Downloaded 962 times


The document defines key epidemiological measures used to describe disease occurrence and impact, including prevalence, incidence, rates, and ratios. It provides examples of how to calculate and interpret these measures. The document concludes that prevalence describes the current disease burden, while incidence provides information on the risk of developing disease over time and is thus better suited for etiological studies.
Introduction to the speaker, Prof. Chen Yu-ming, and the topic of epidemiologic measures.
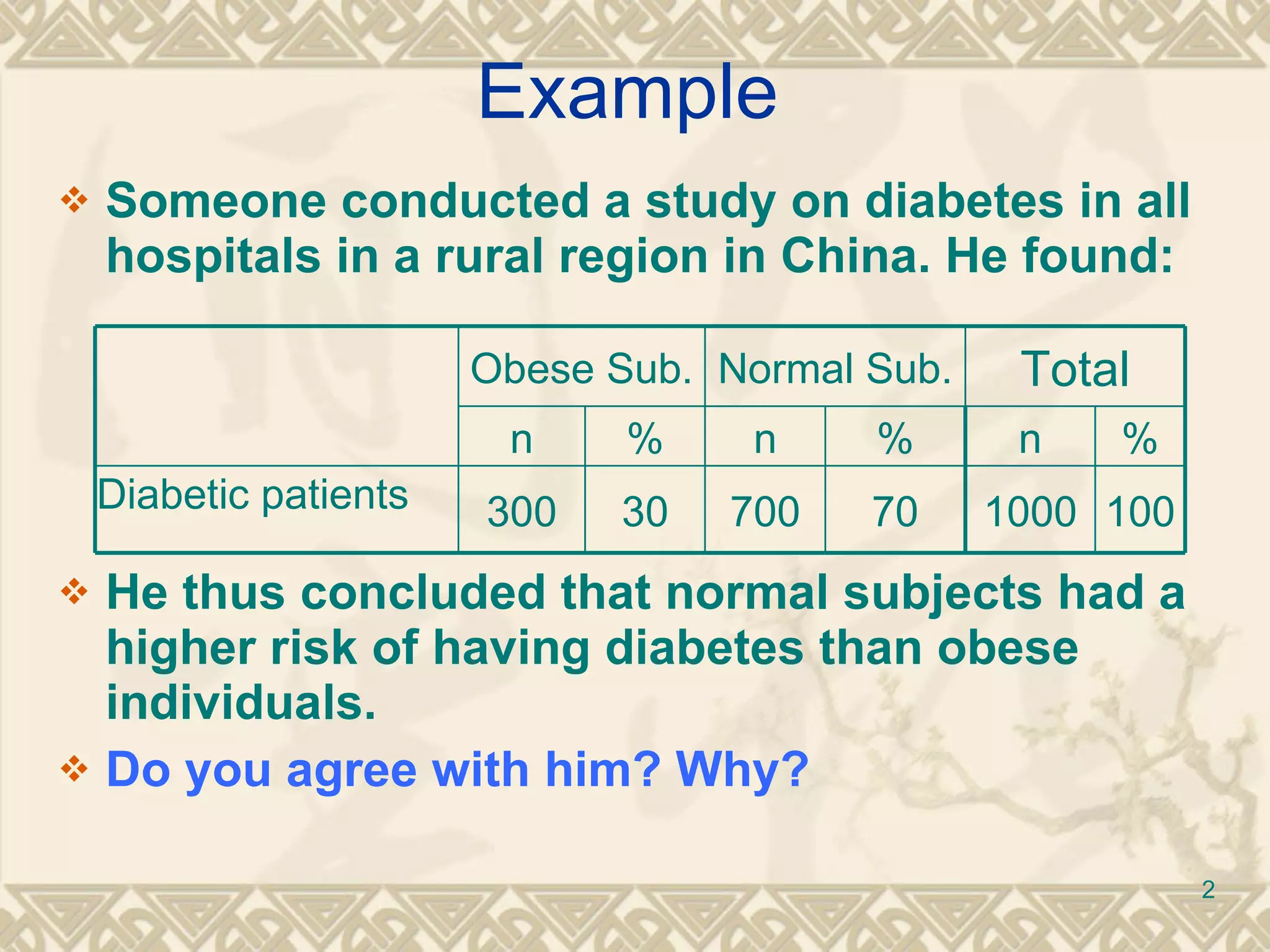
A study on diabetes showing a higher percentage of diabetic patients among normal subjects over obese.
Overview of lesson objectives including definitions of ratios, proportions, rates, incidence, and prevalence.
Definitions and usages of ratios, proportions, rates, and measures of disease occurrence including prevalence and incidence.
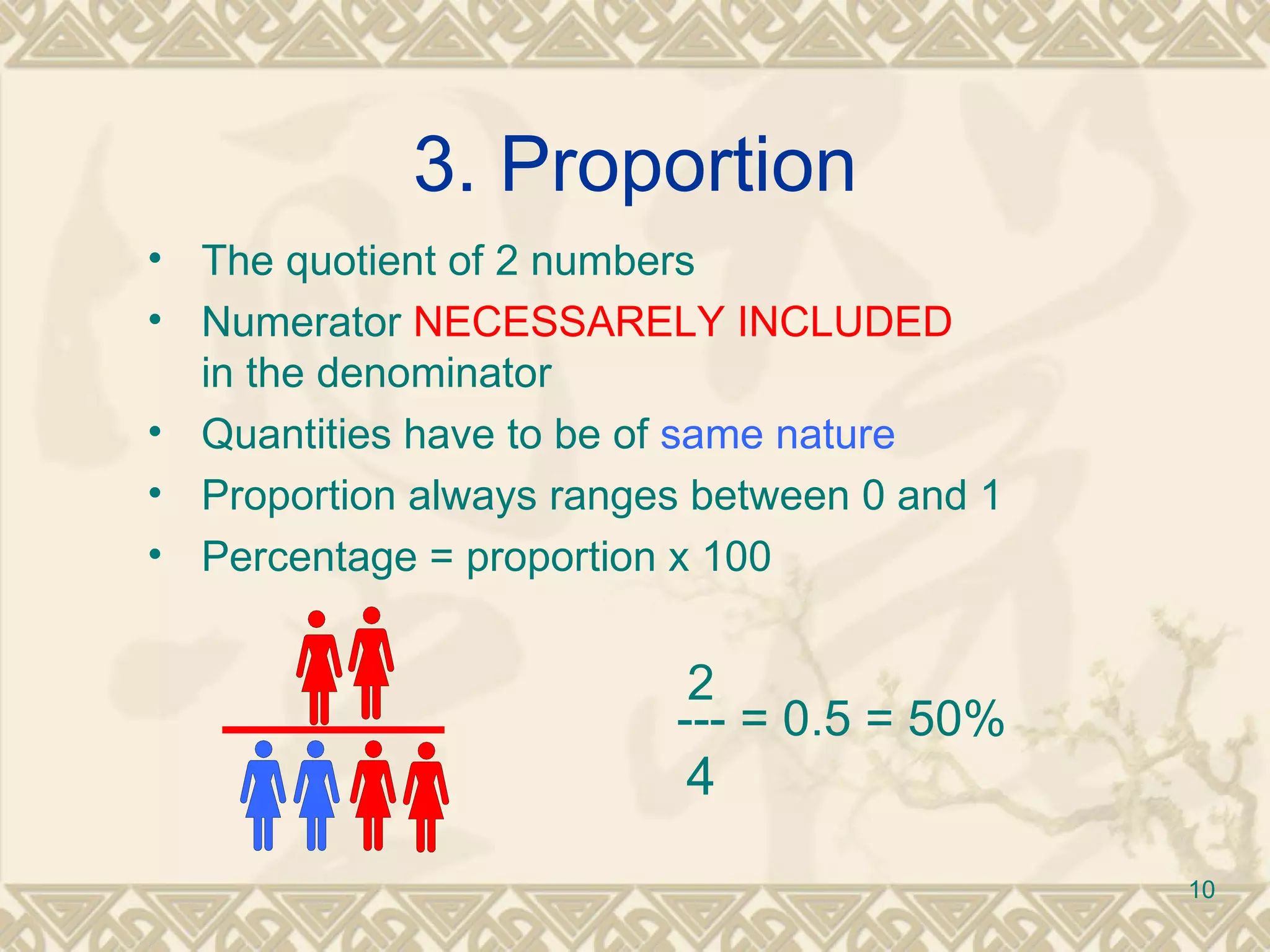
Detailed definitions of count, ratio, and proportion with examples of how they are utilized in epidemiology.
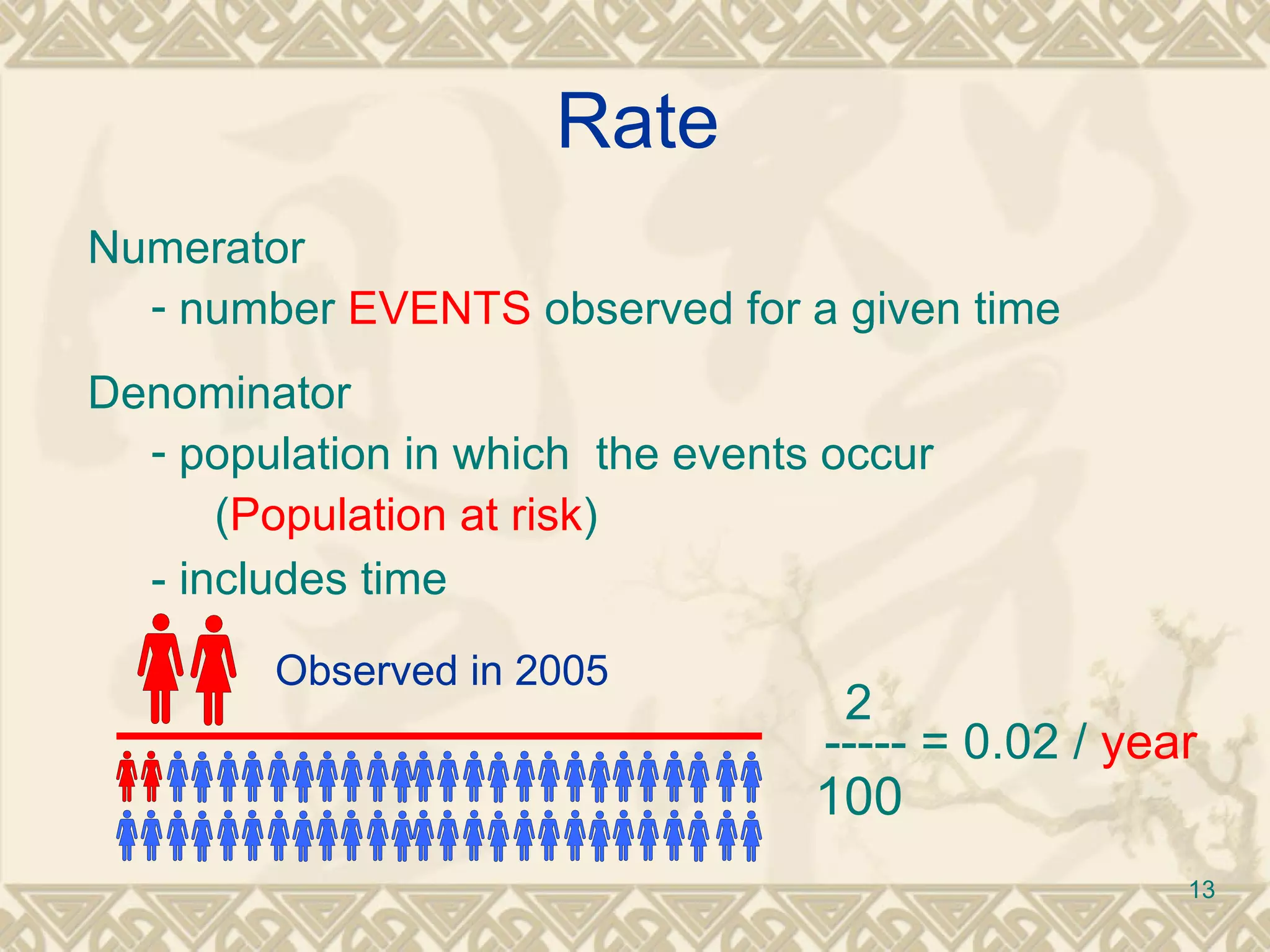
Definition of rate as a measure of the speed of occurrence of events, including key elements and examples.
