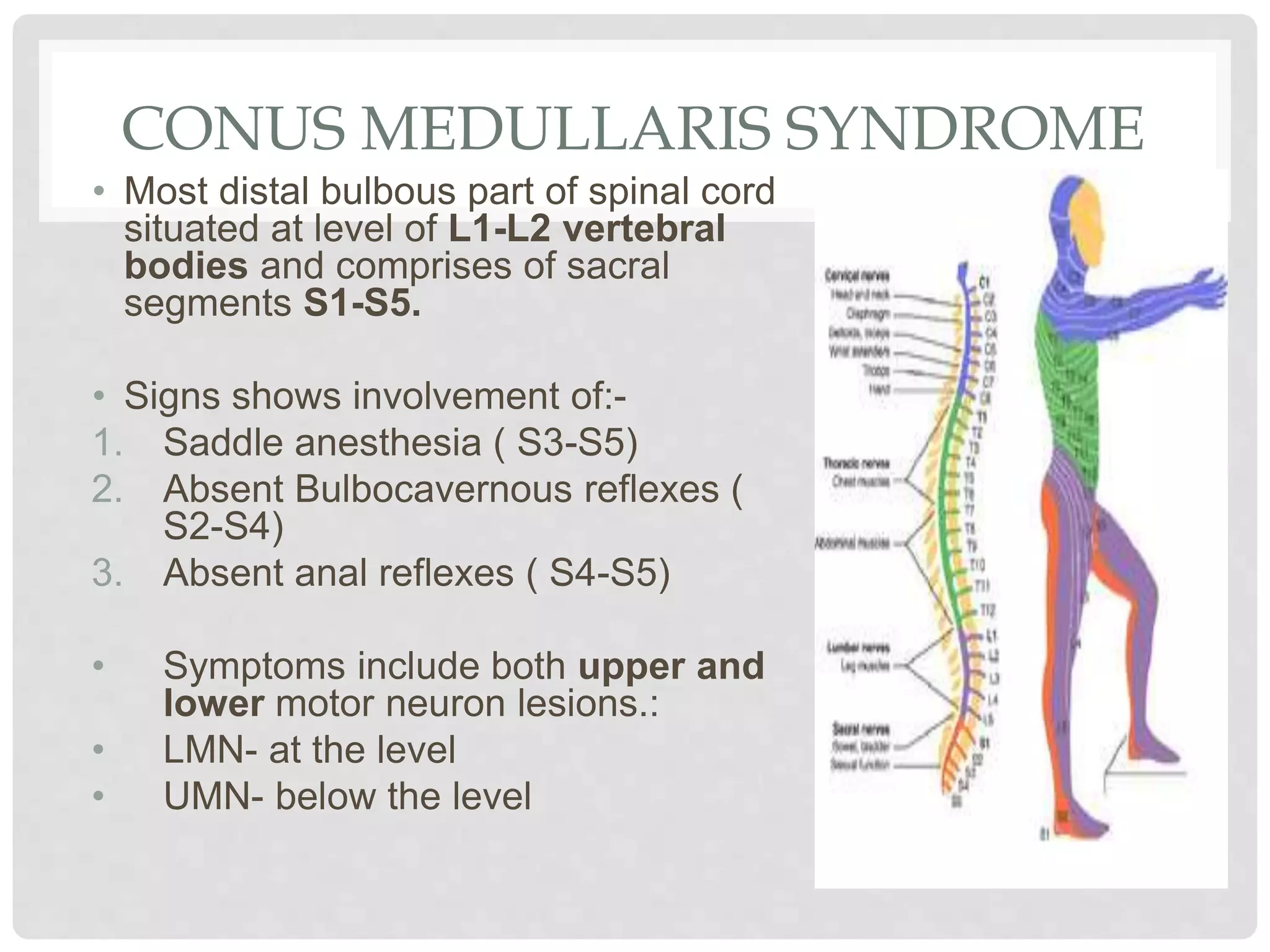
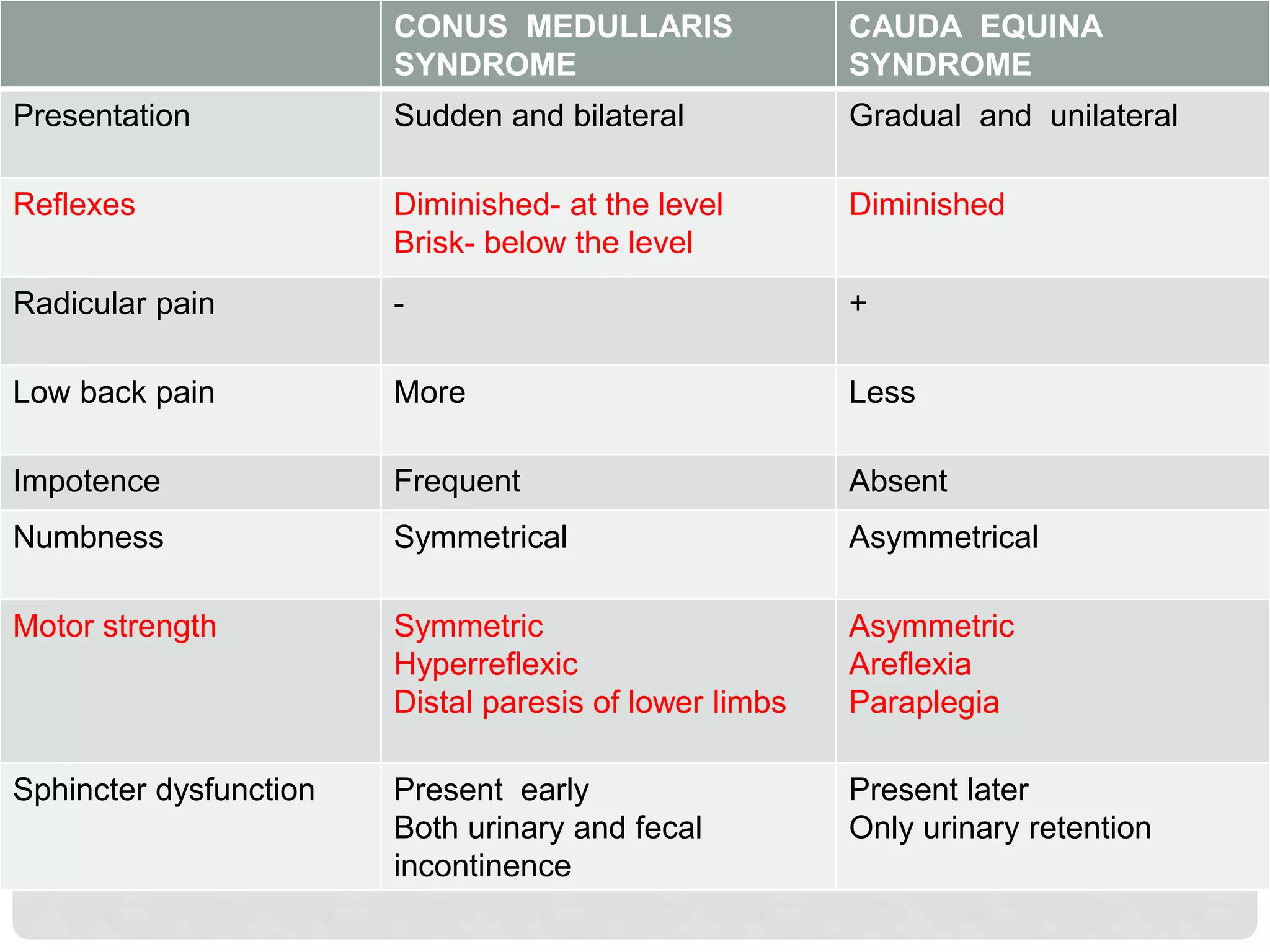
- The conus medullaris syndrome involves compression of the lower end of the spinal cord known as the conus medullaris, located around the L1-L2 vertebrae. This can result in saddle anesthesia, absent bulbocavernous and anal reflexes, and both upper and lower motor neuron signs and symptoms below the level of compression.
