Downloaded 1,517 times
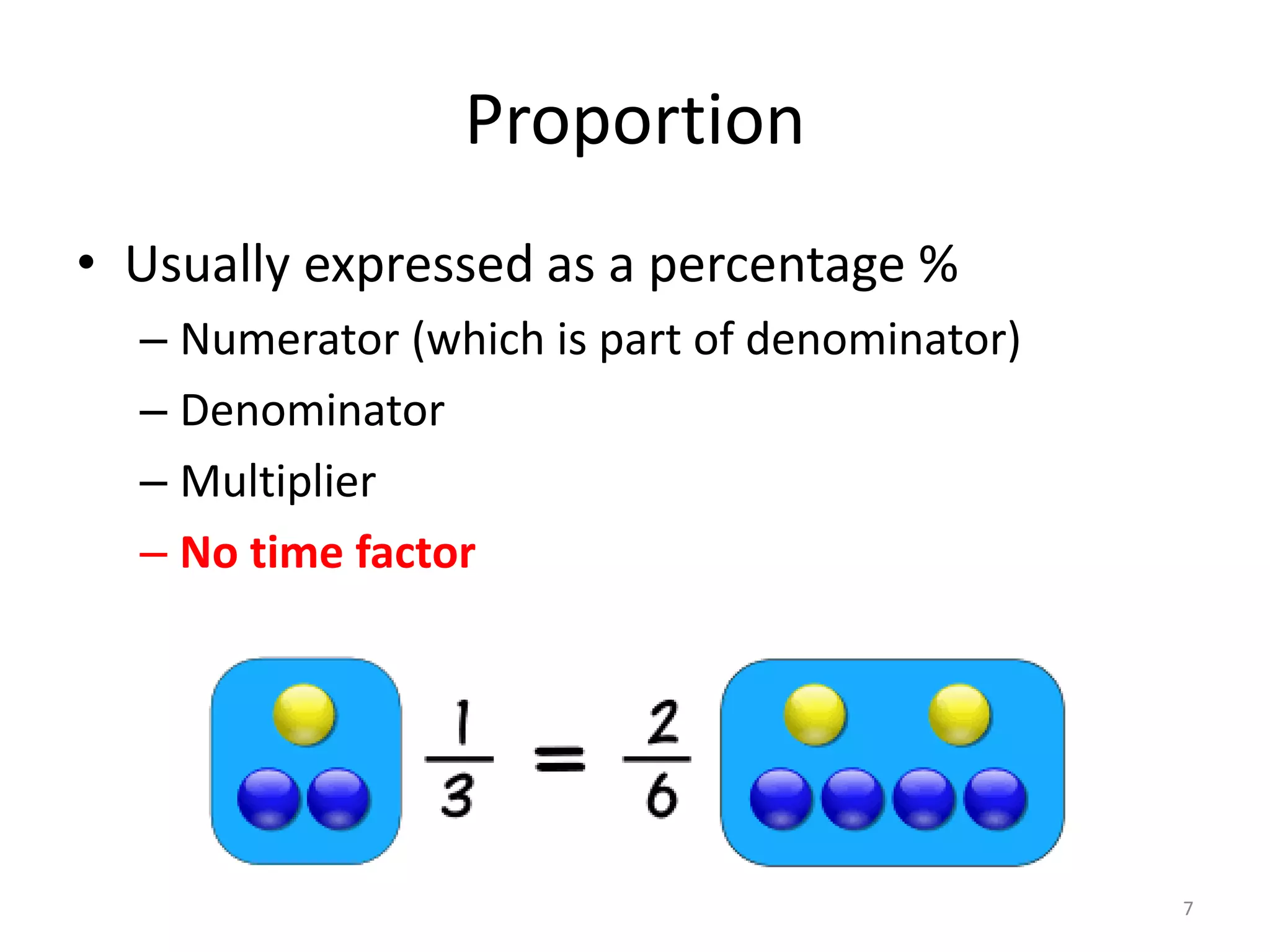
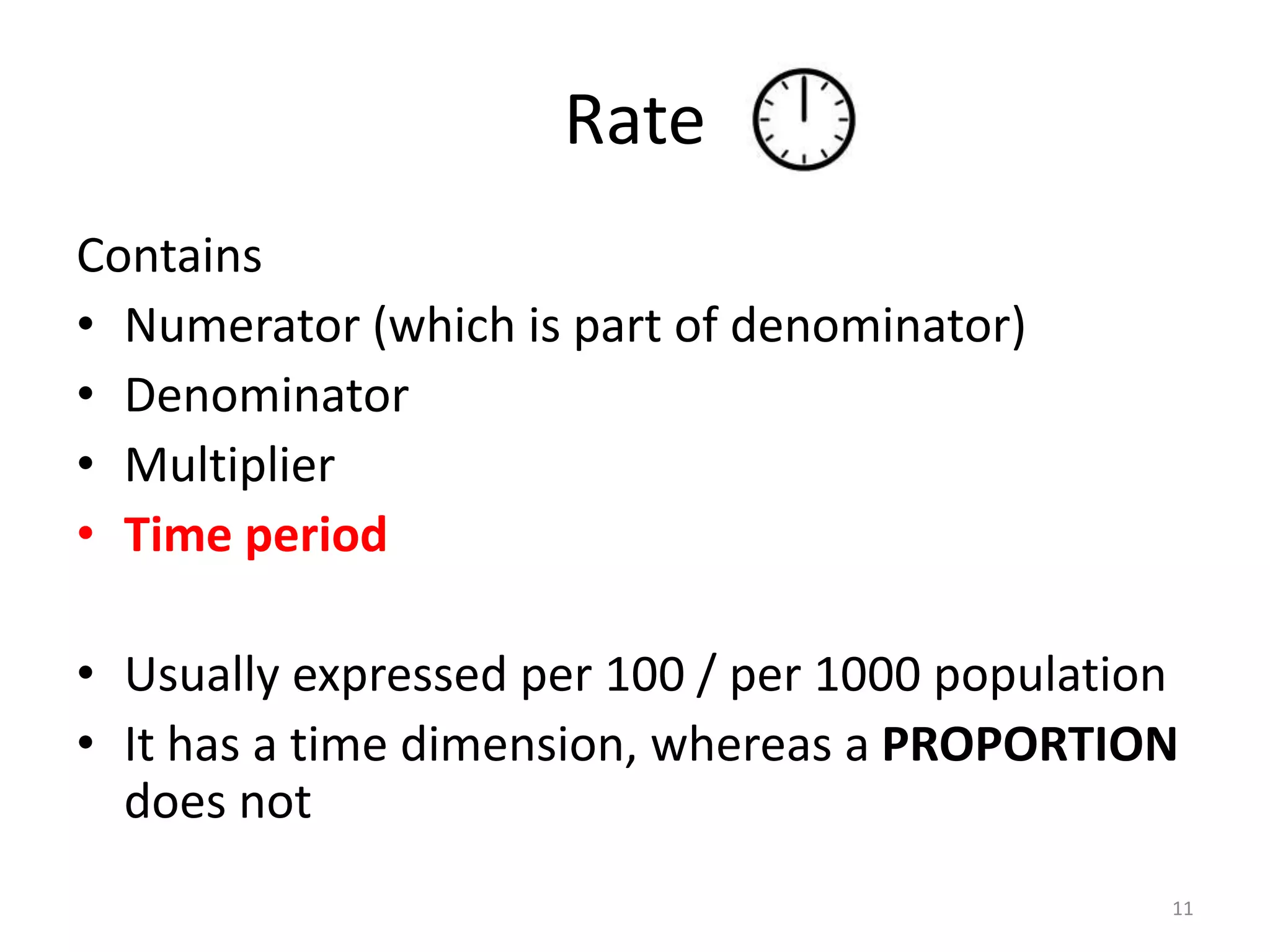