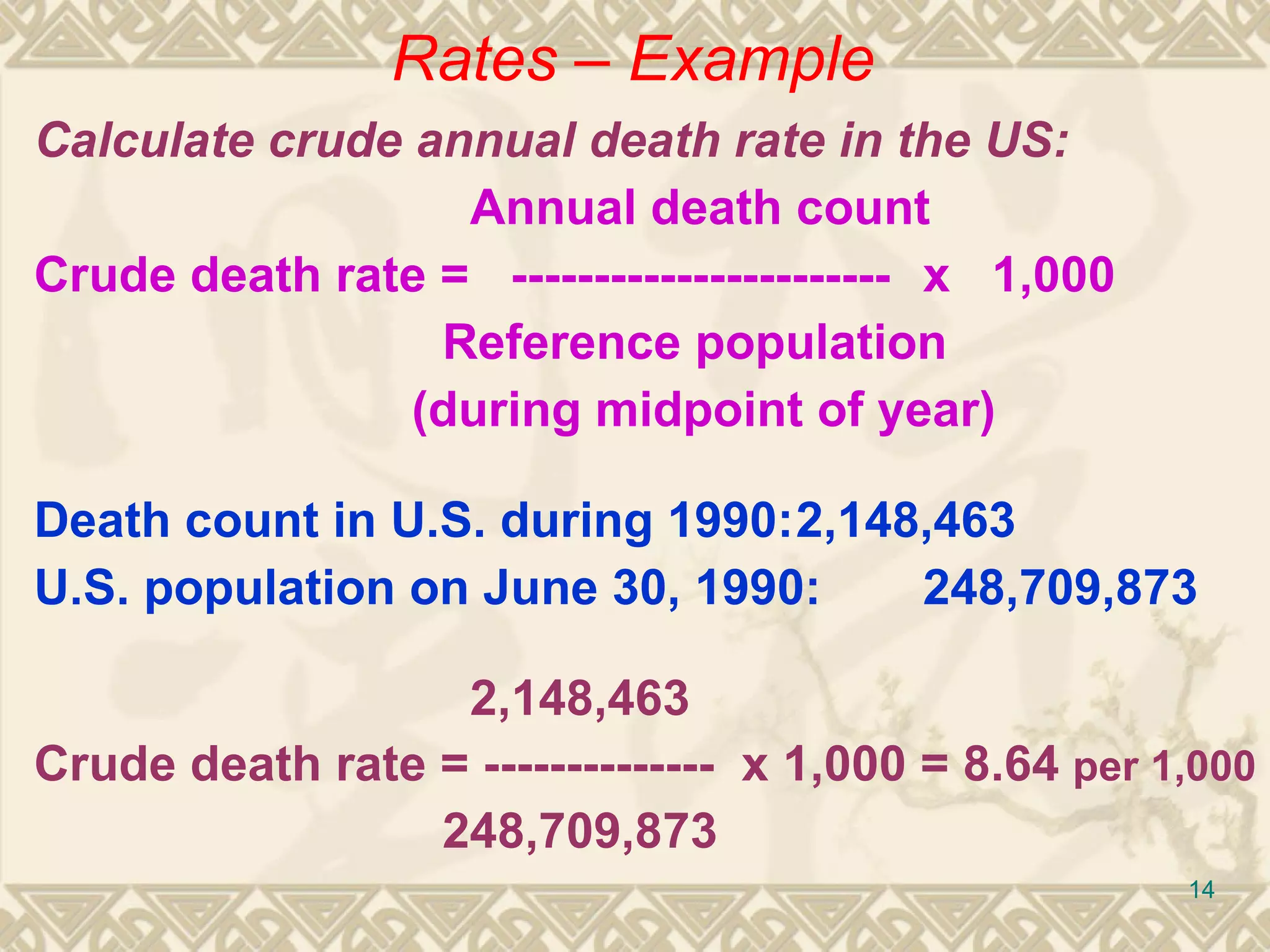
Explanation and example of calculating the crude annual death rate using U.S. statistics.
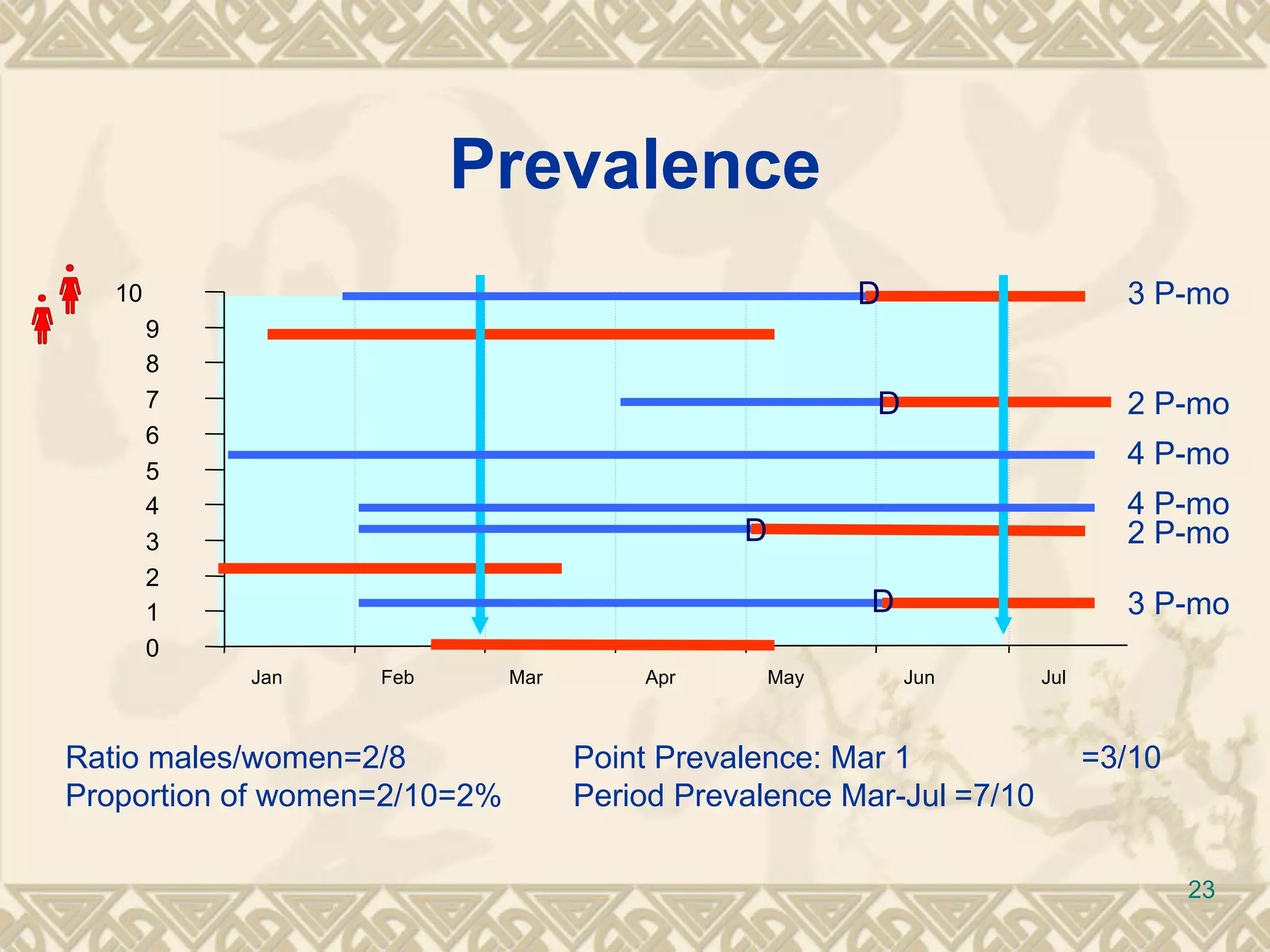
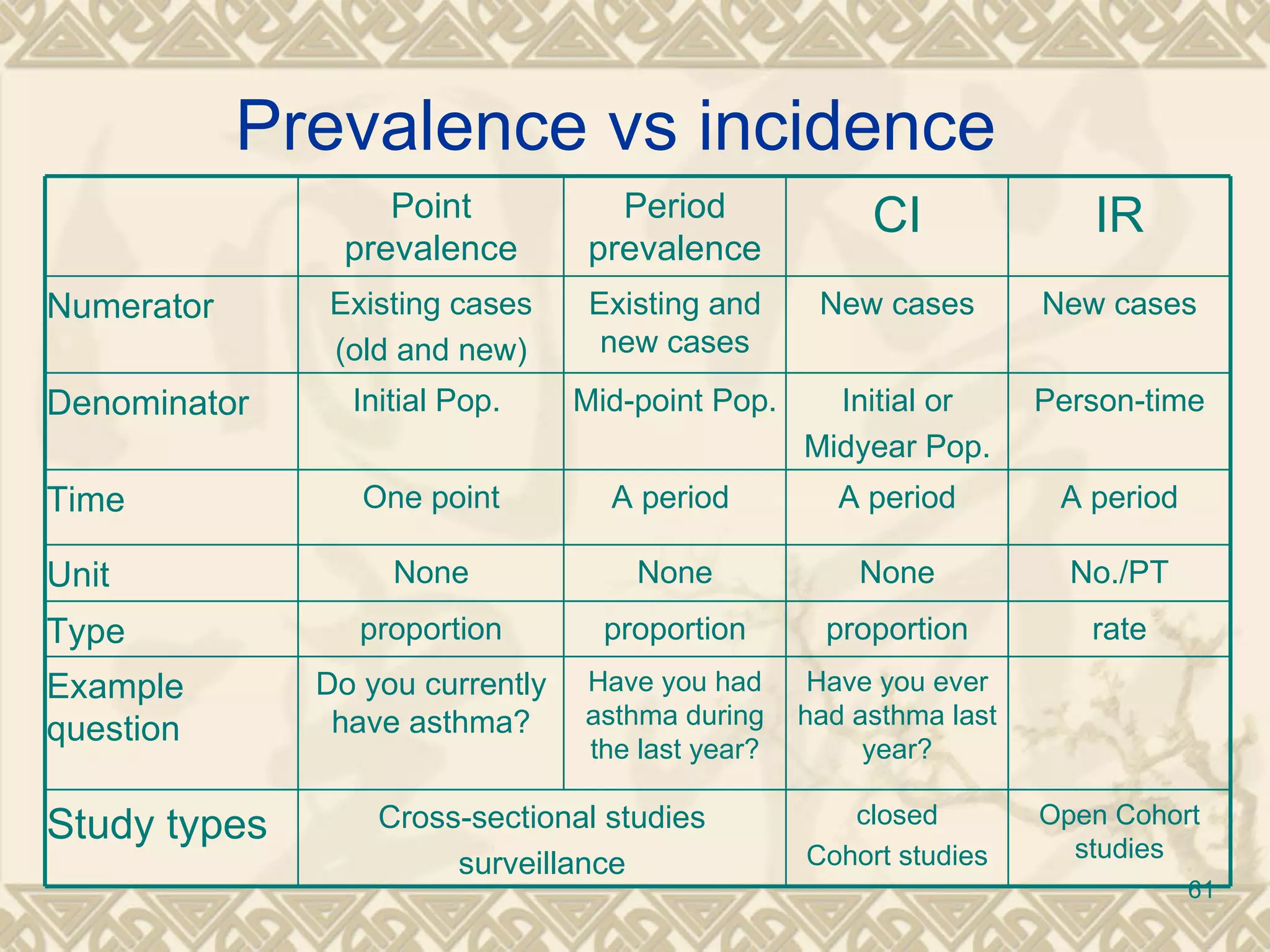
Understanding morbidity through prevalence types, definitions, and calculation examples.
