Downloaded 1,682 times
![Spinal,epidural and caudal anesthesia [email_address]](https://image.slidesharecdn.com/5regionalanesthesia-100526045613-phpapp02/75/5-regional-anesthesia-1-2048.jpg)



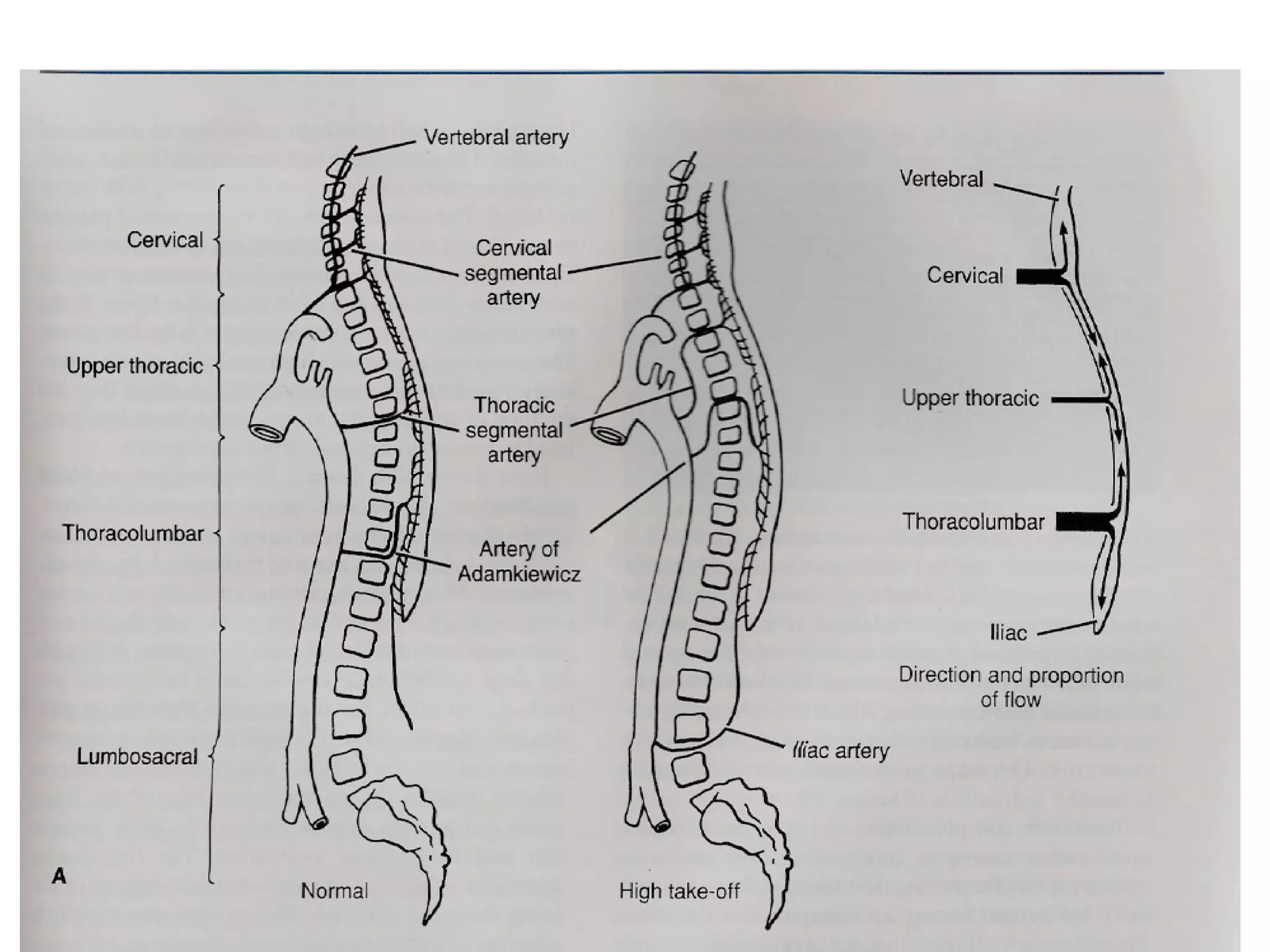














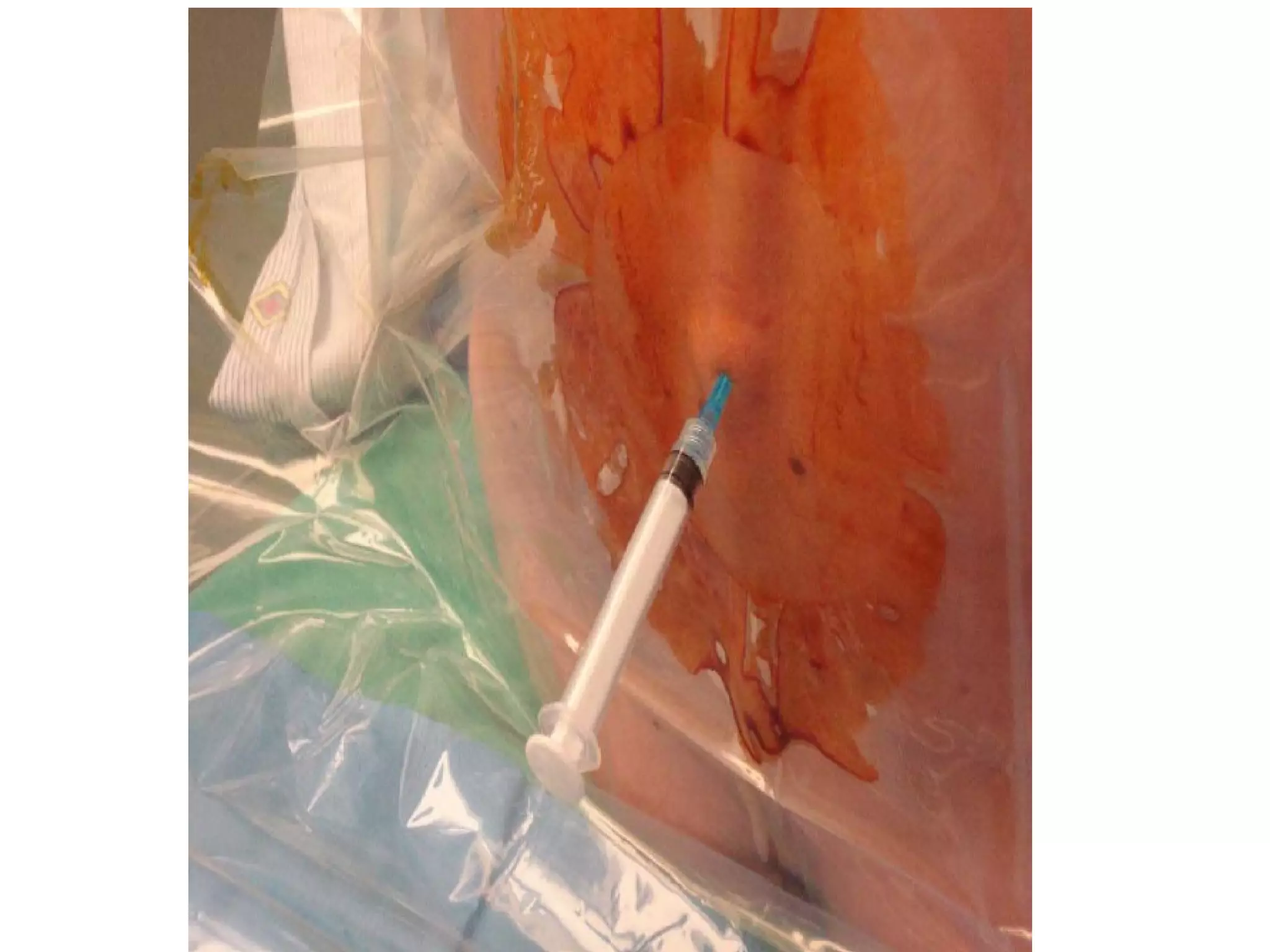
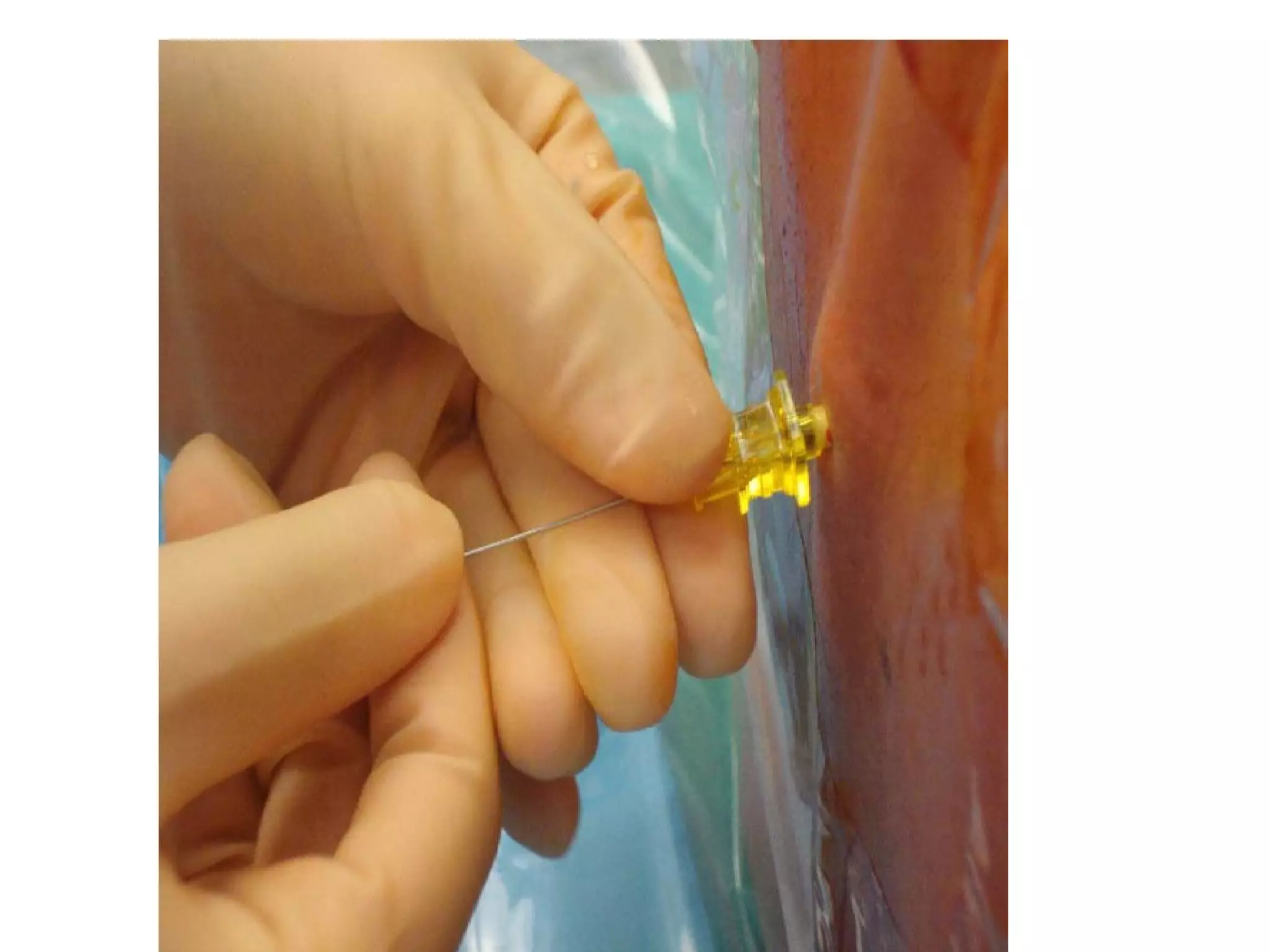