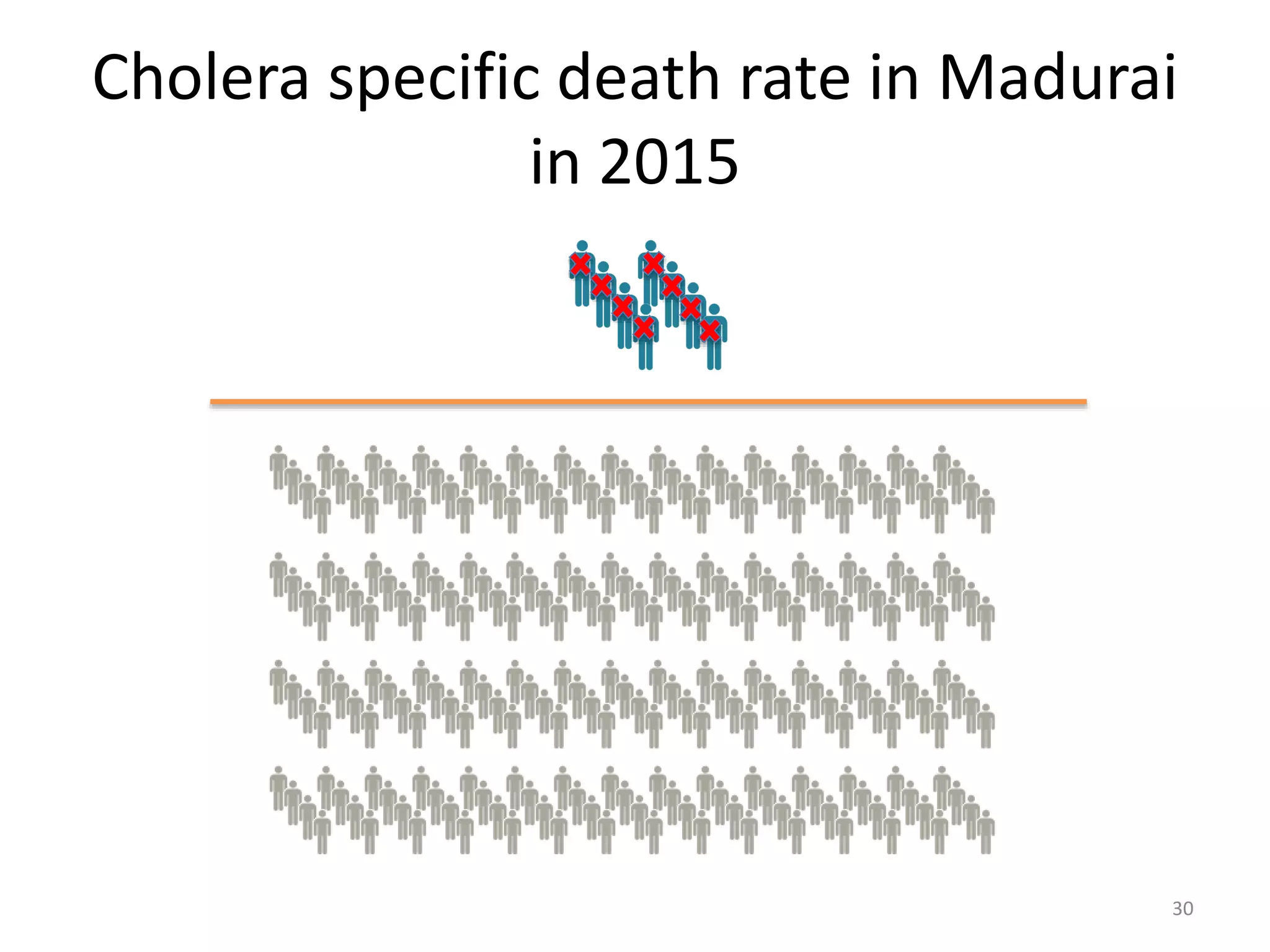
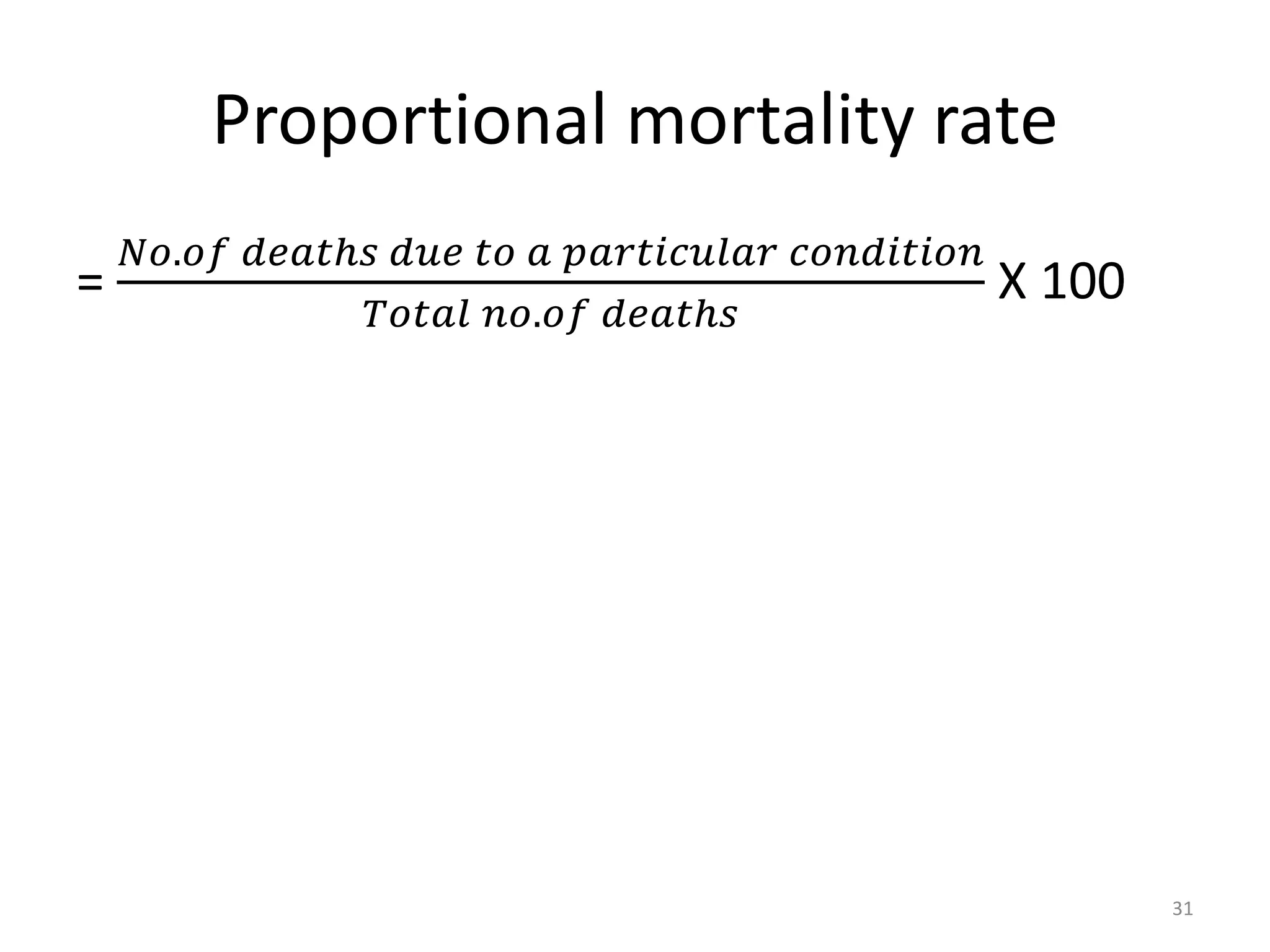
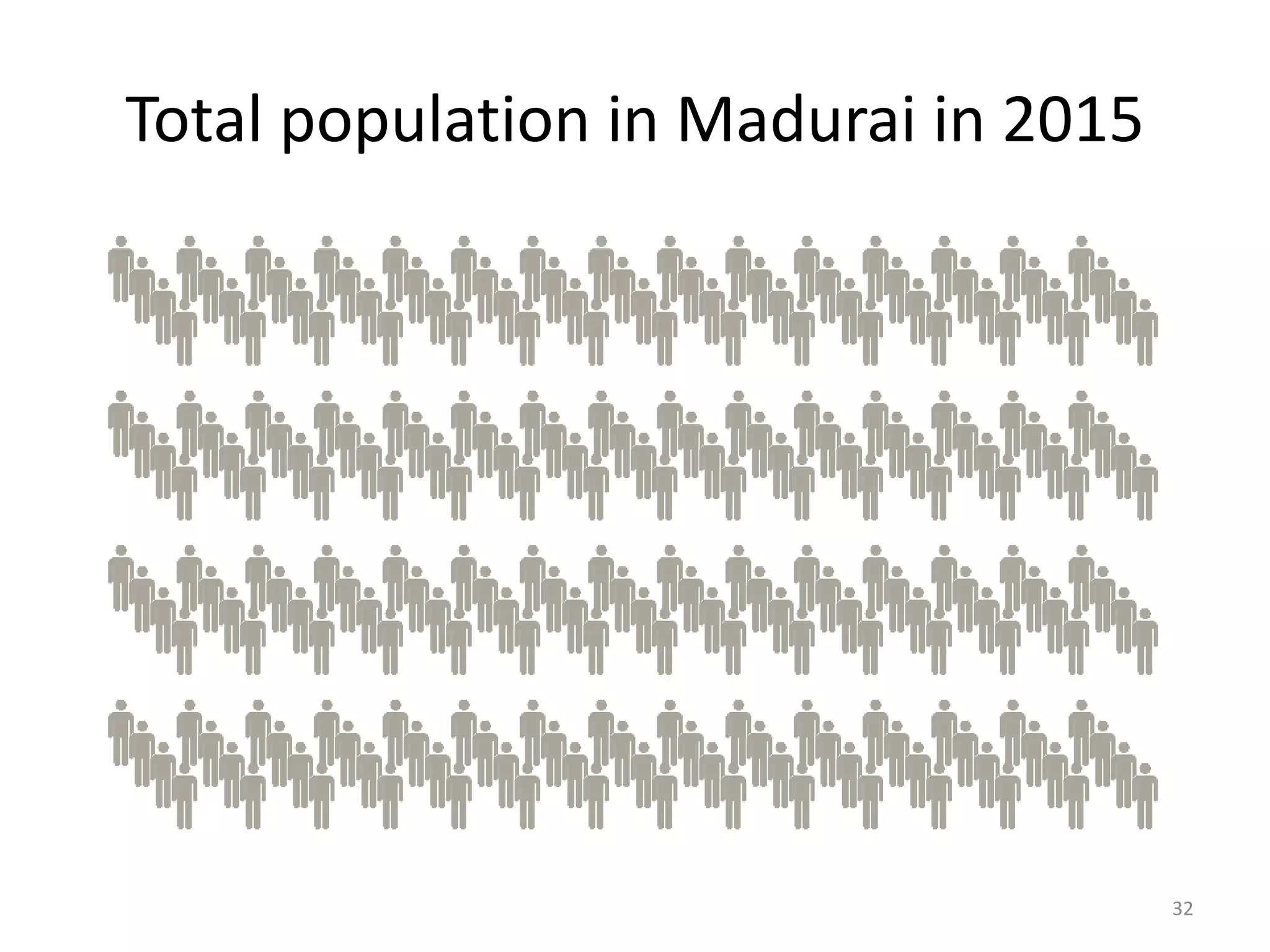