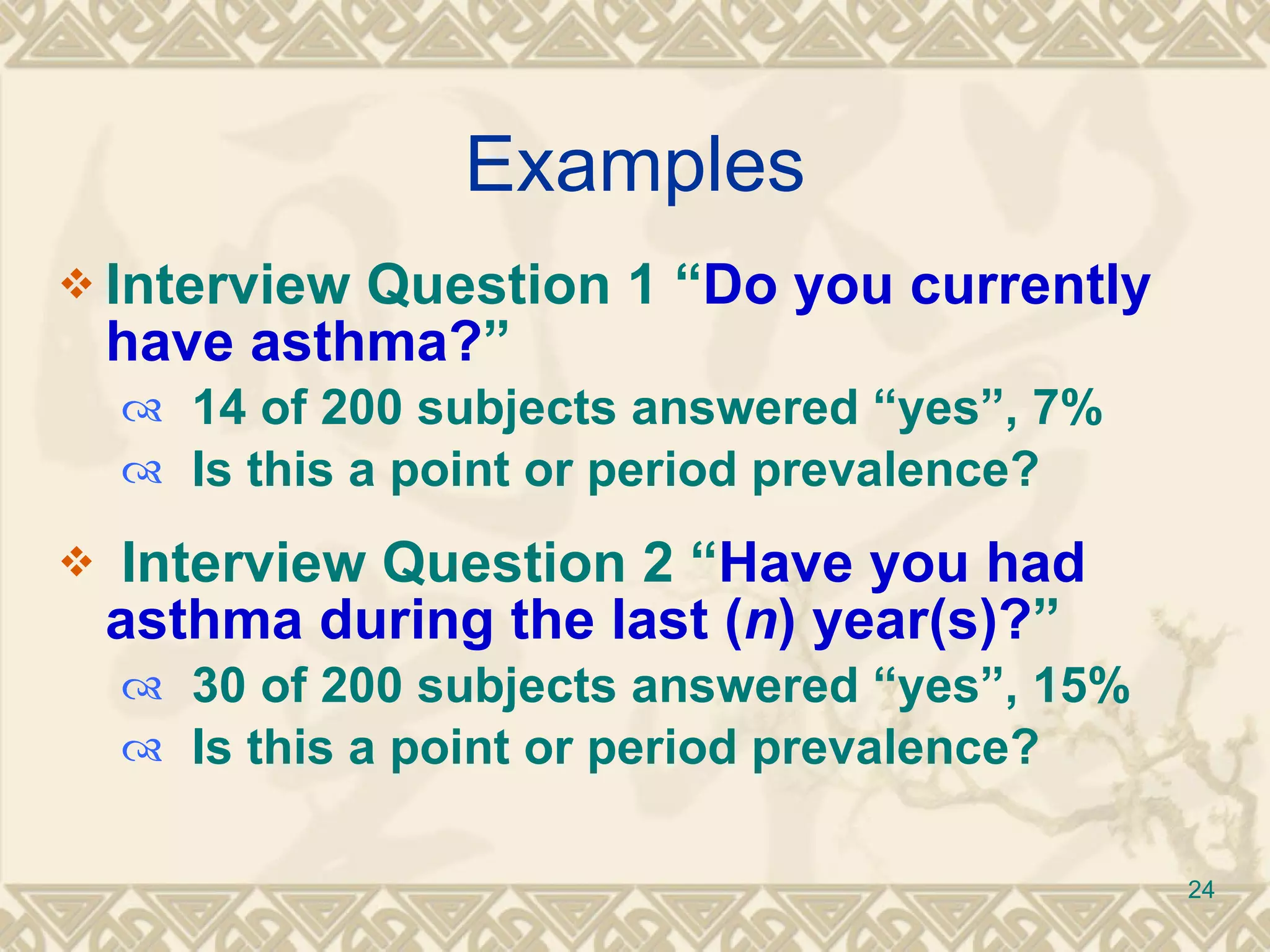
Components and types of prevalence including definitions, examples, and clinical implications.
Discussion of limitations regarding prevalence as an epidemiological measure and its suitability.
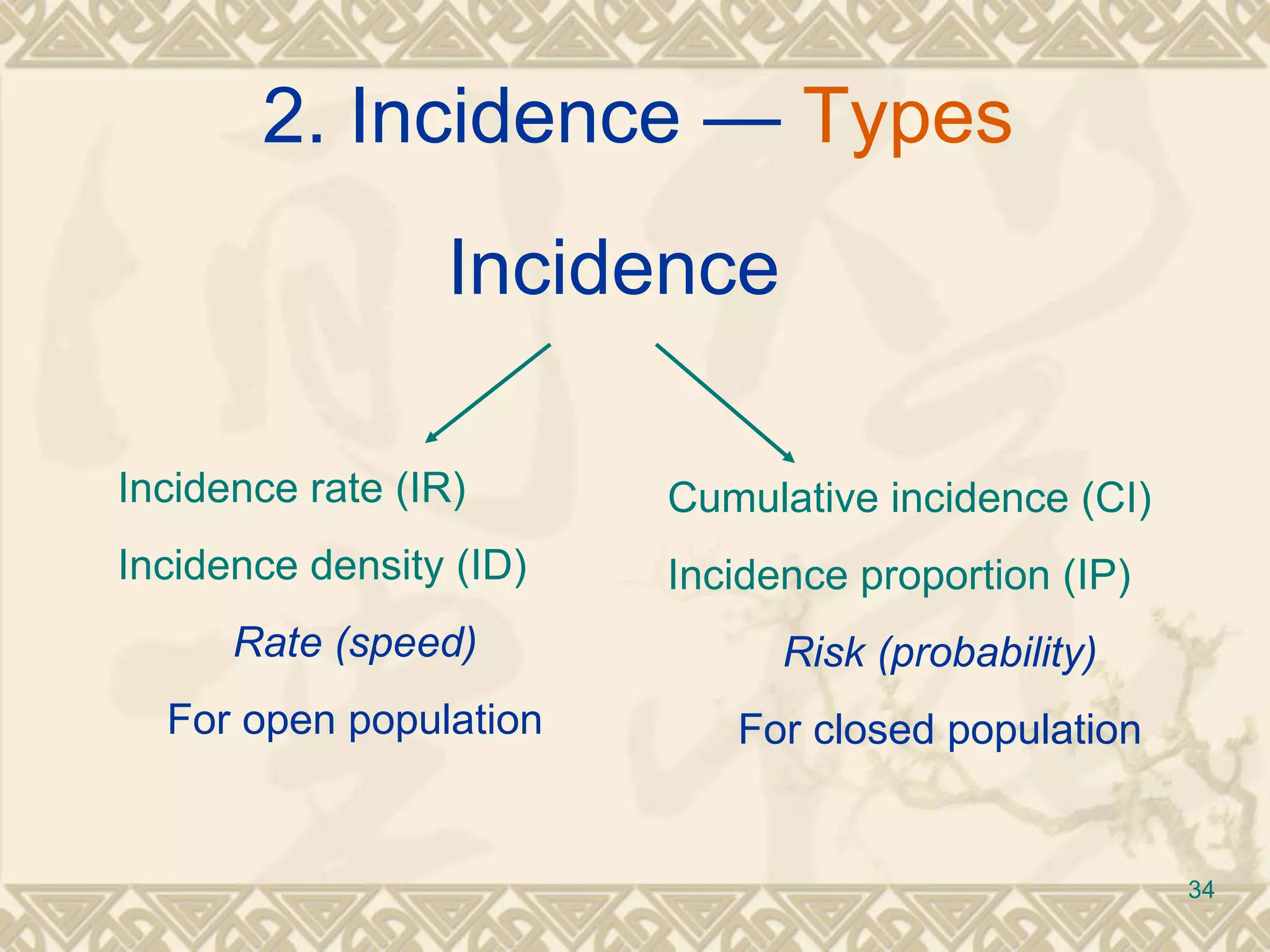