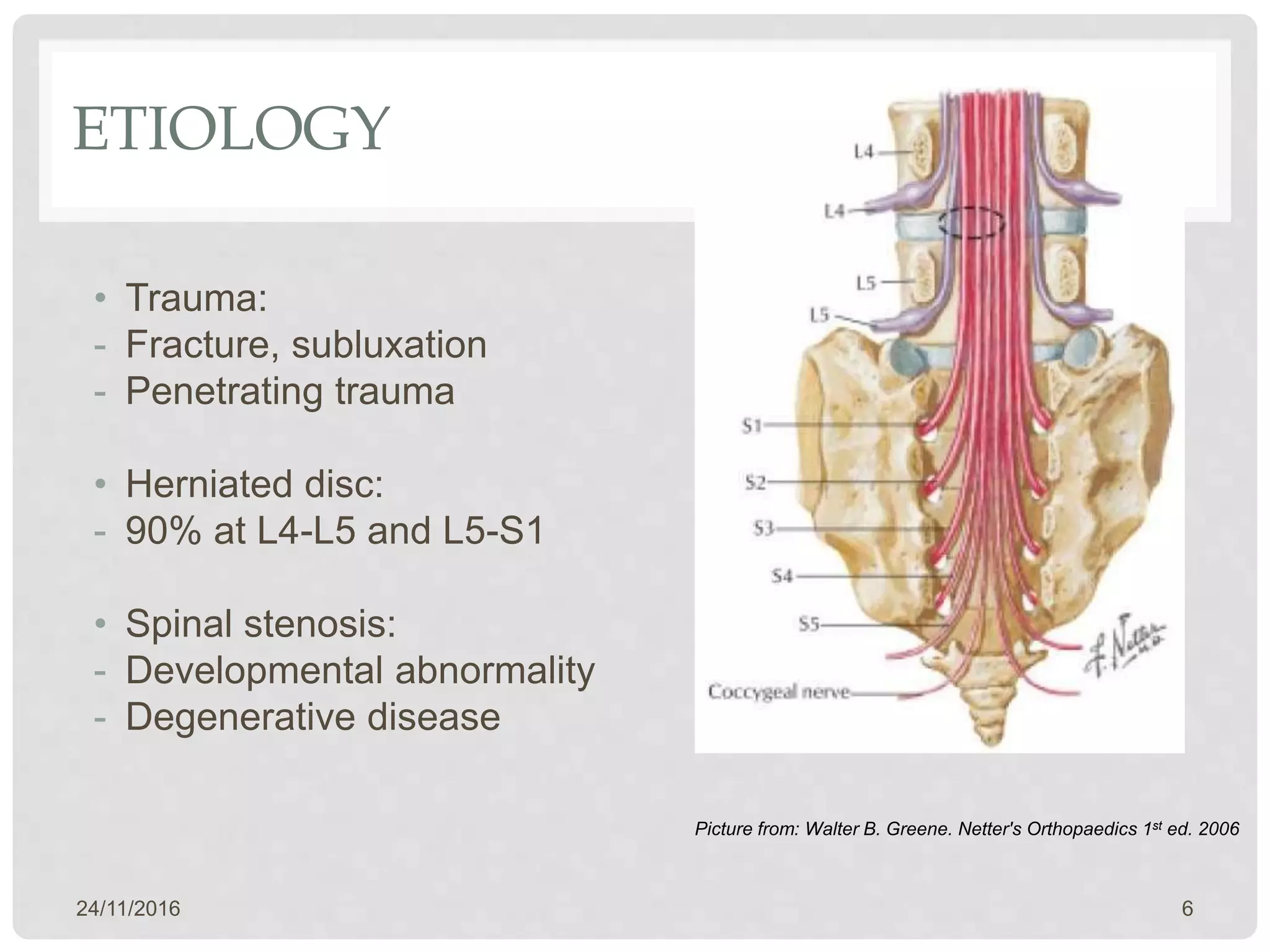
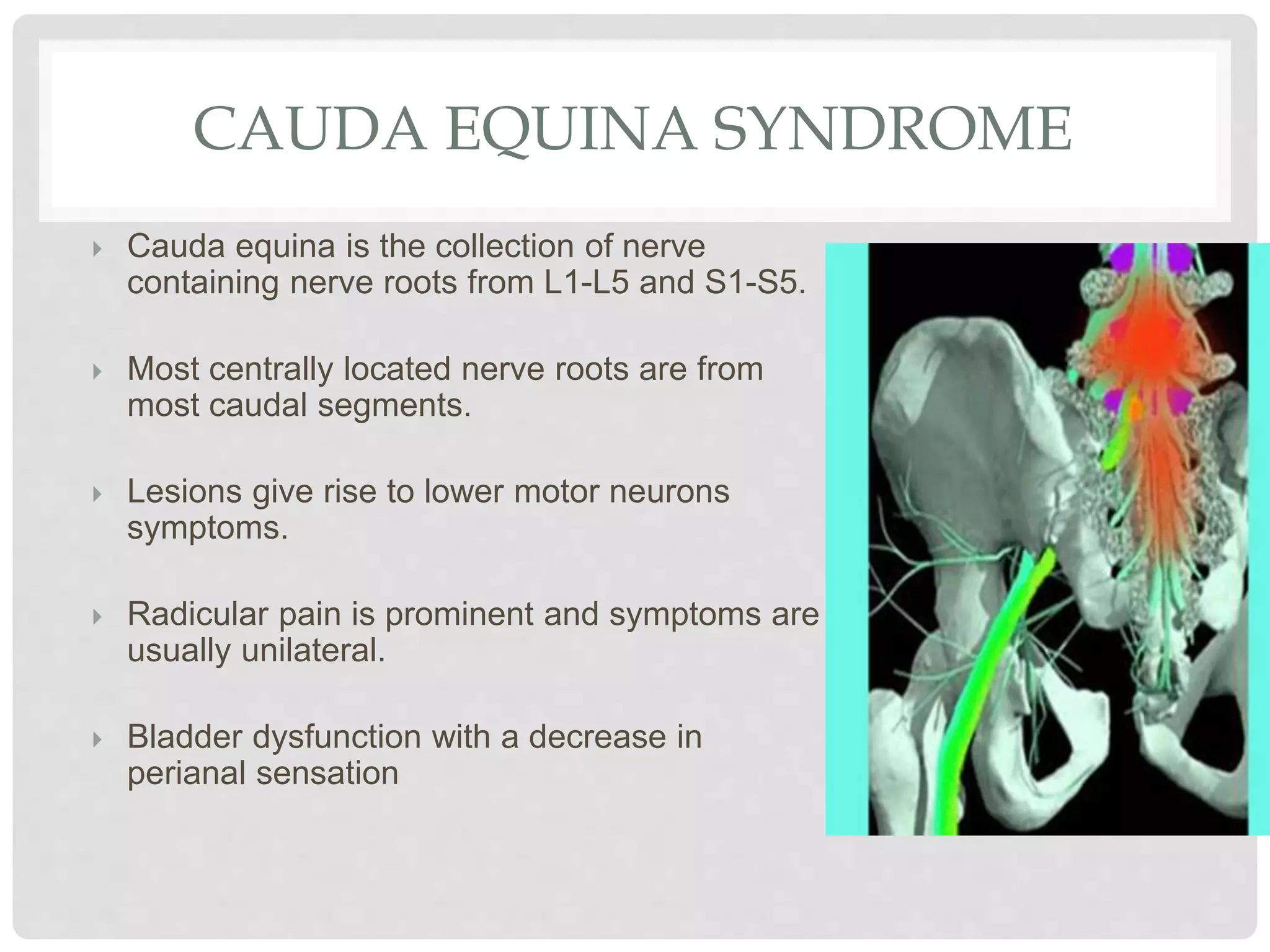
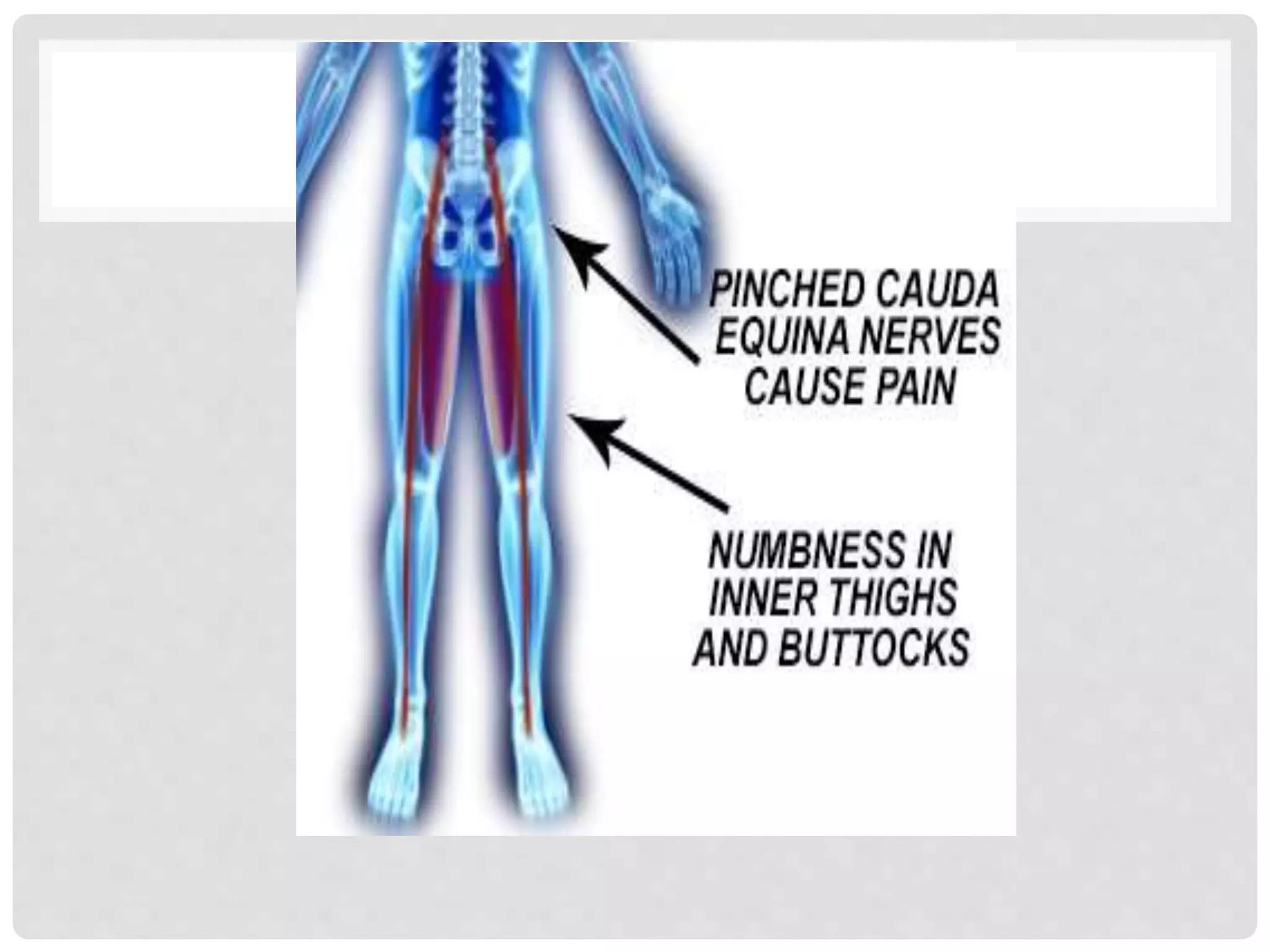