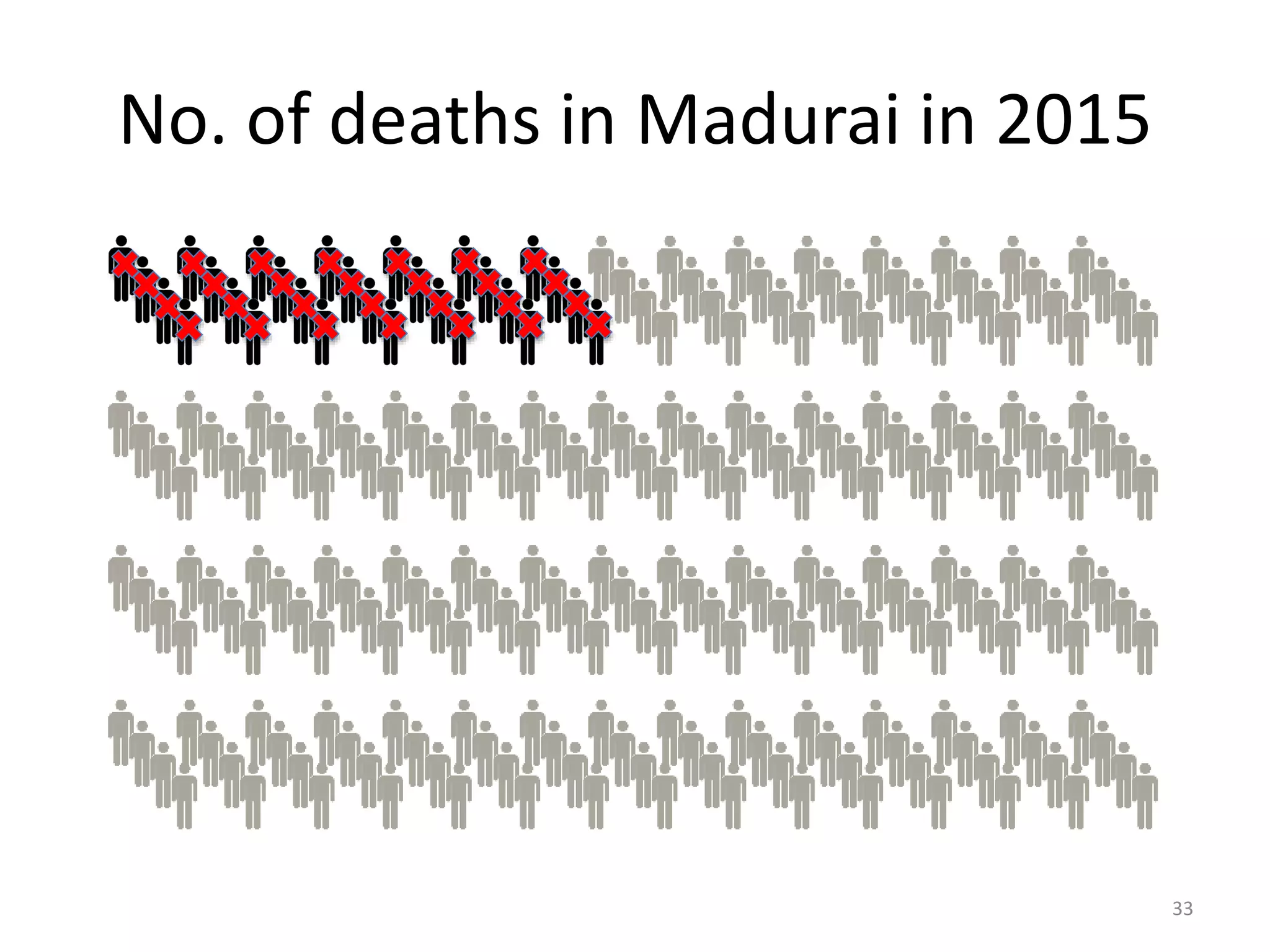

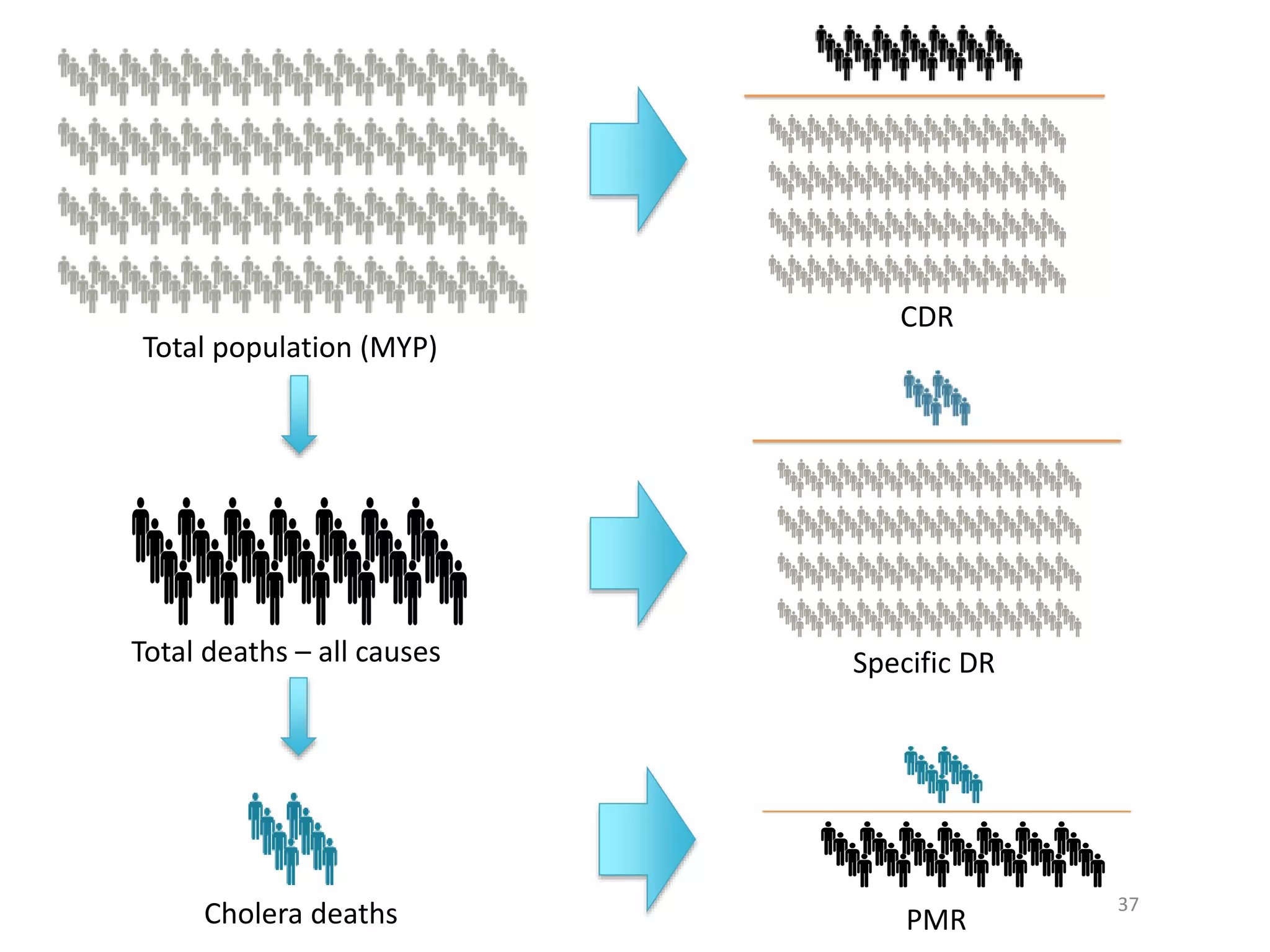