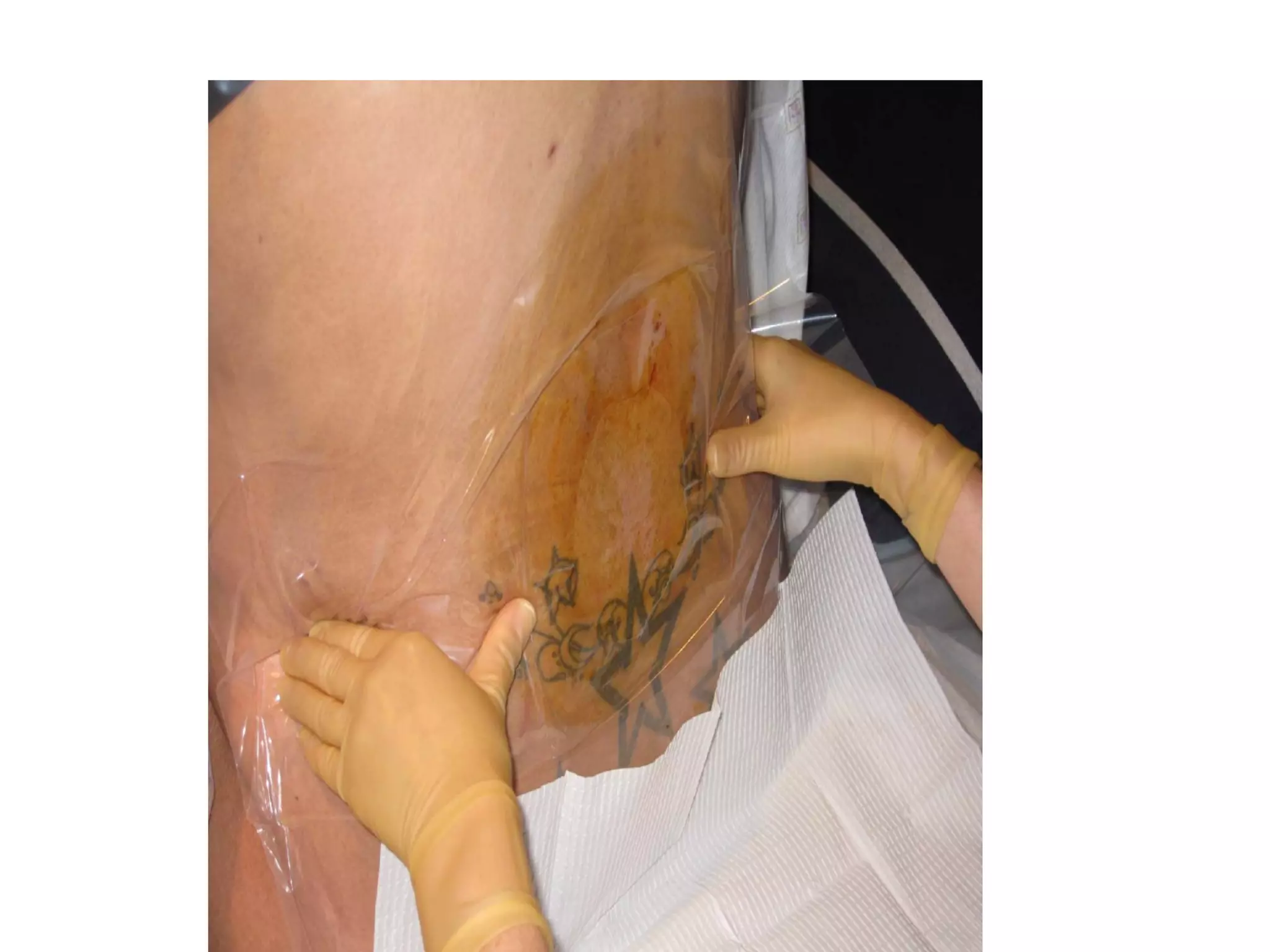



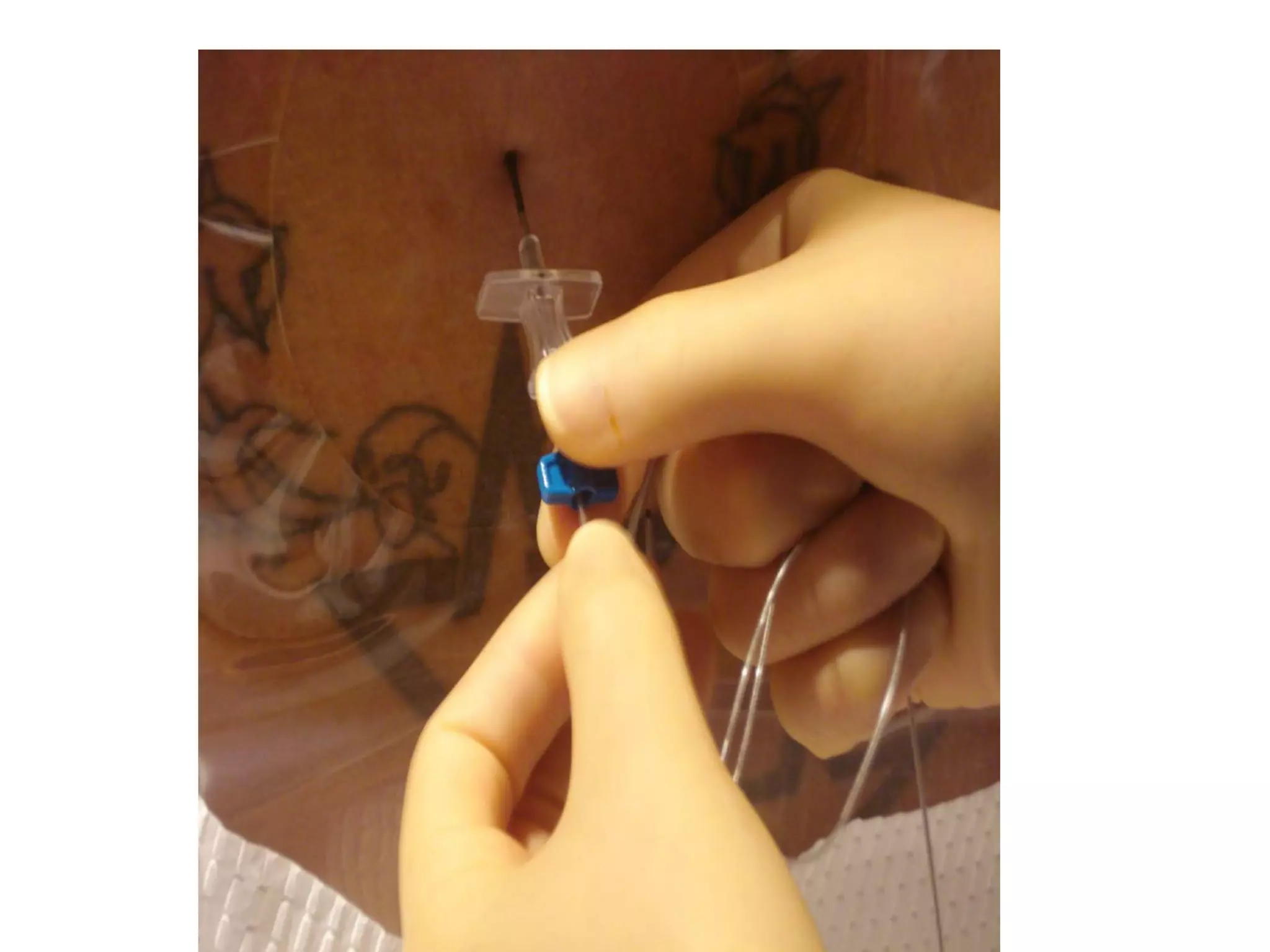

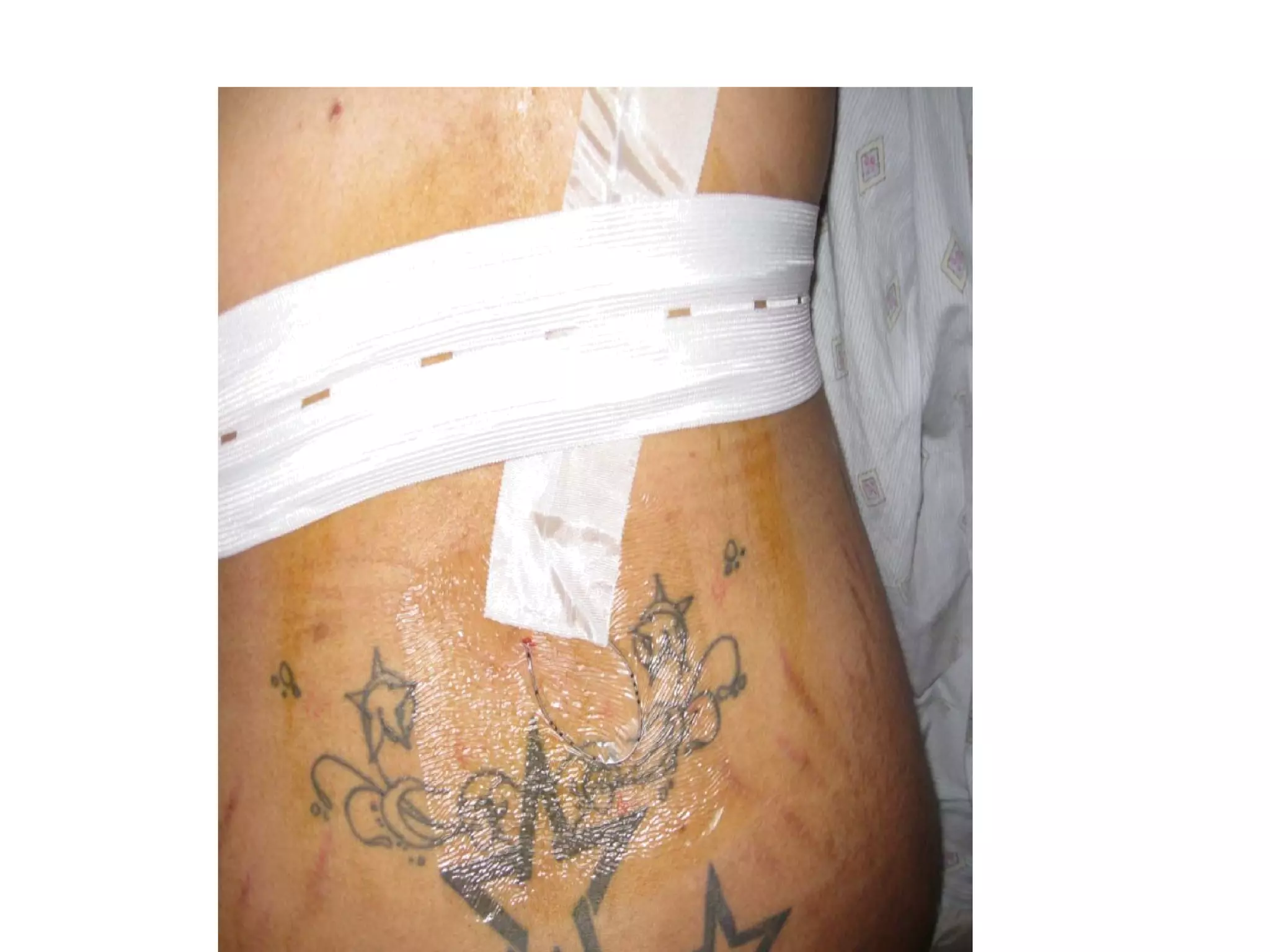