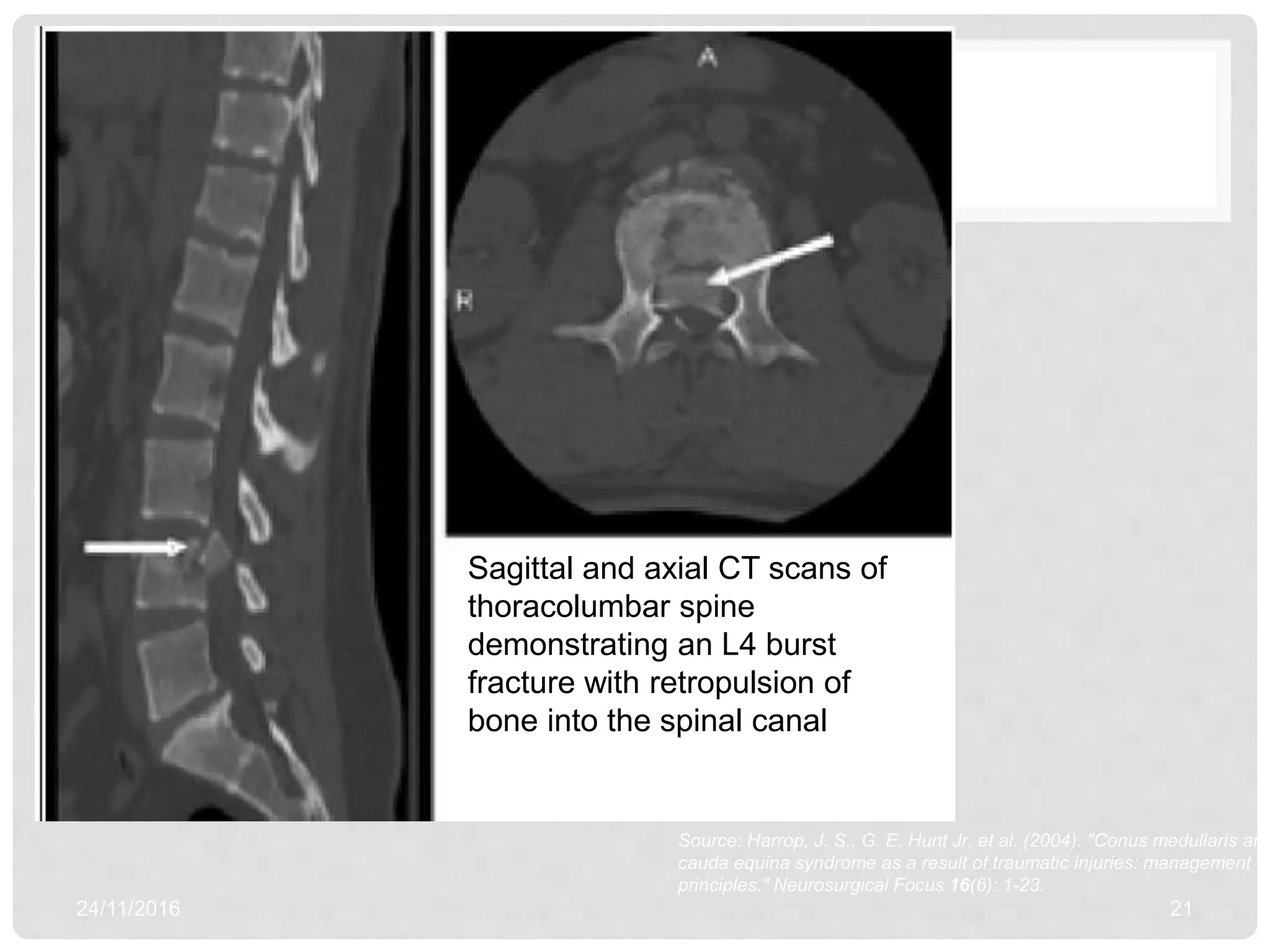
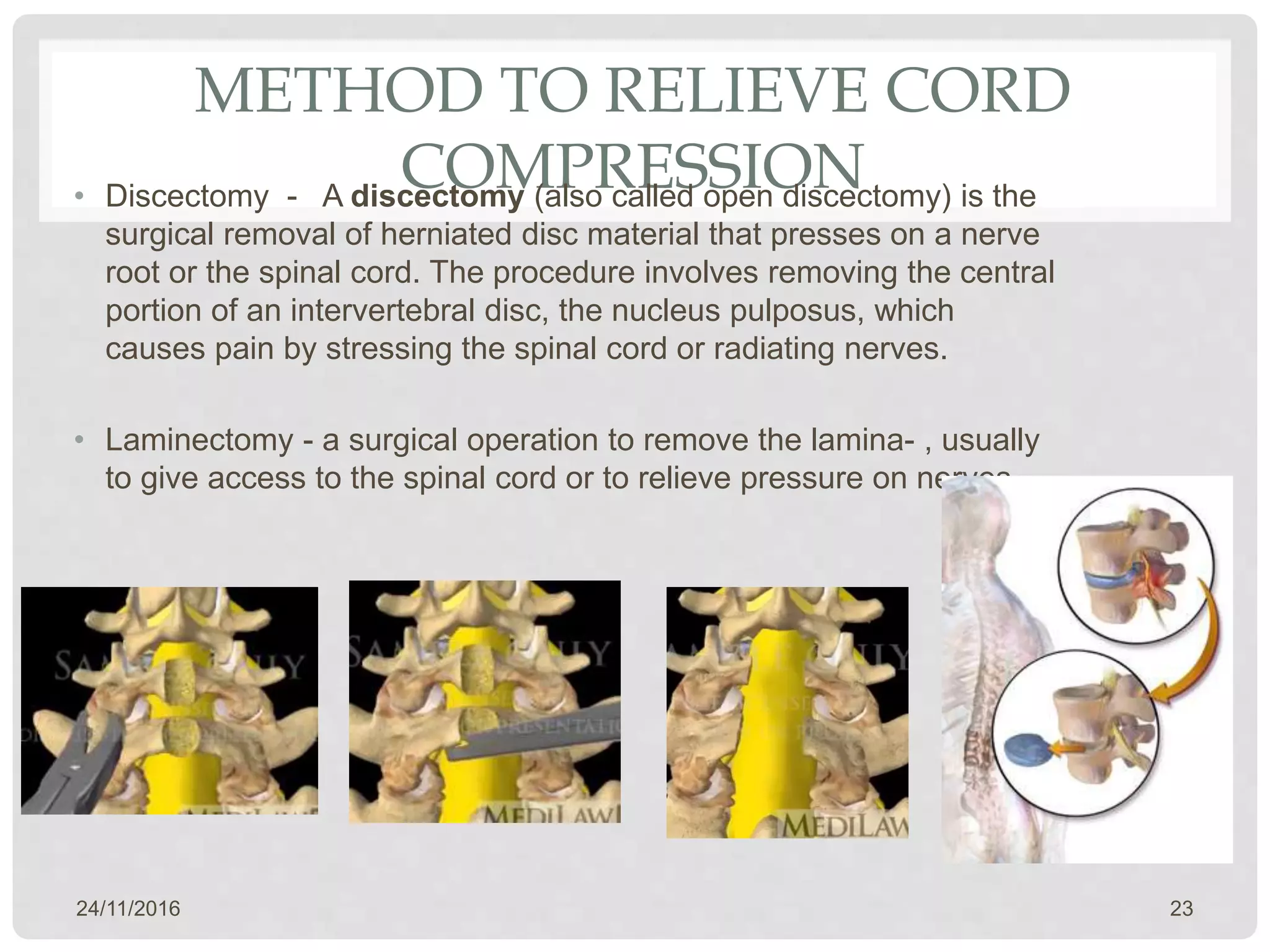
- The cauda equina syndrome involves compression of the bundle of spinal nerve roots in the lower back called the cauda equina. It can cause radicular pain, urinary retention, and asymmetric sensory loss. MRI is key for diagnosis and treatment involves decompression through procedures like discectomy, laminectomy, or corpectomy.
-