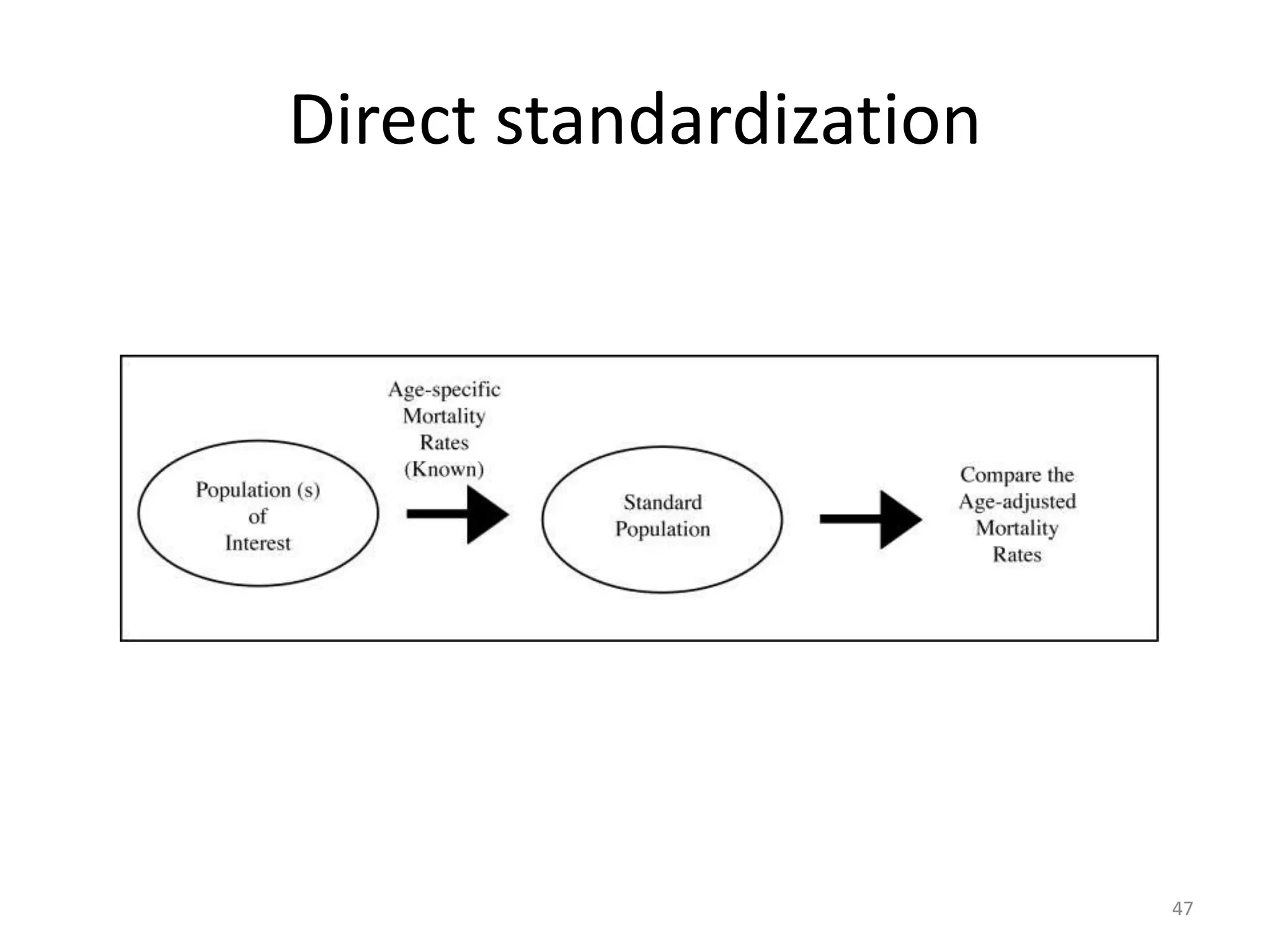
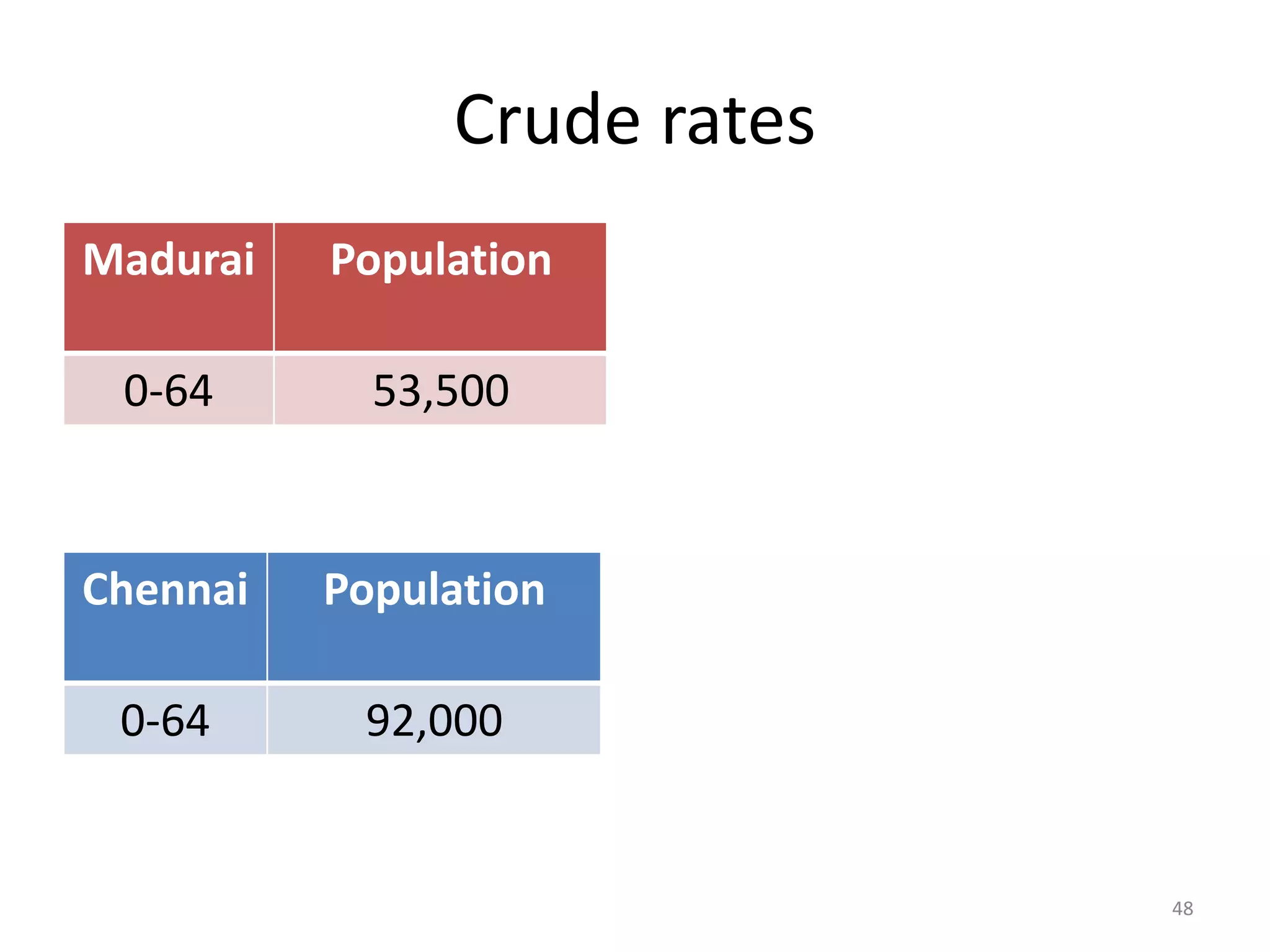
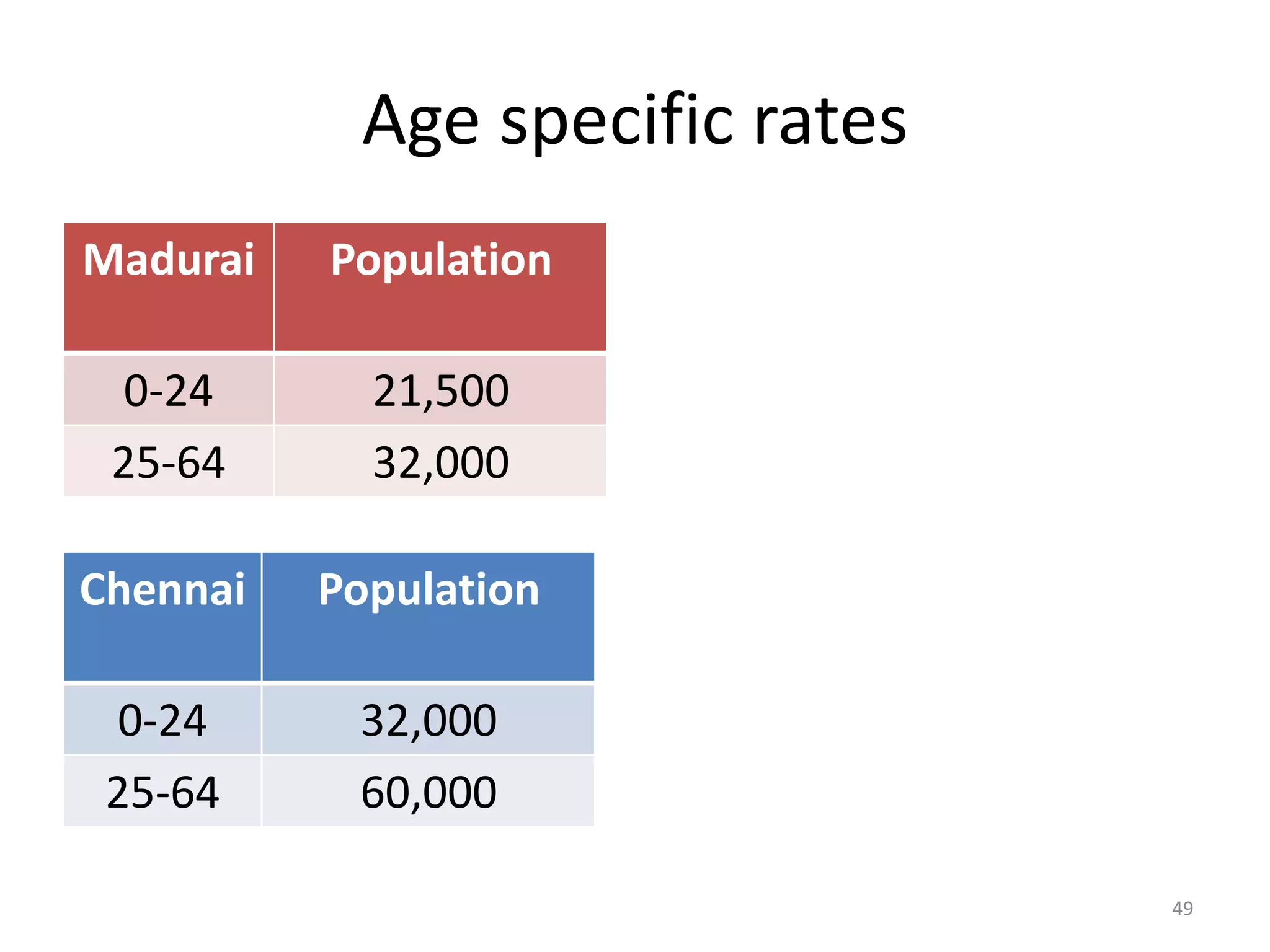