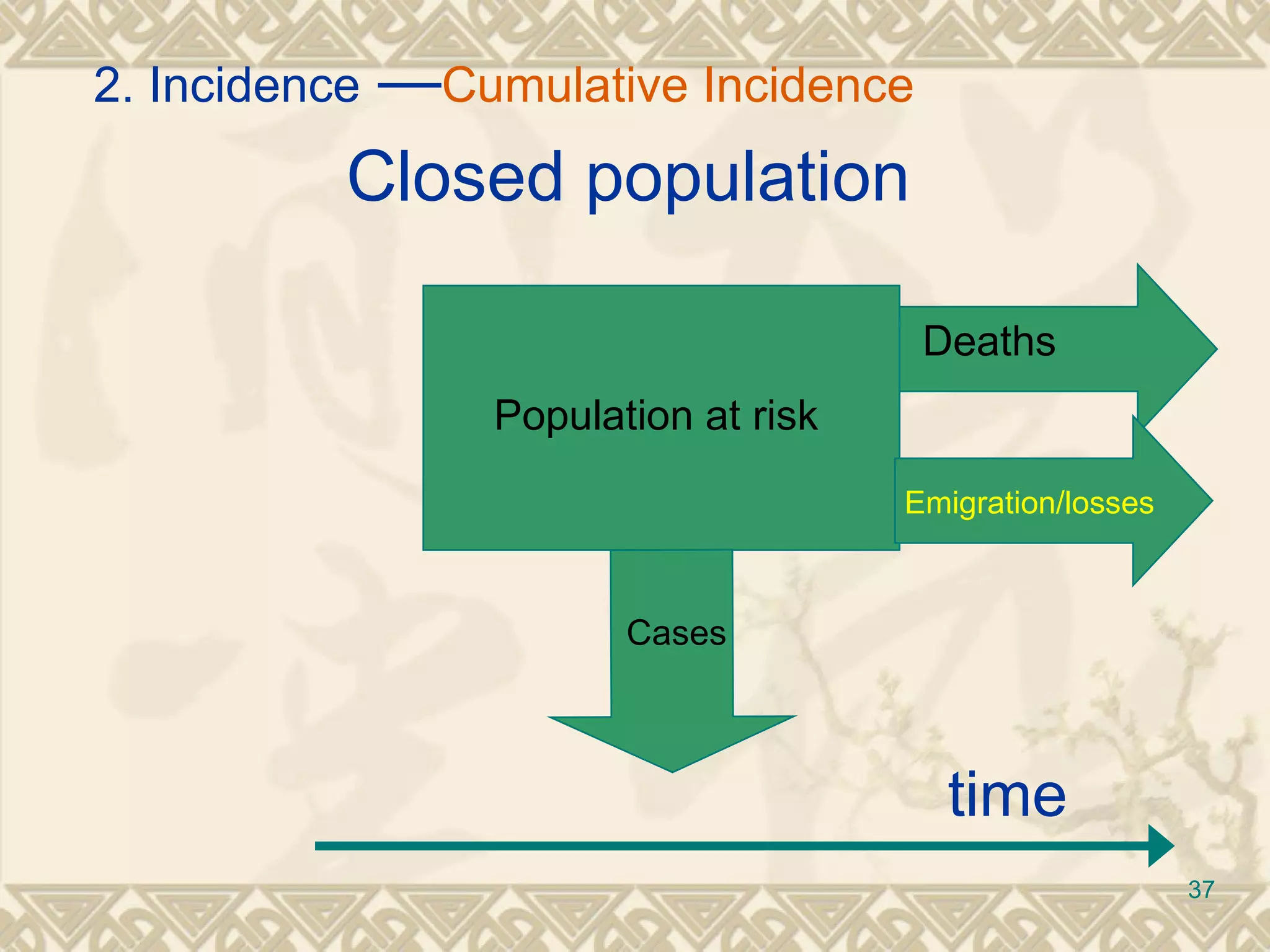
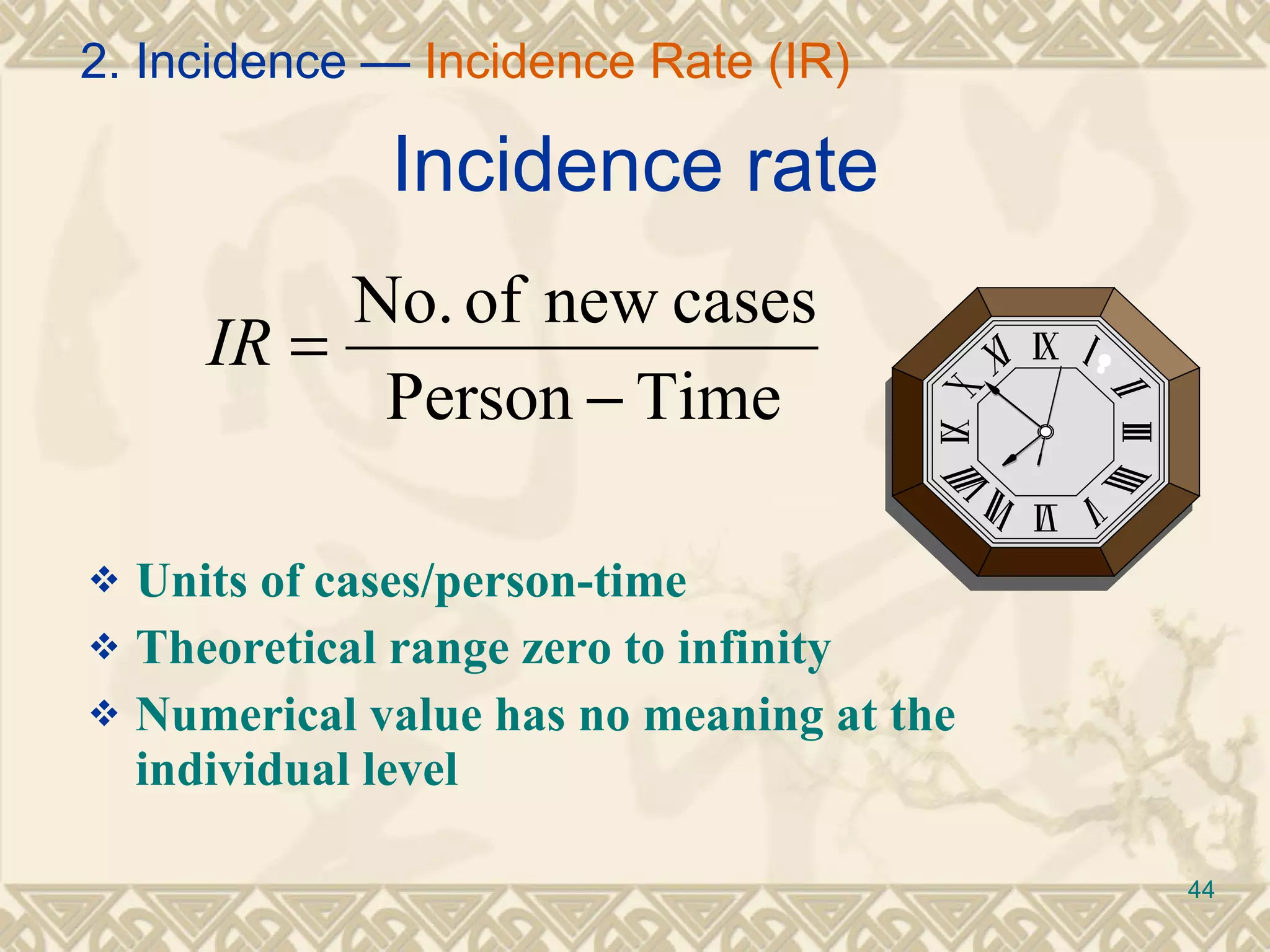
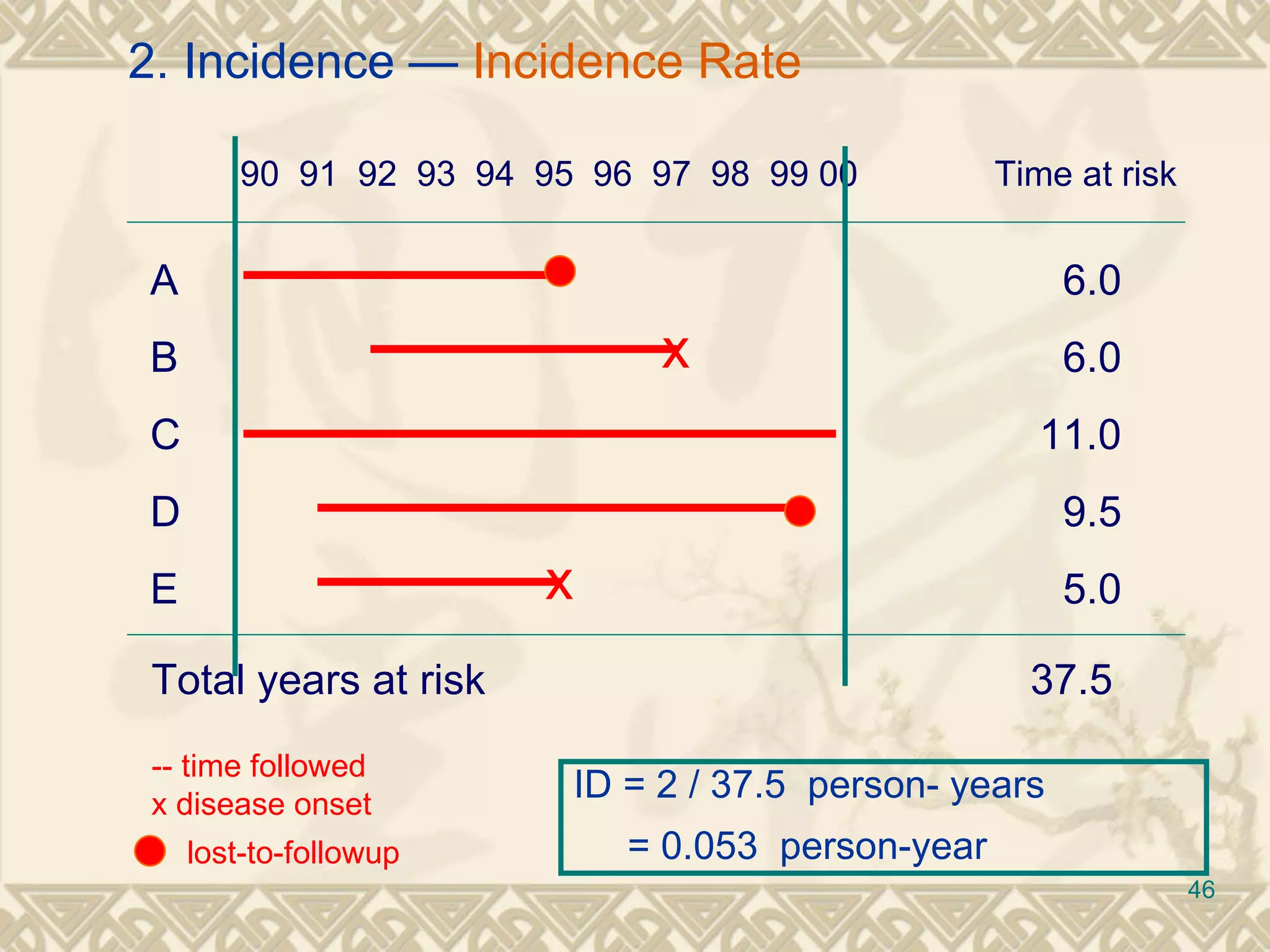
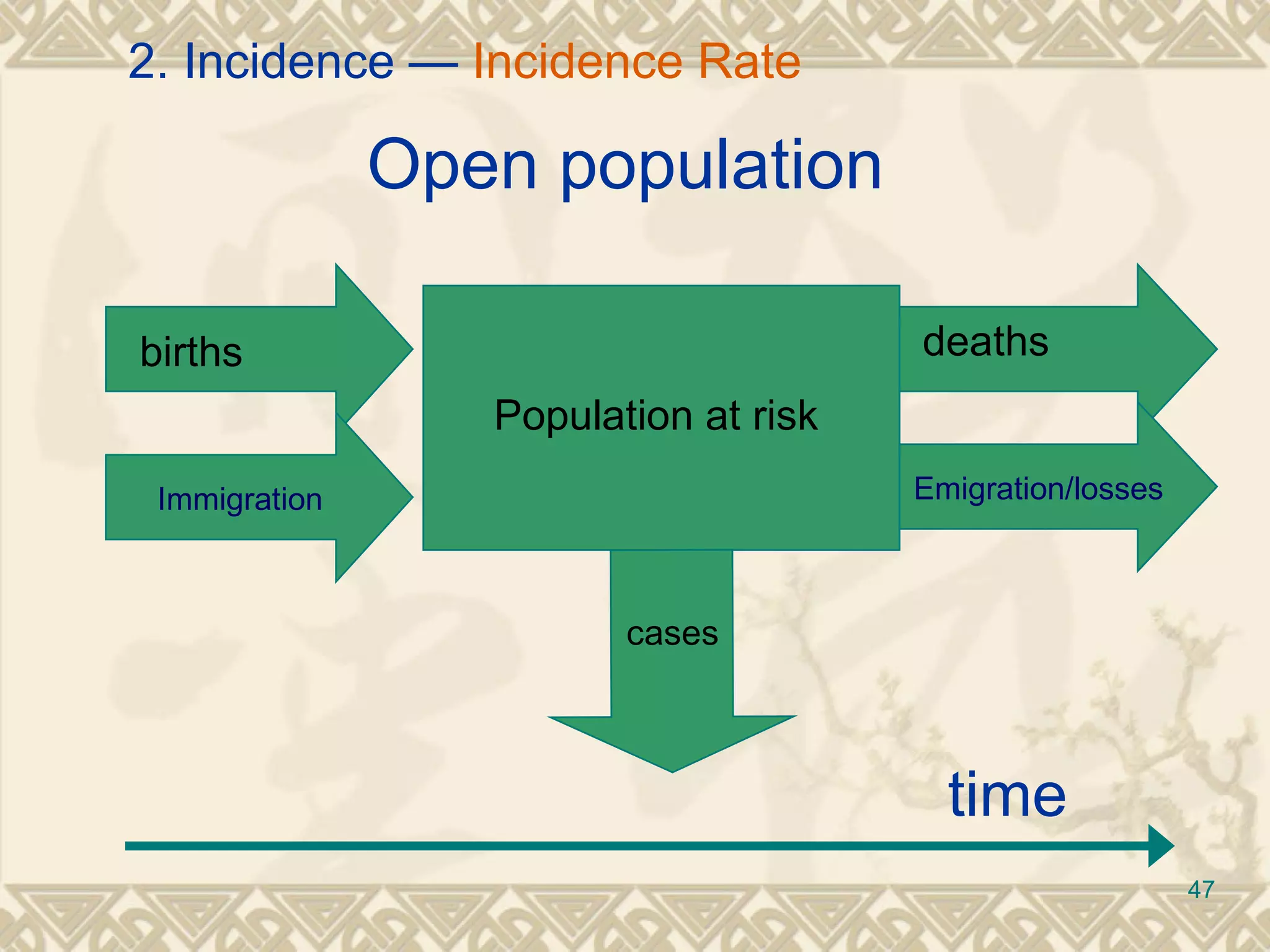
Definition of incidence and its key elements, including how it is calculated and population at risk factors.
