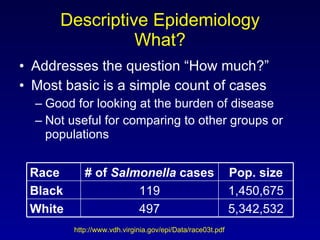
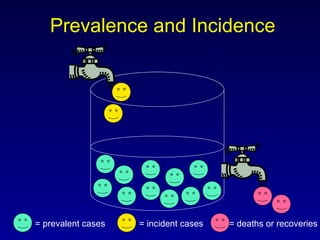
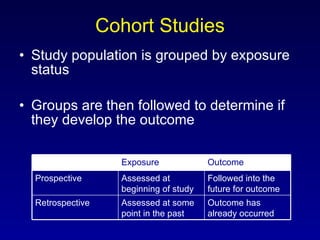
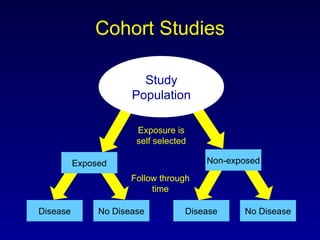
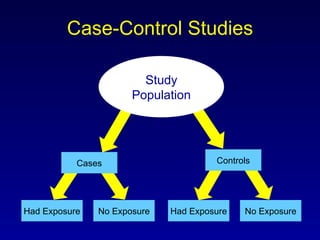
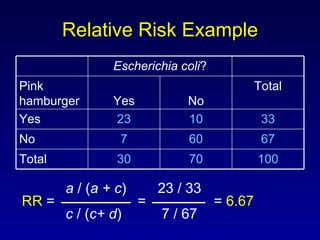
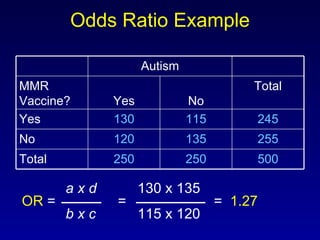
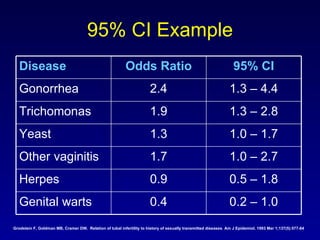
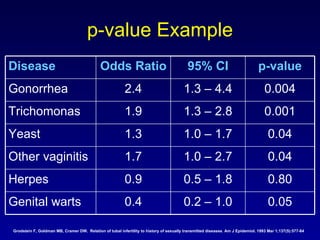
This document provides an overview of a training session on descriptive and analytic epidemiology. Descriptive epidemiology involves describing disease frequency, distribution, and determinants in populations using measures like prevalence and incidence. Analytic epidemiology aims to understand why diseases occur using study designs like cohort studies and case-control studies to test hypotheses. Key terms discussed include measures of association like relative risk and odds ratio, and statistical tests like confidence intervals and p-values.


























































![Surgery cholangitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/surgery-cholangitis1-120601032247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





