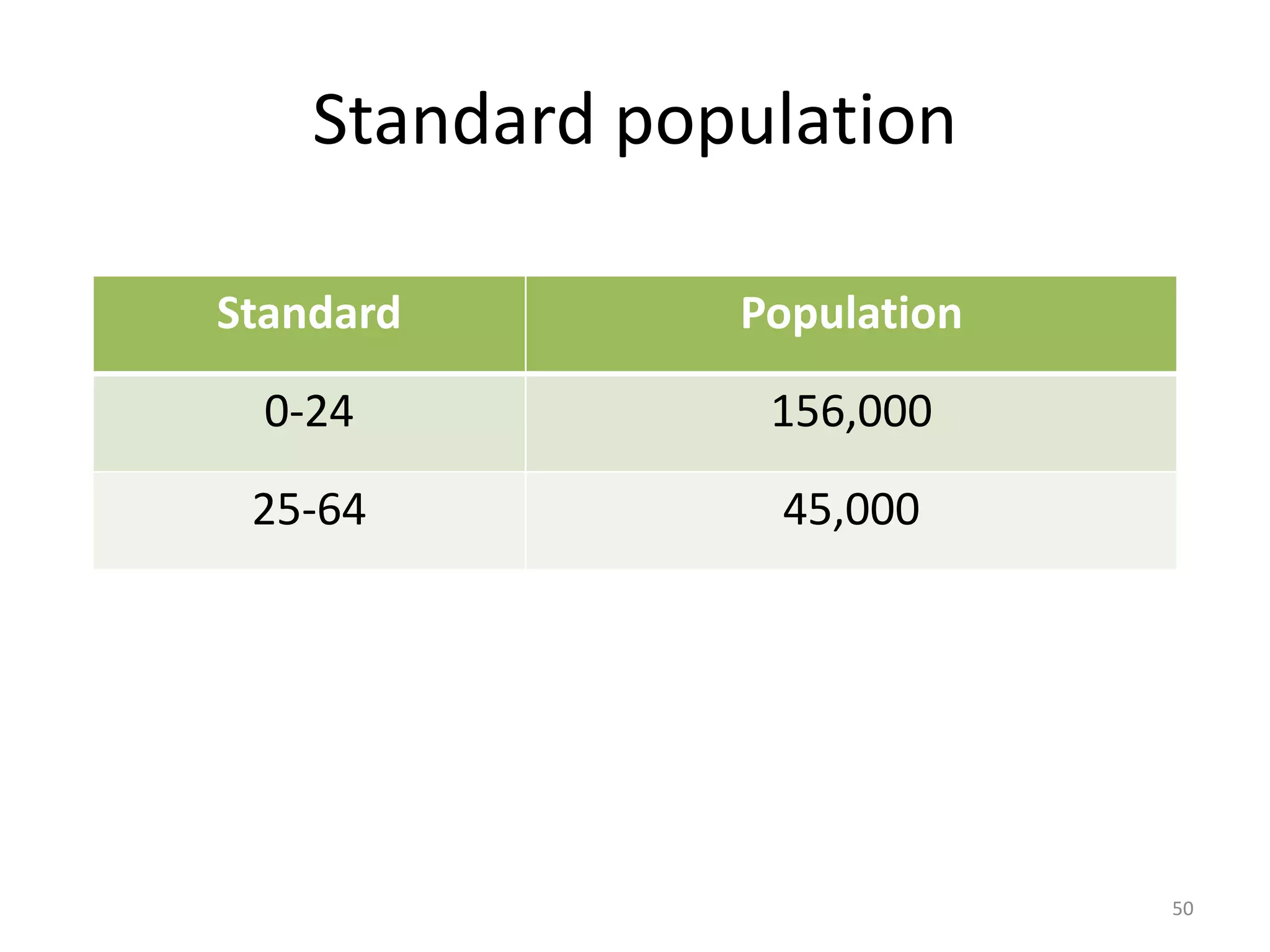
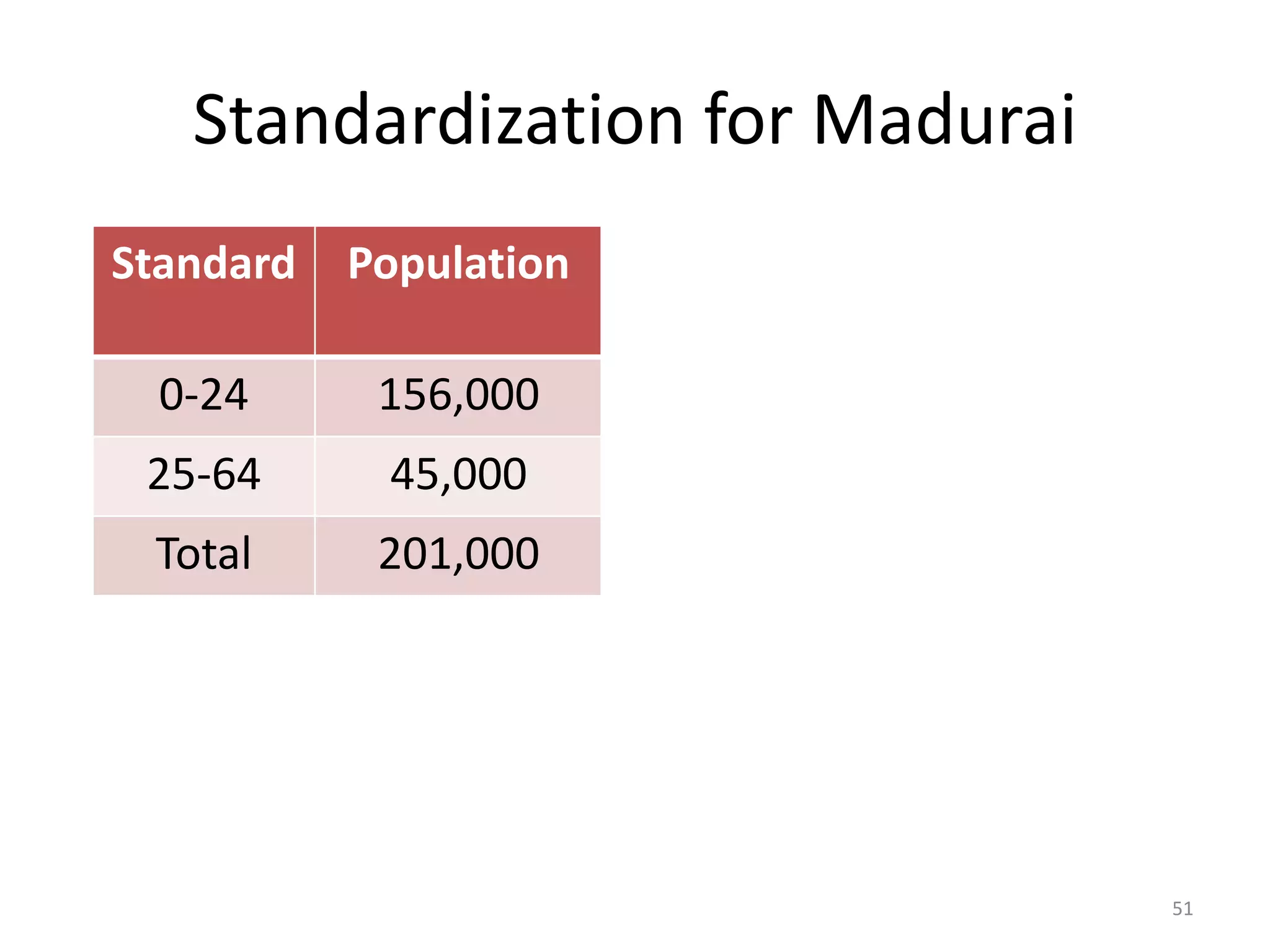