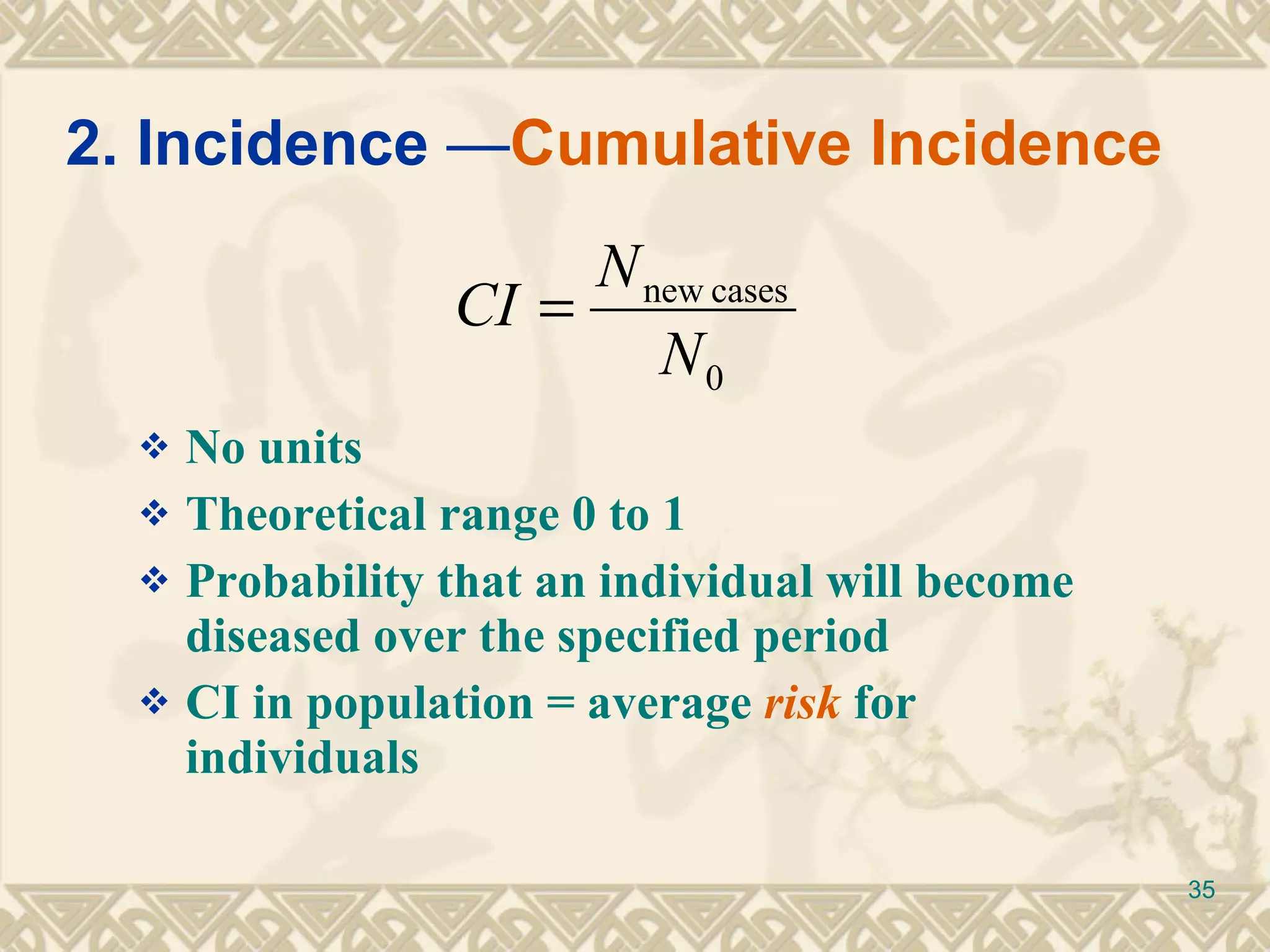
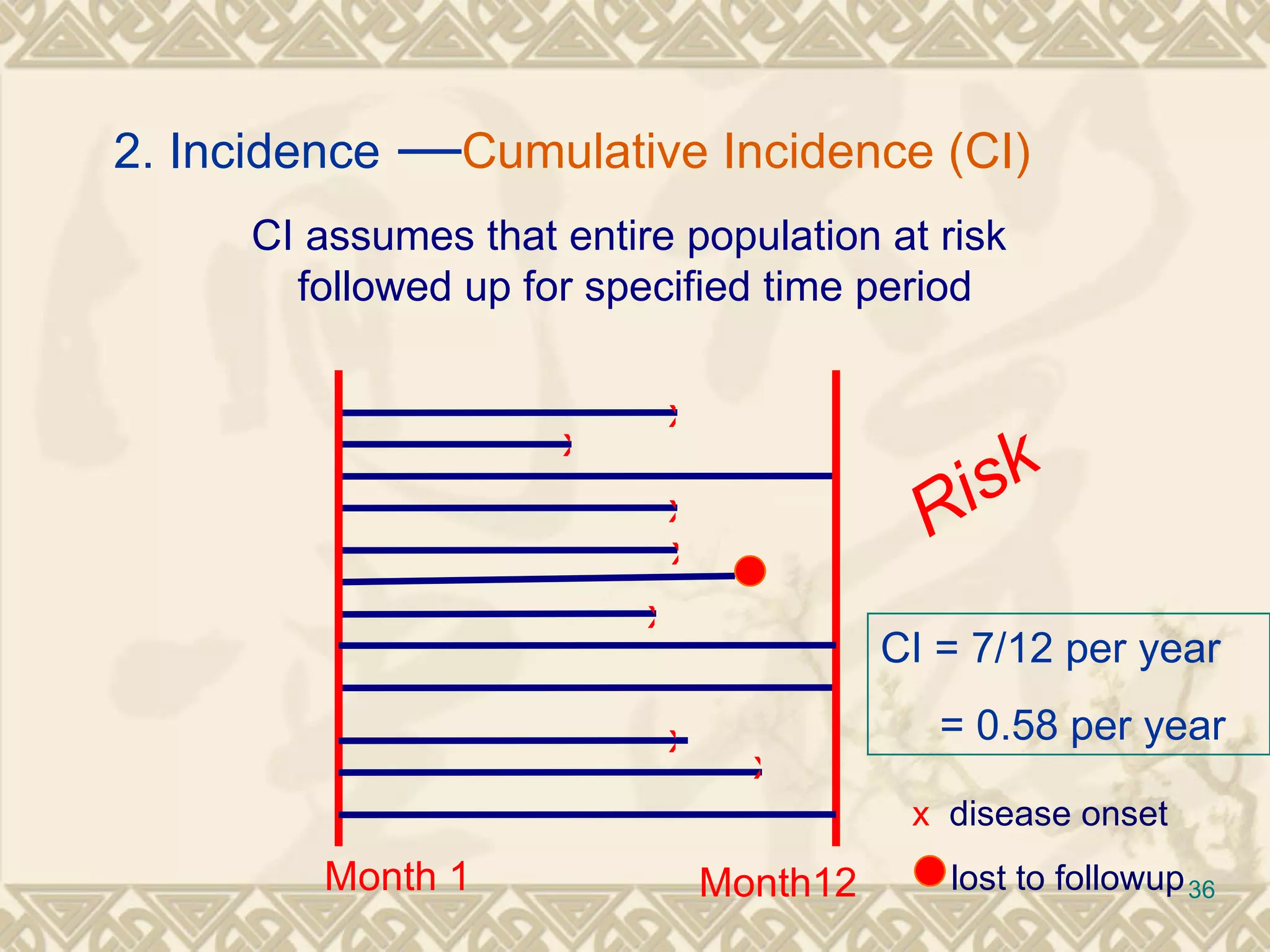
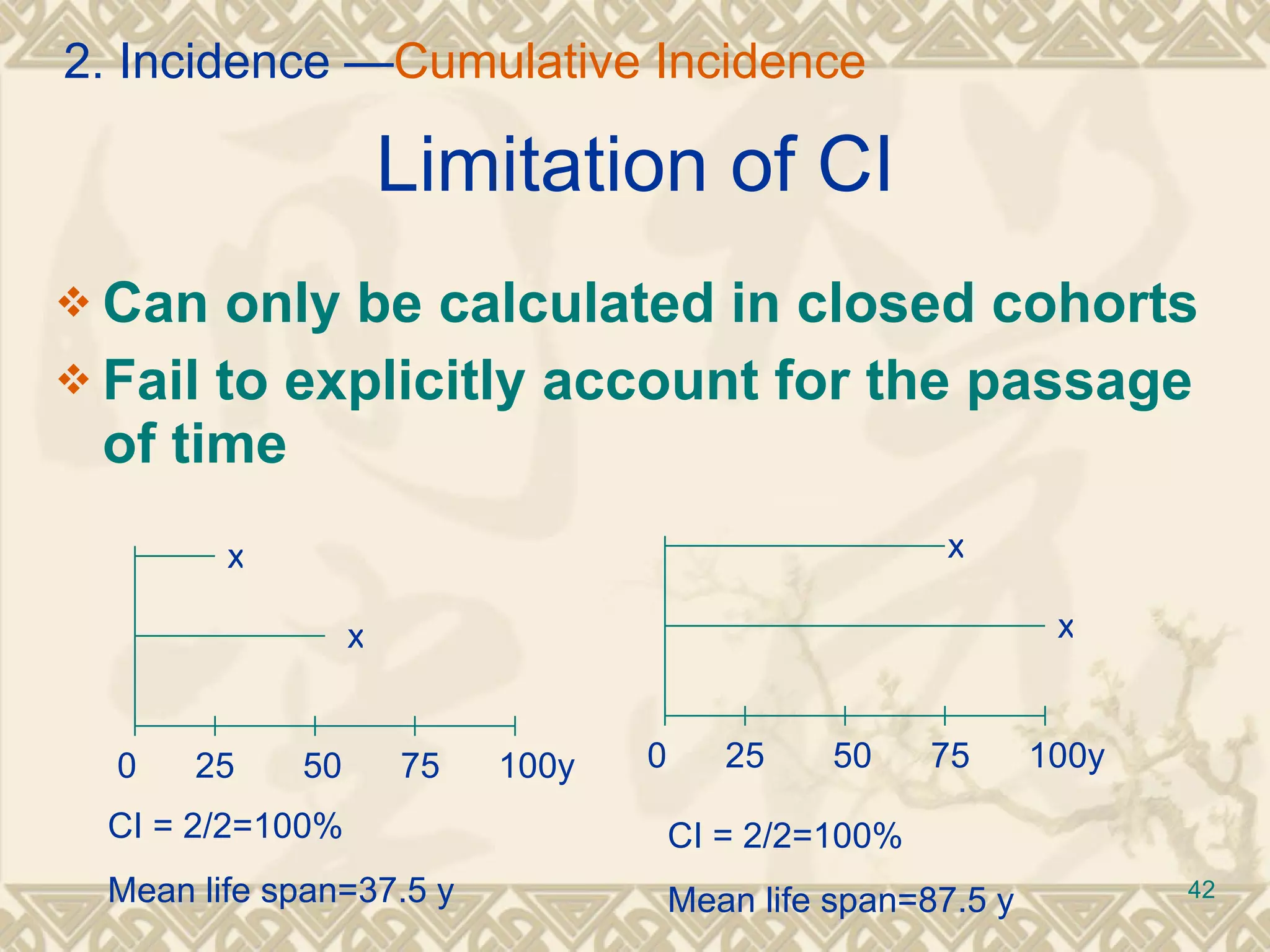
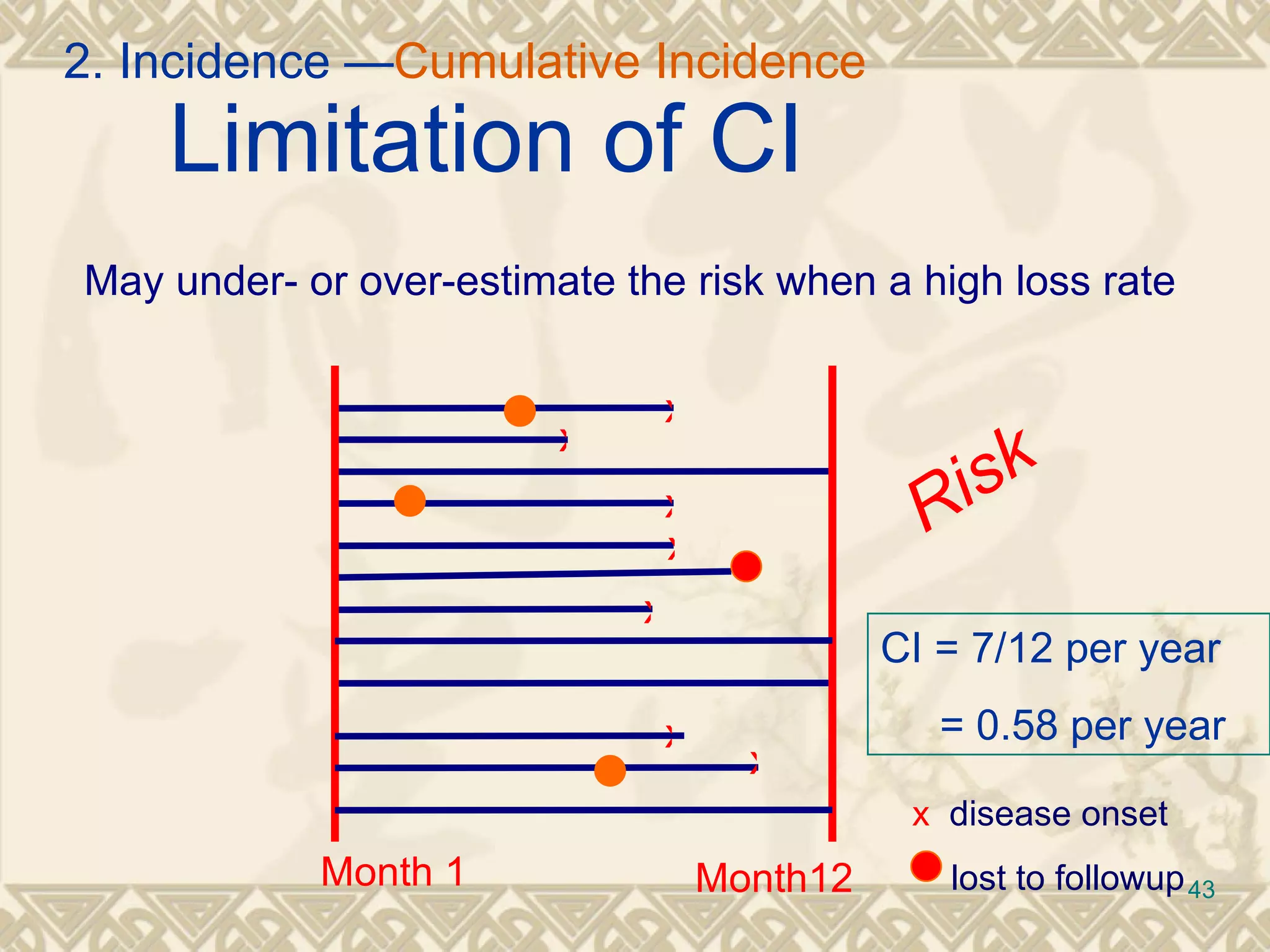
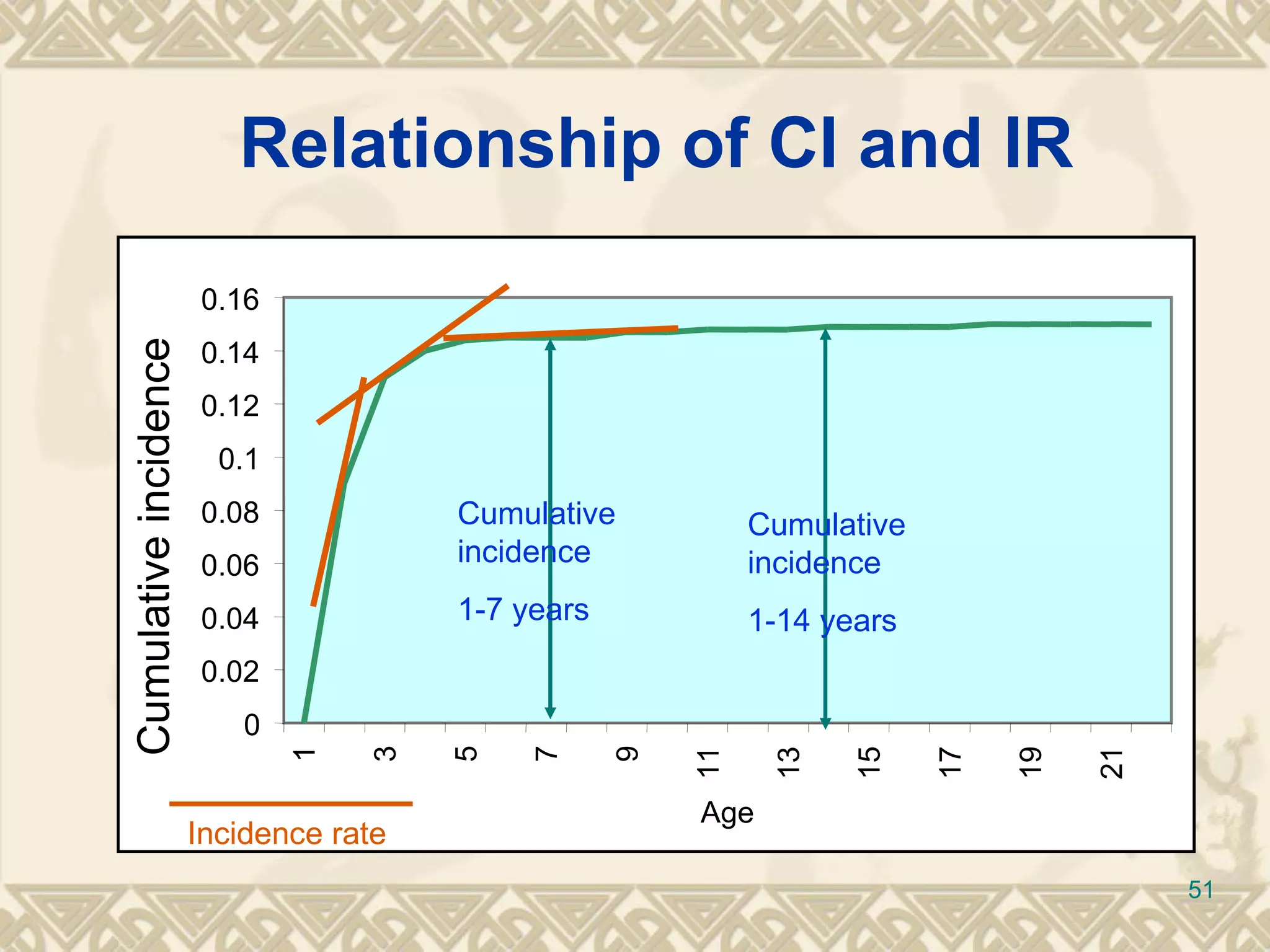