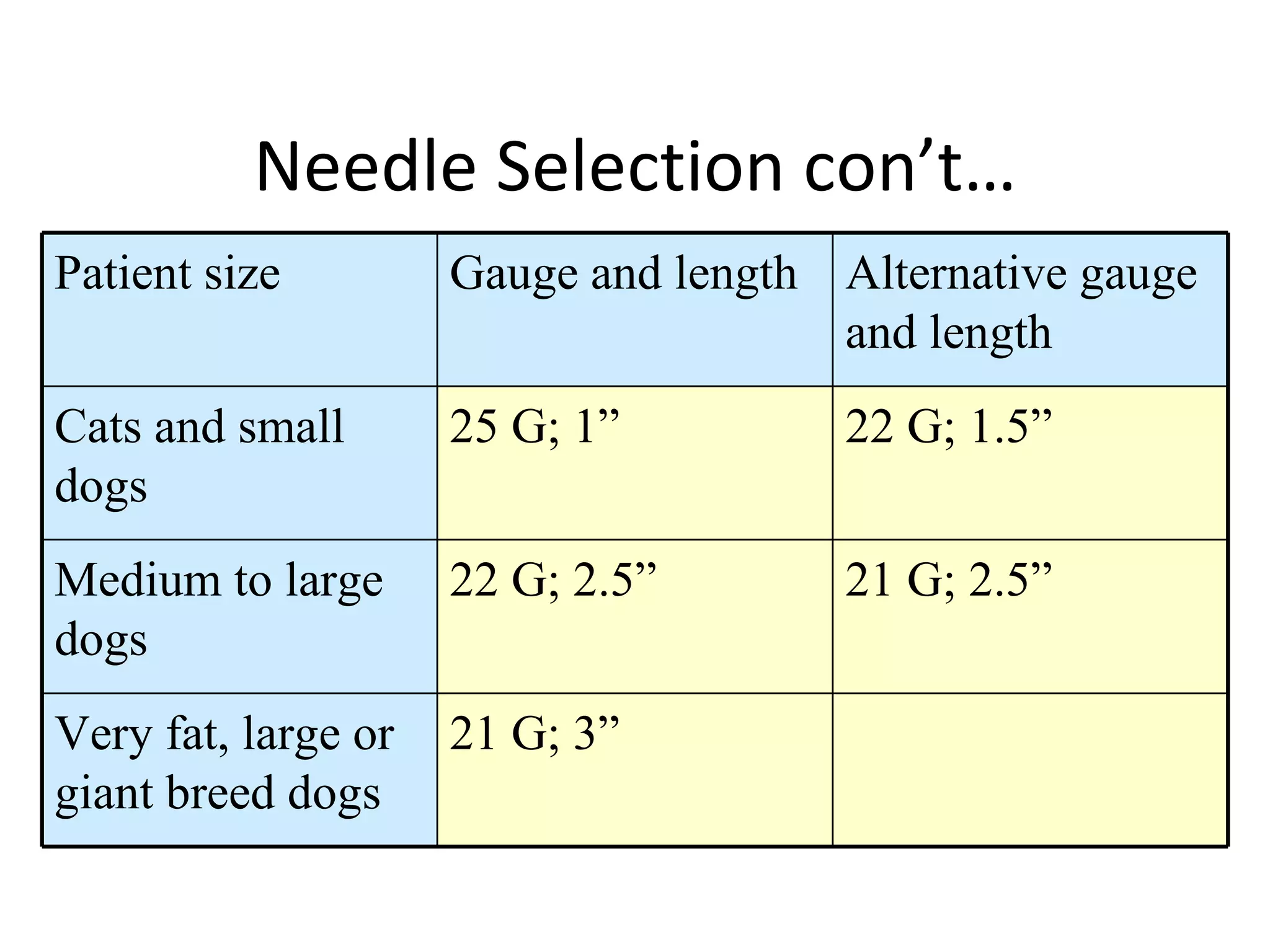





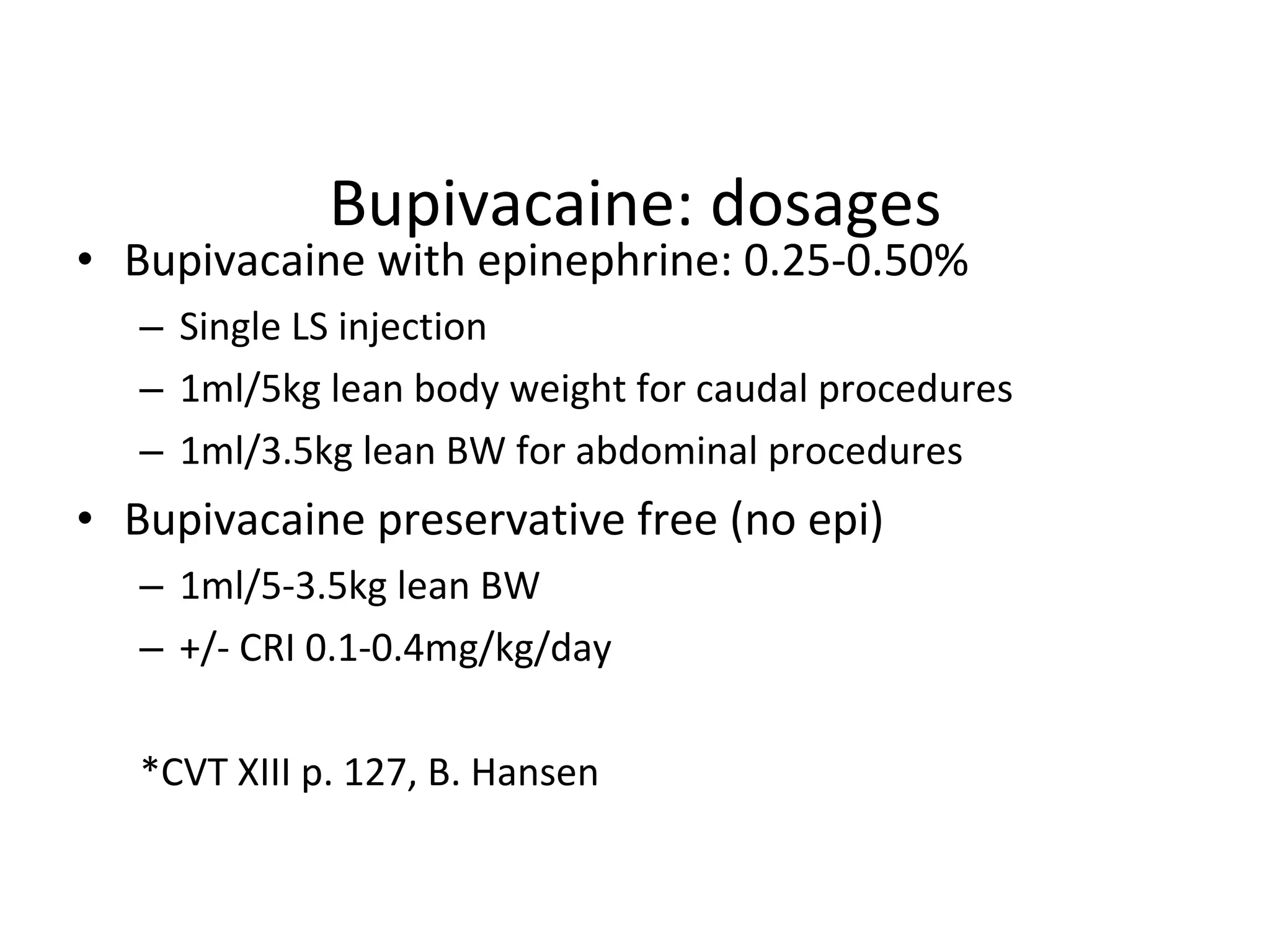








The document discusses the history and current use of spinal, epidural, and caudal anesthesia. It provides details on: 1) The key developments in these techniques from 1885 to present day and their current role in veterinary and human anesthesia. 2) The indications, contraindications, and complications of these regional anesthesia techniques. 3) The local anesthetics, opioids, and other agents used and their mechanisms of action, dosages, durations, and side effects. 4) Techniques for administering spinal, epidural, and caudal anesthesia including needle selection, injection procedures, and postoperative care.































































