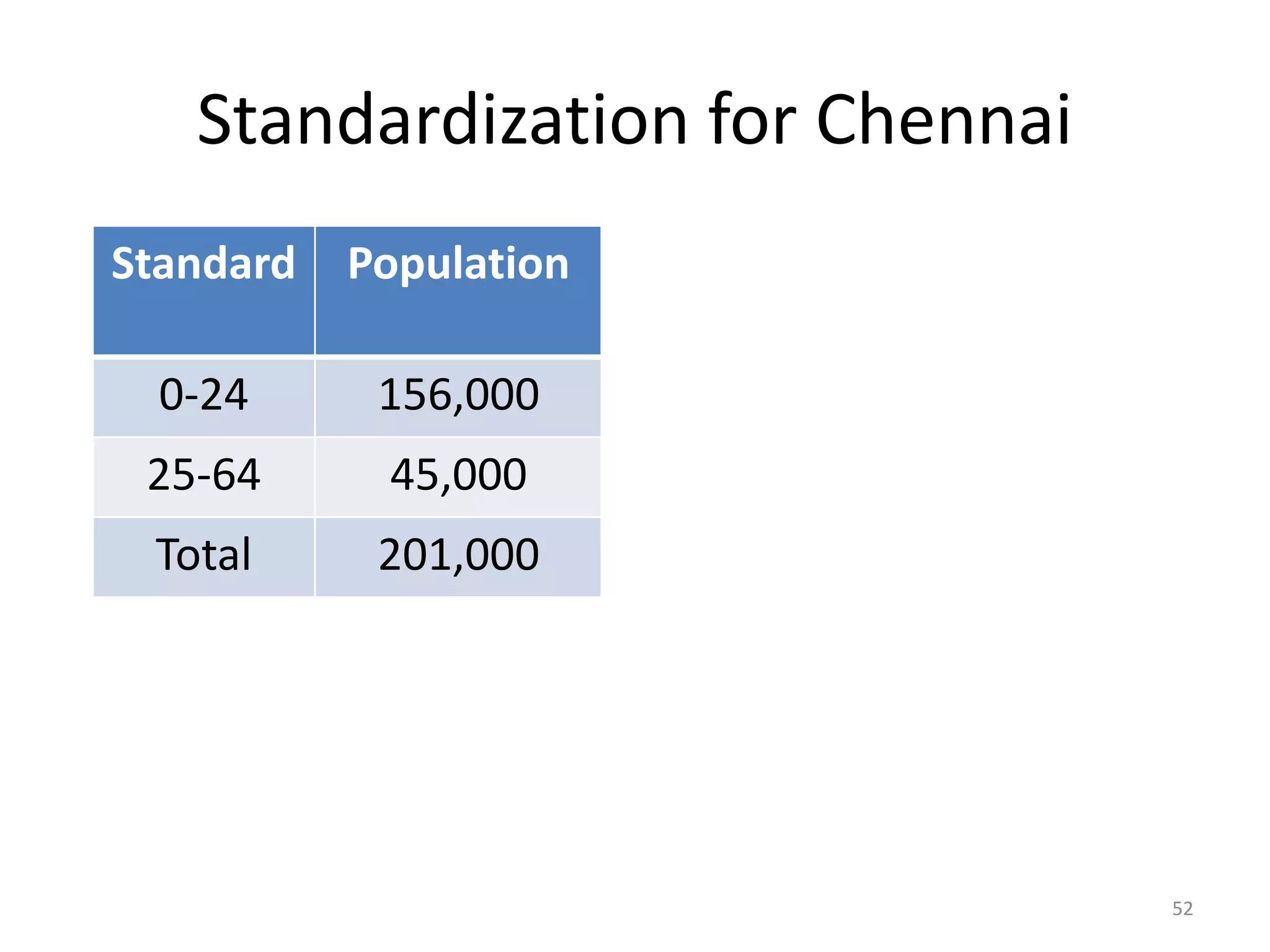
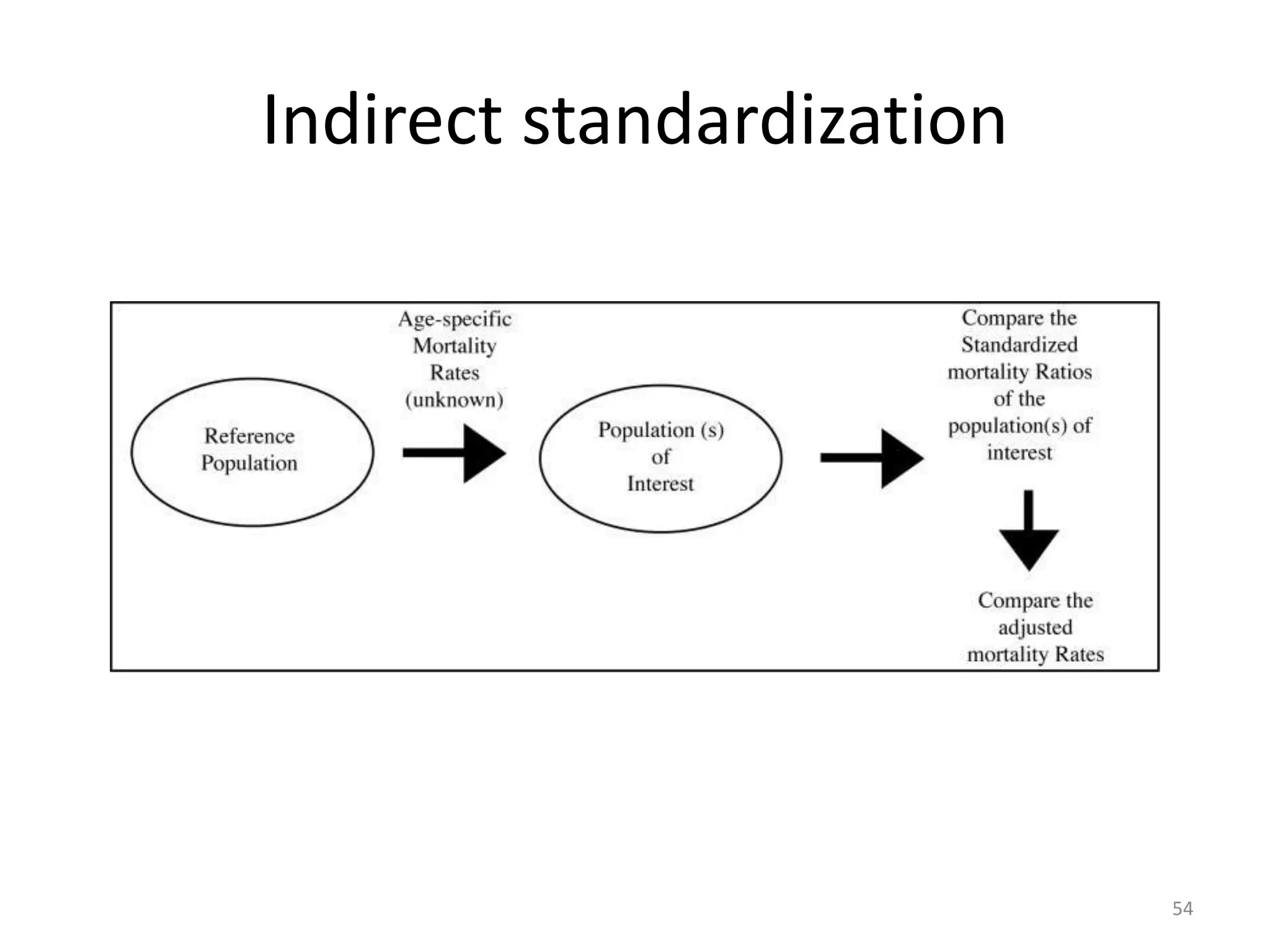
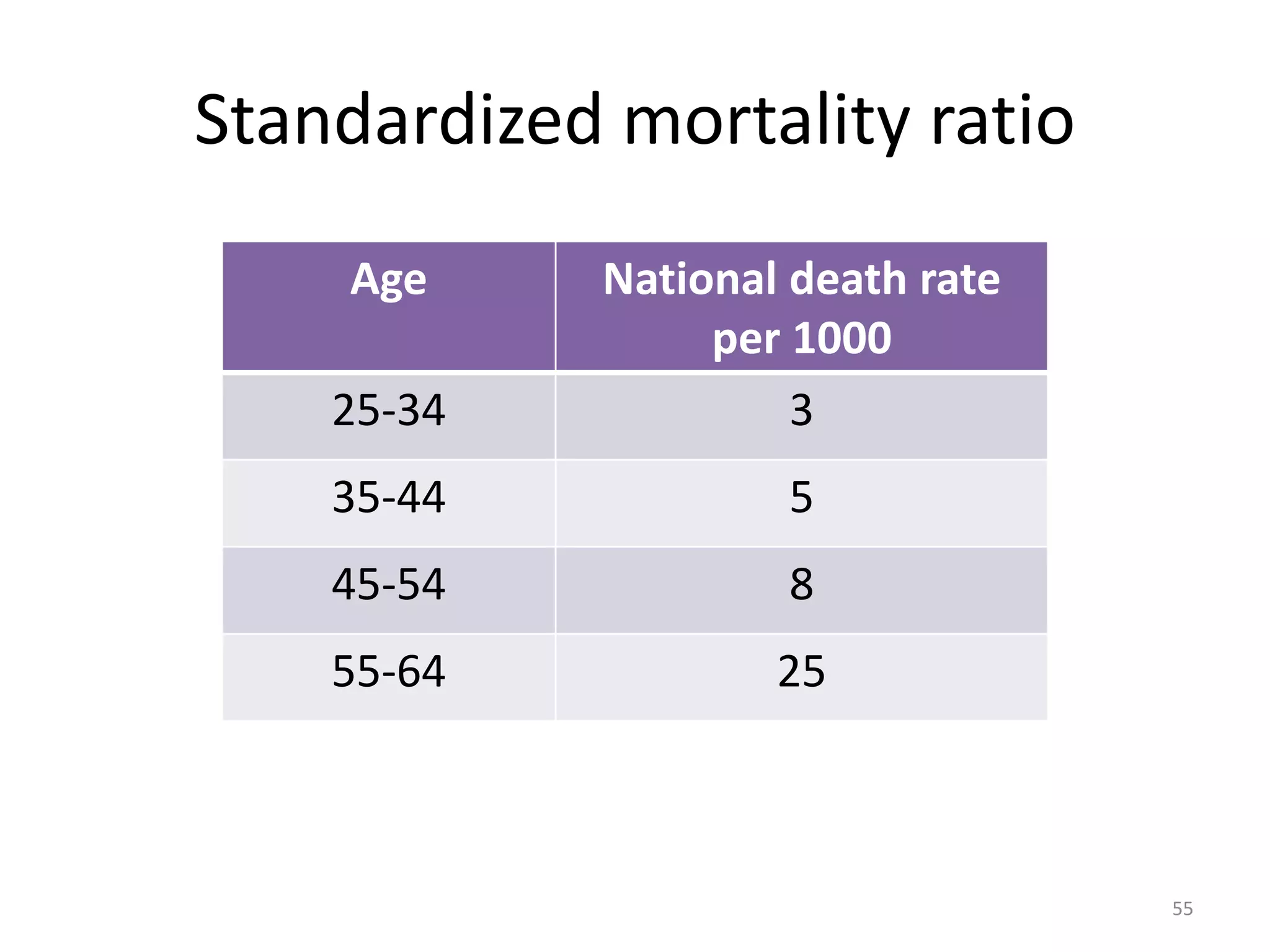