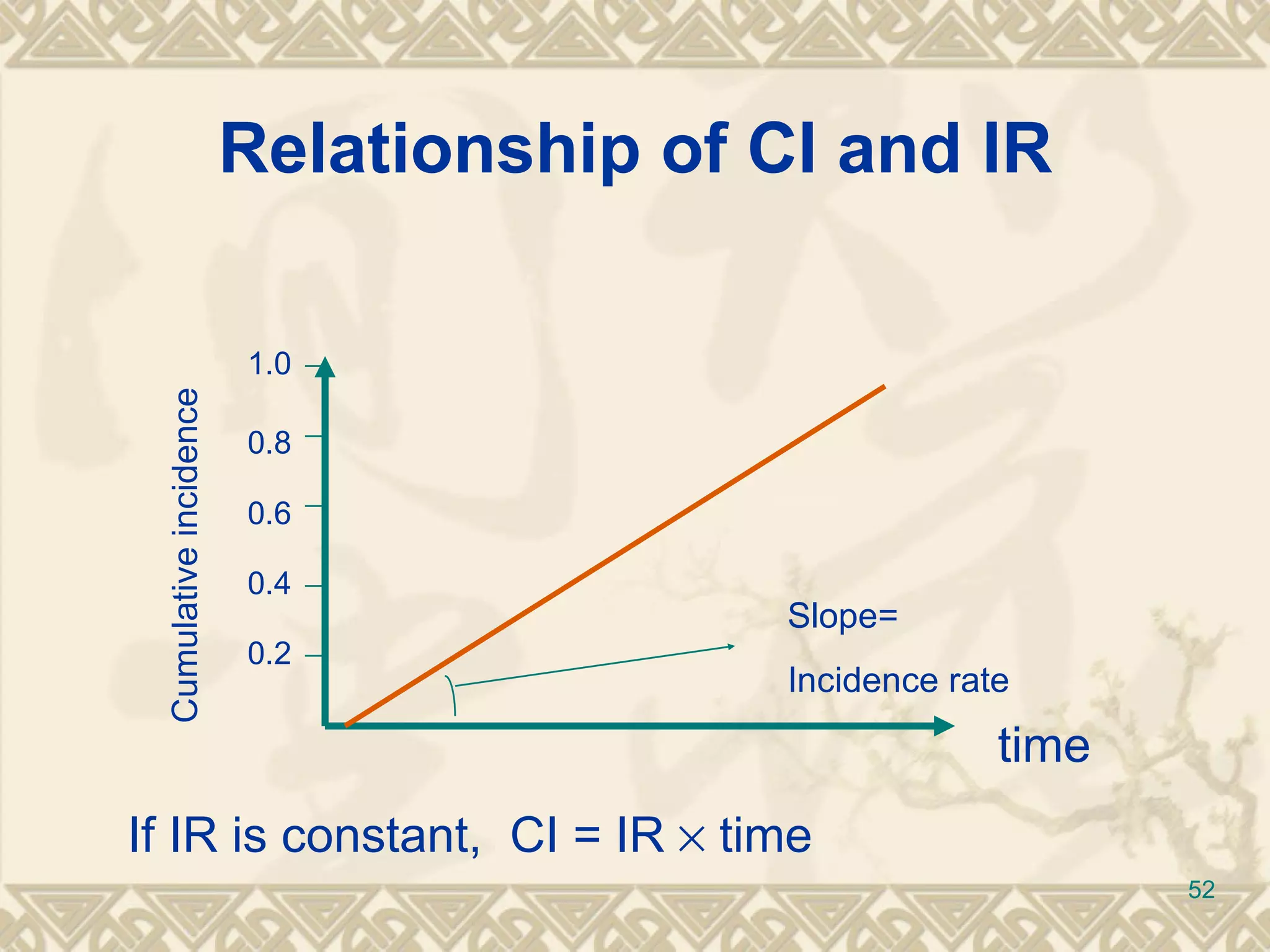
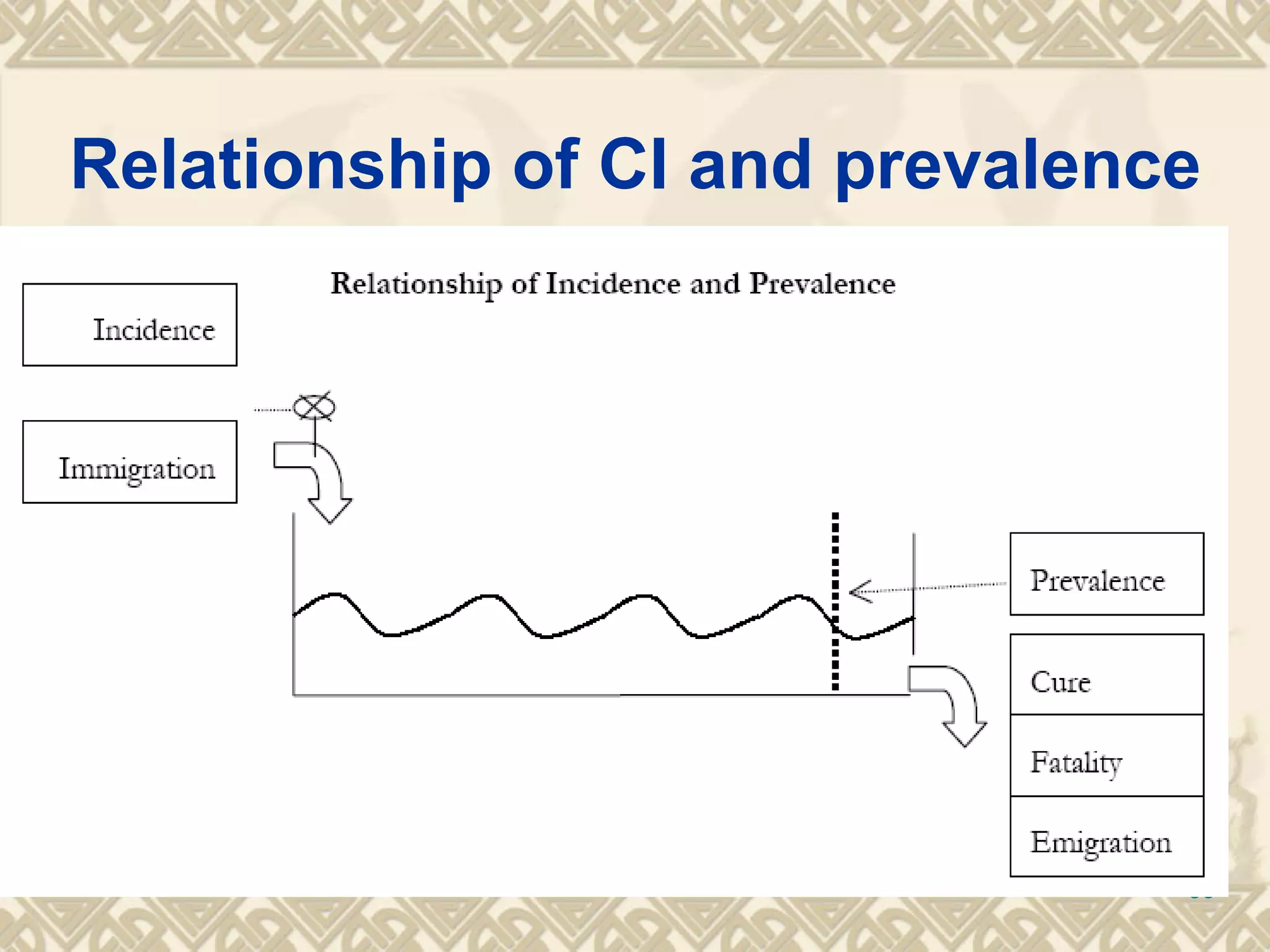
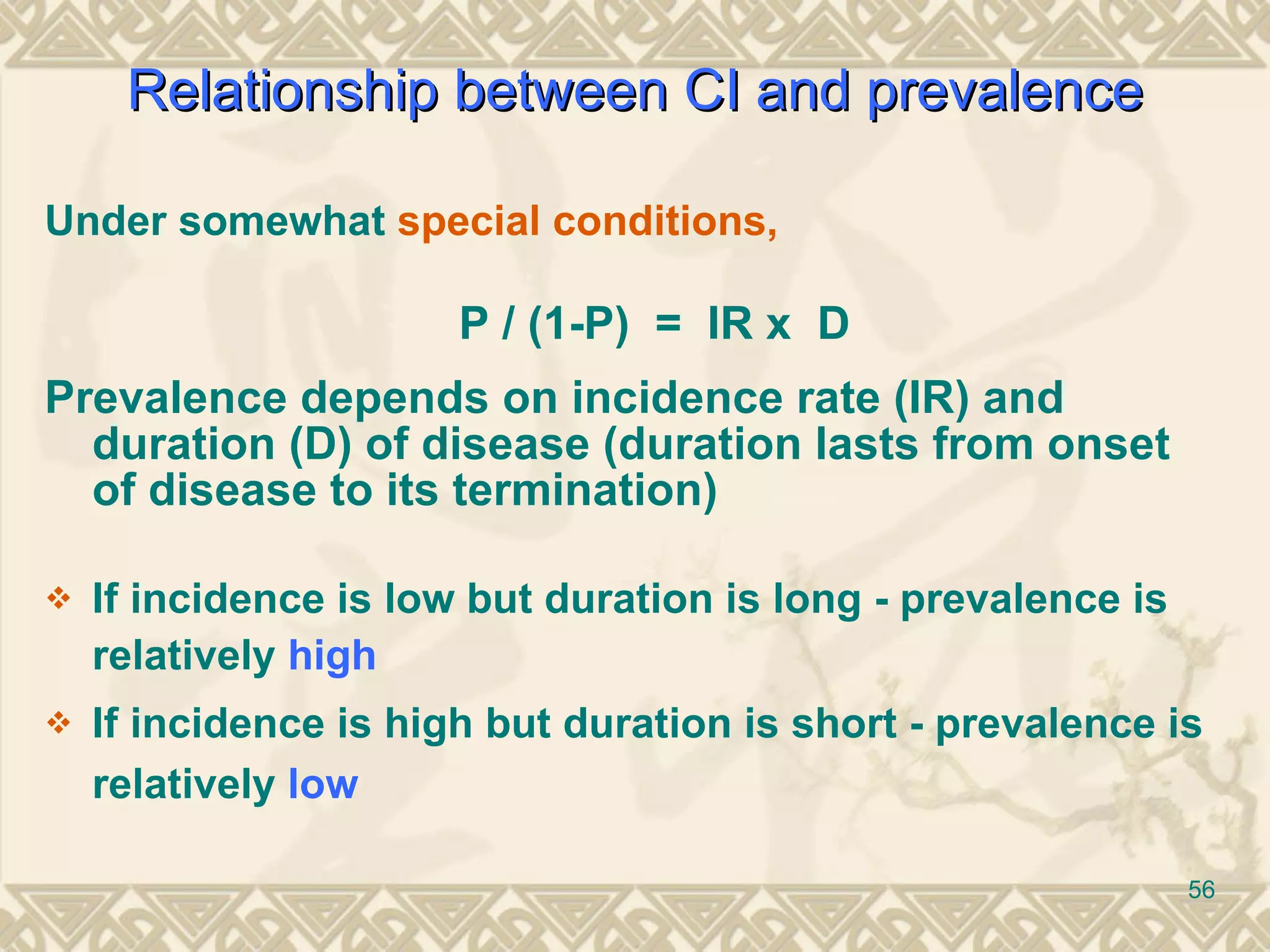
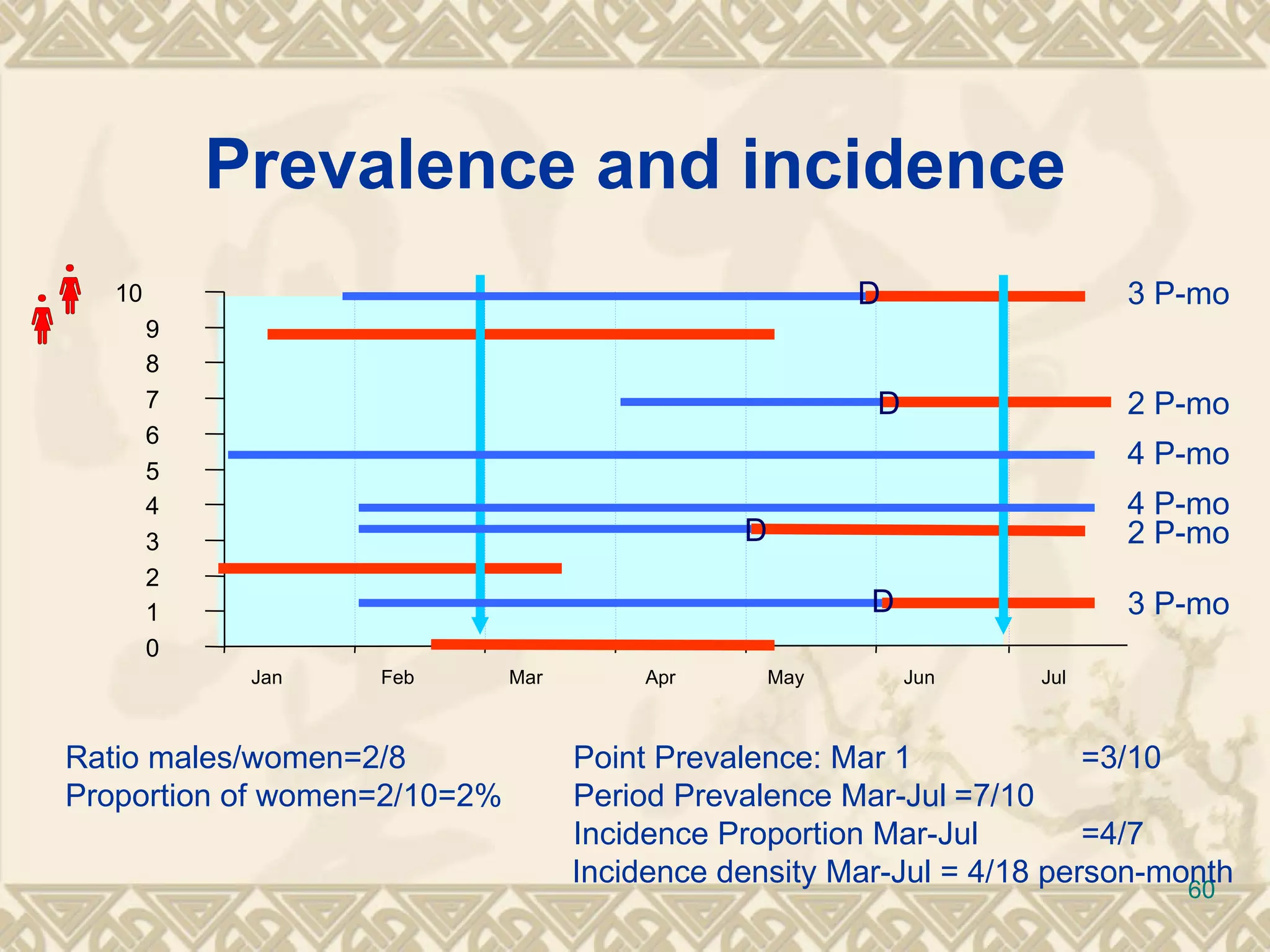
Calculating population at risk, the incidence rate, cumulative incidence, and attack rates, with examples.Comparative analysis of cumulative incidence and prevalence, factors affecting their relationship.