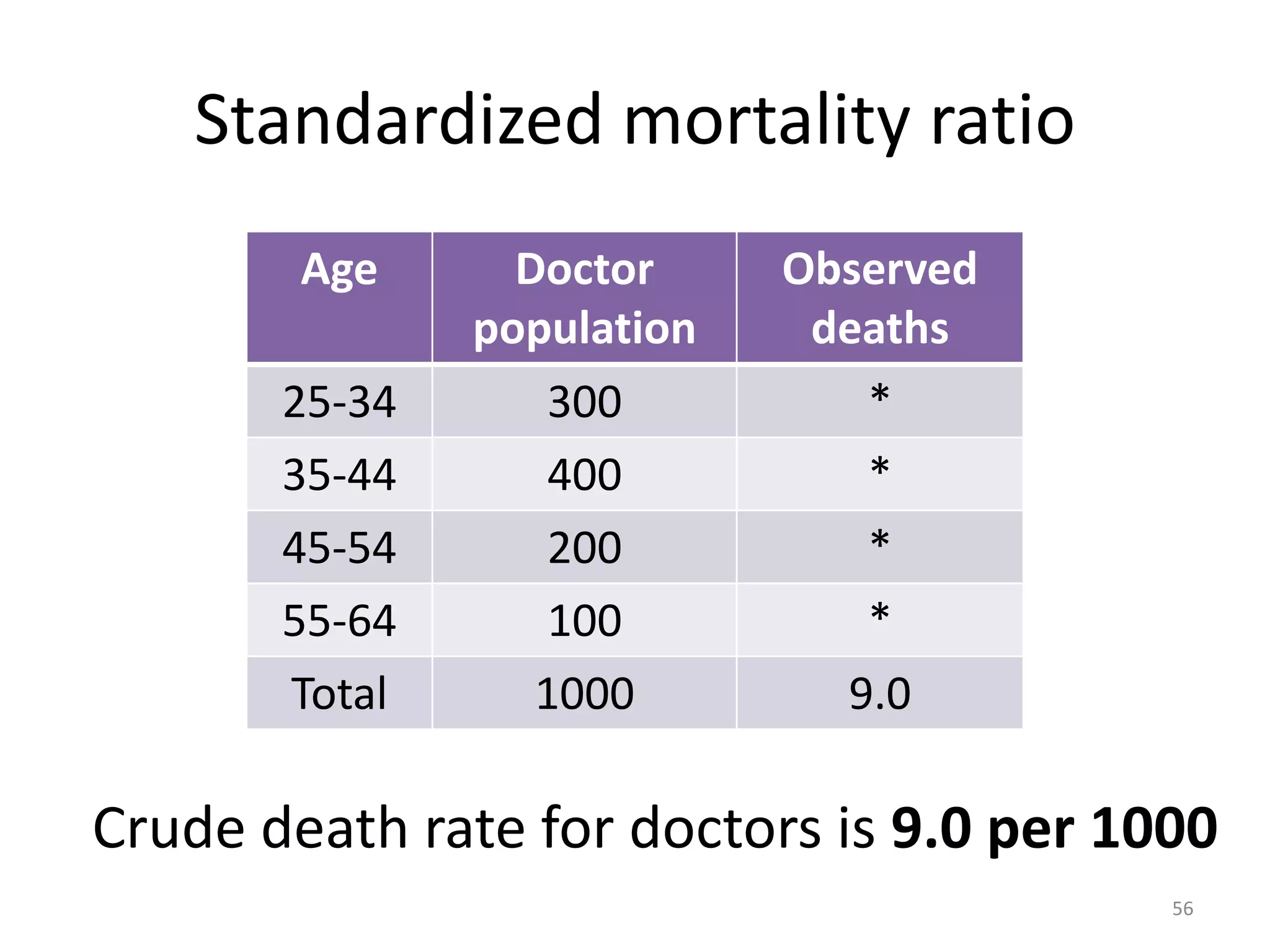
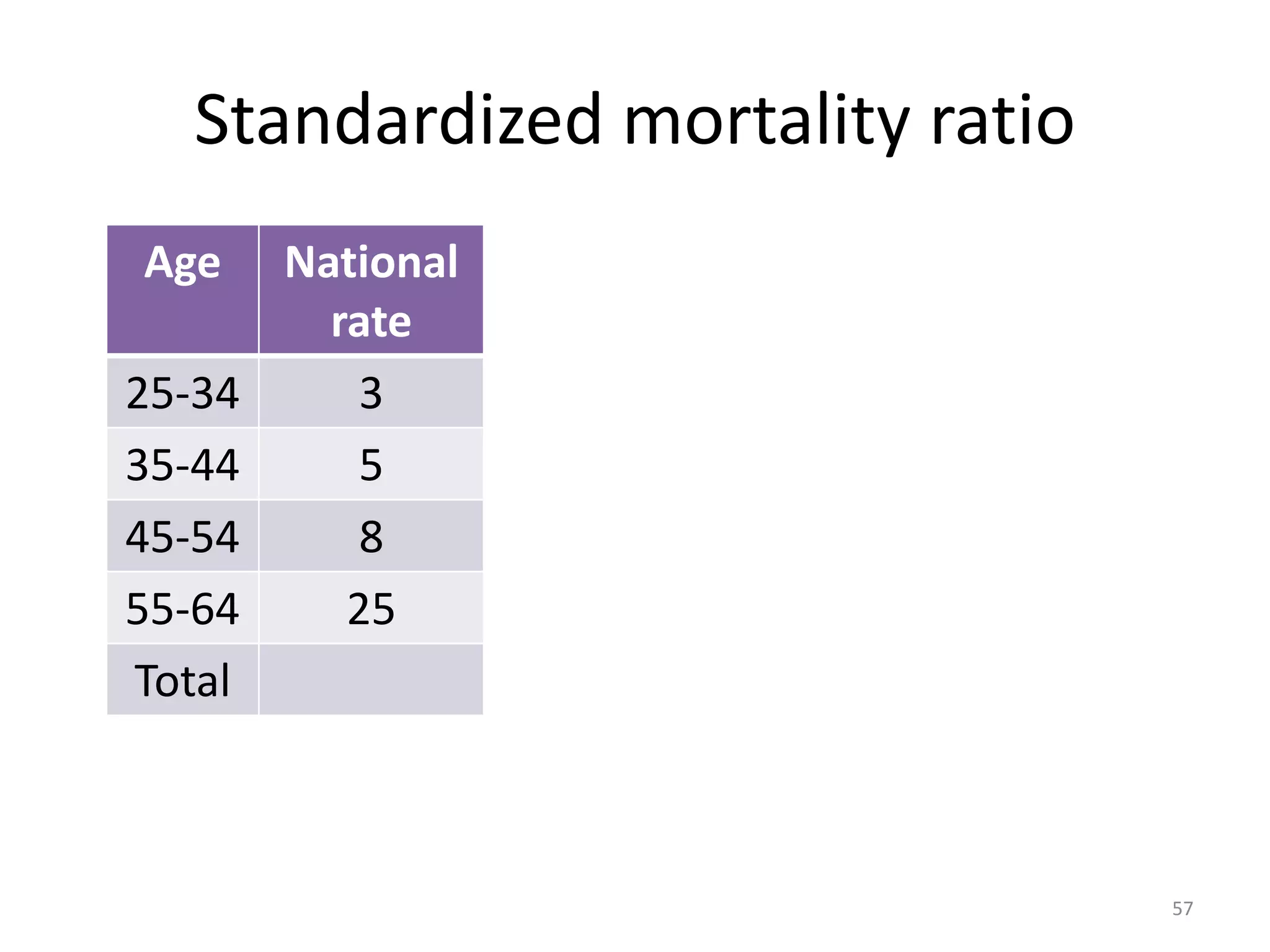