Practical uses of incidence and prevalence measures in public health for planning and evaluating.
Discussion on why incidence is preferred over prevalence in studying disease etiology.
Summarization of key points regarding prevalence and incidence definitions and their applications.
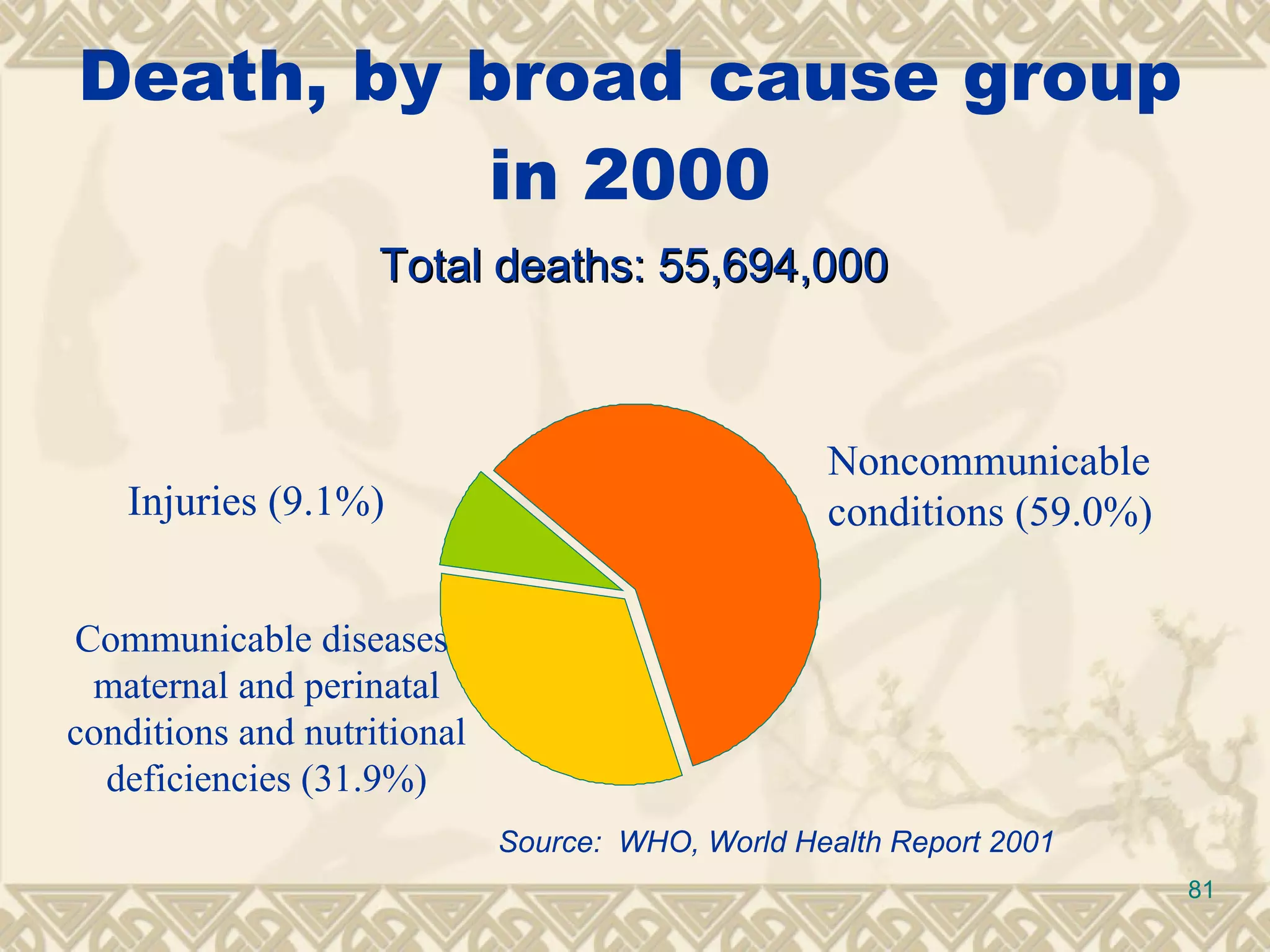
Introduction to measuring mortality rates as part of epidemiological measures.
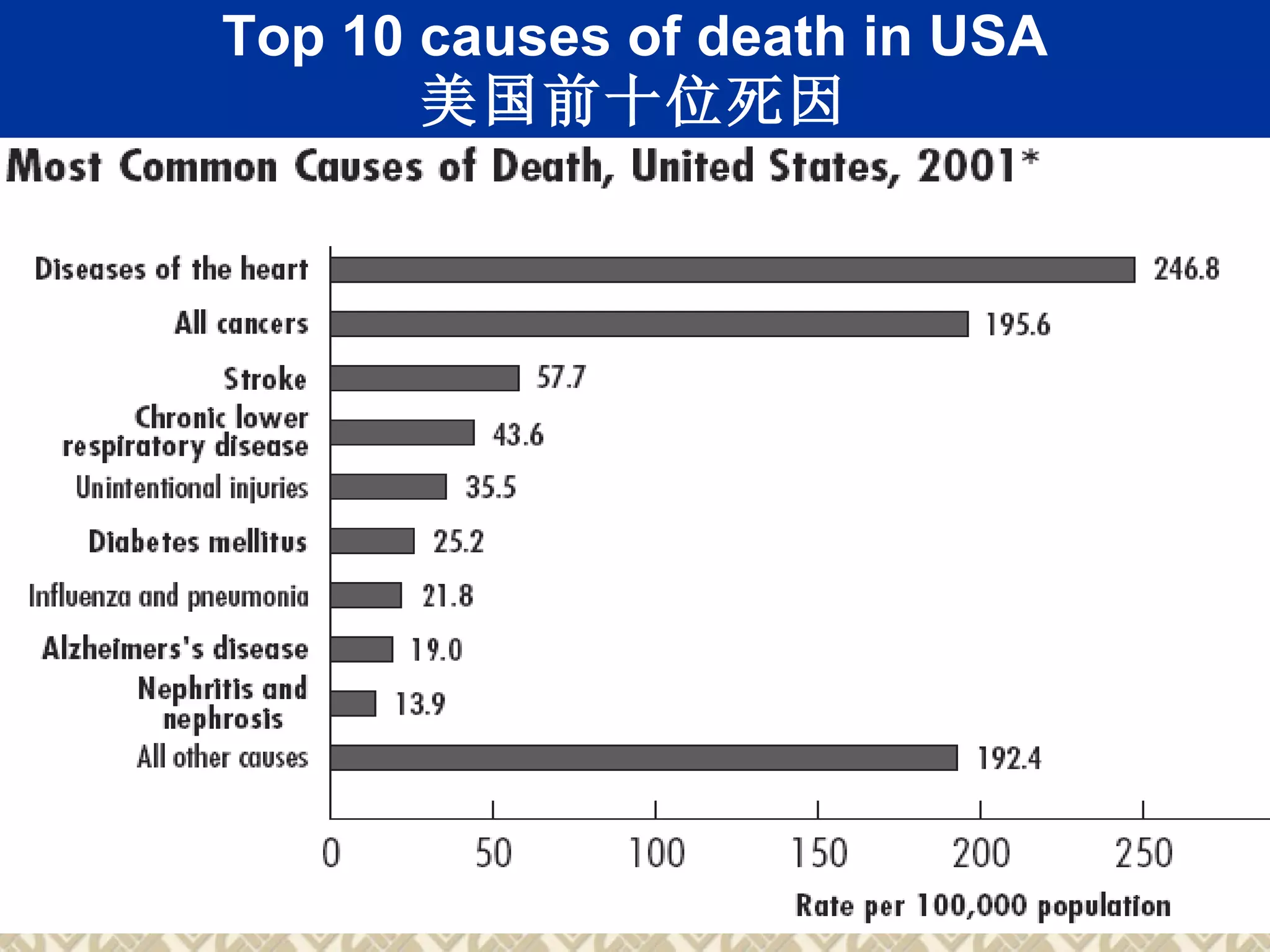
Different types of mortality rates including specific mortality, case-fatality rates, and comparisons.
Citations for further reading and conclusion of the presentation, thanking the participants.











































































