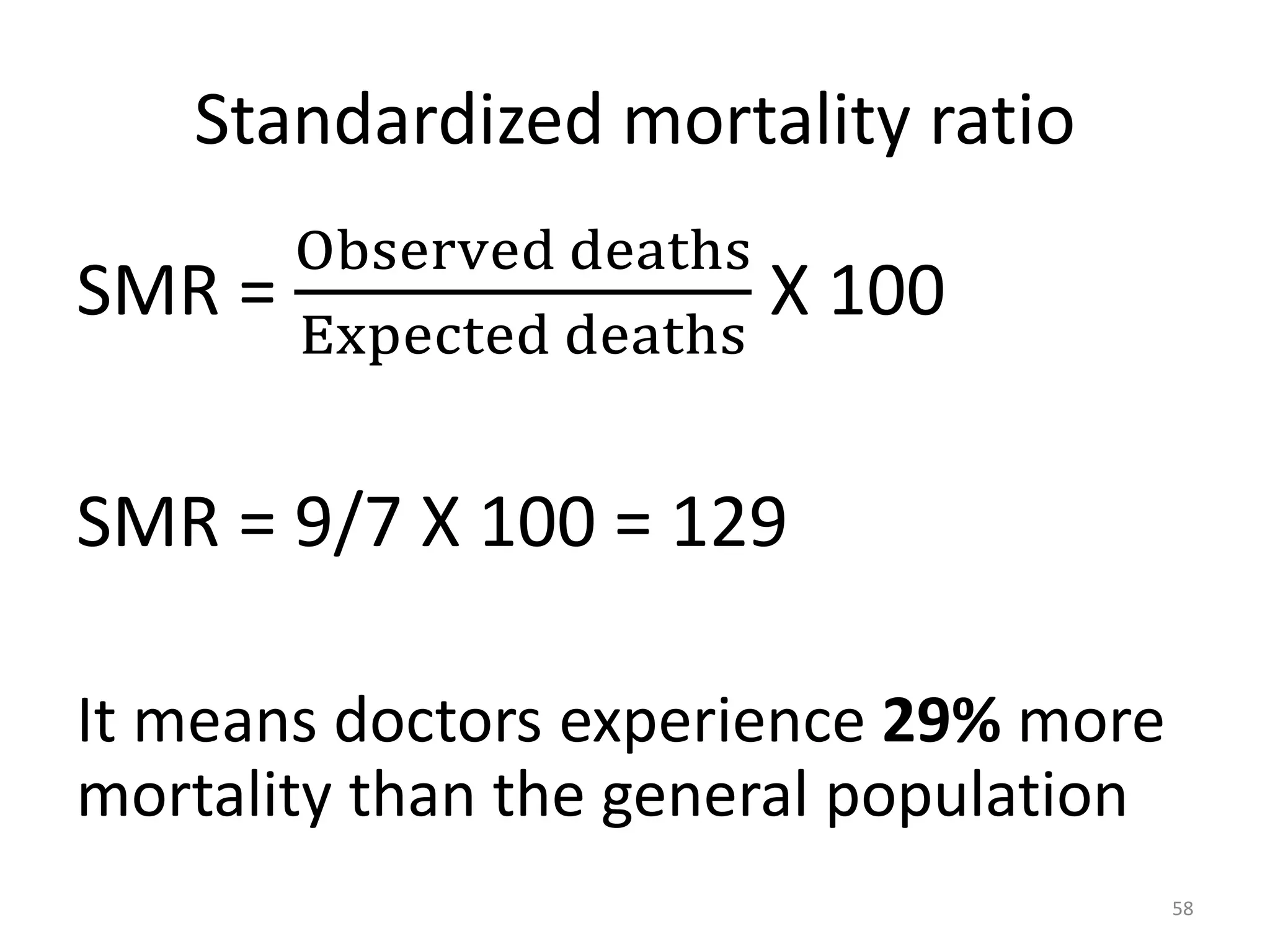
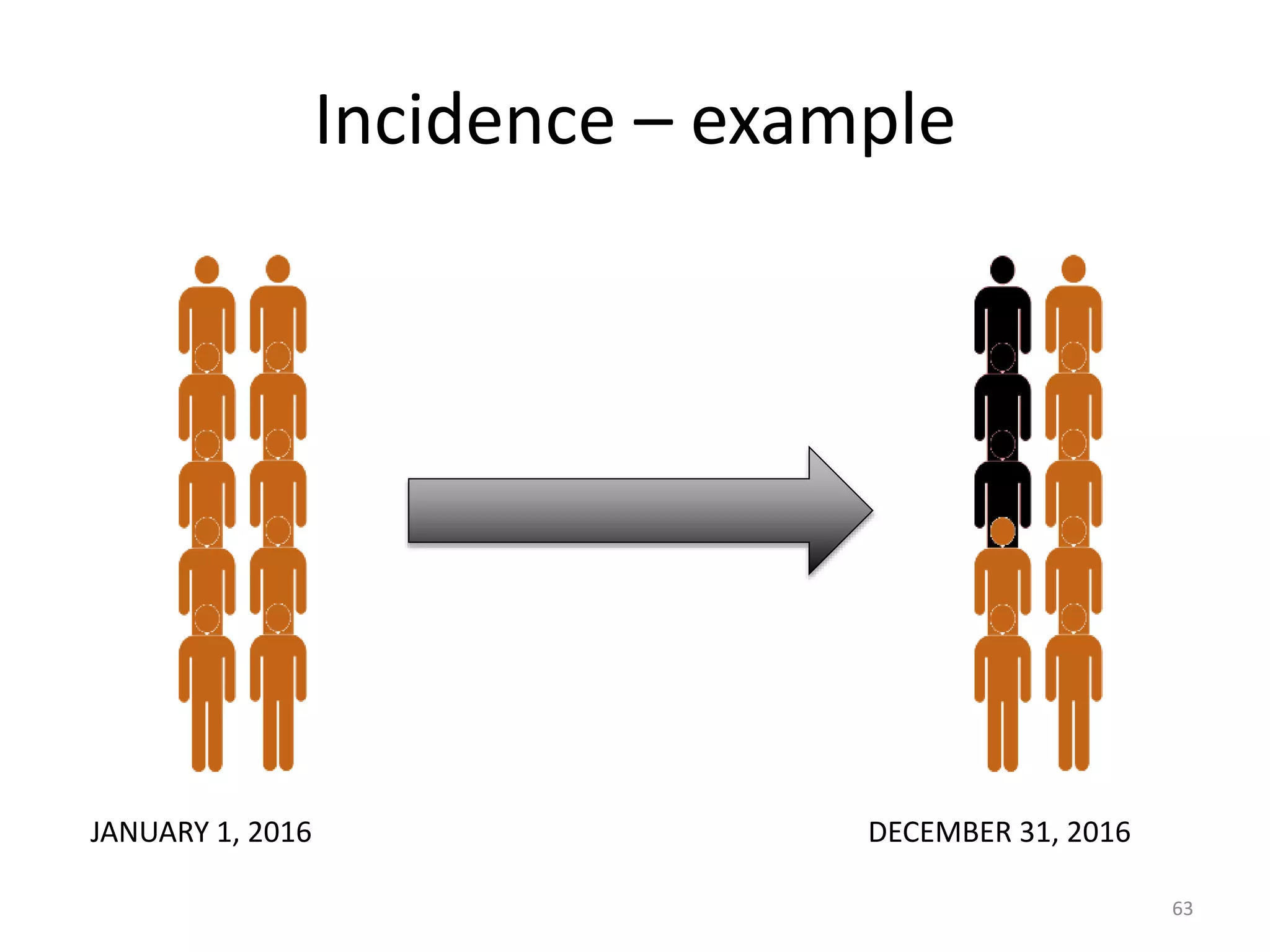
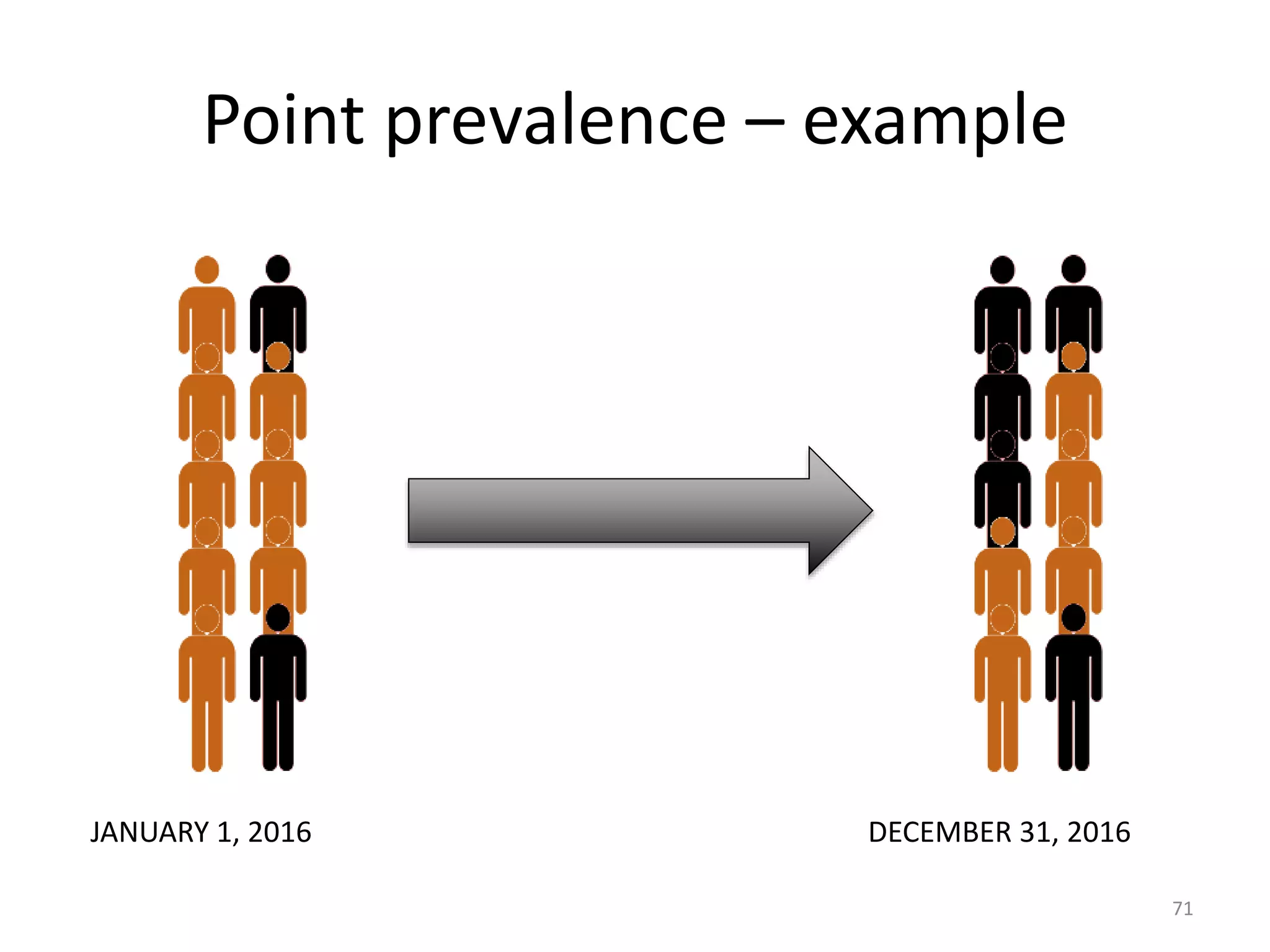
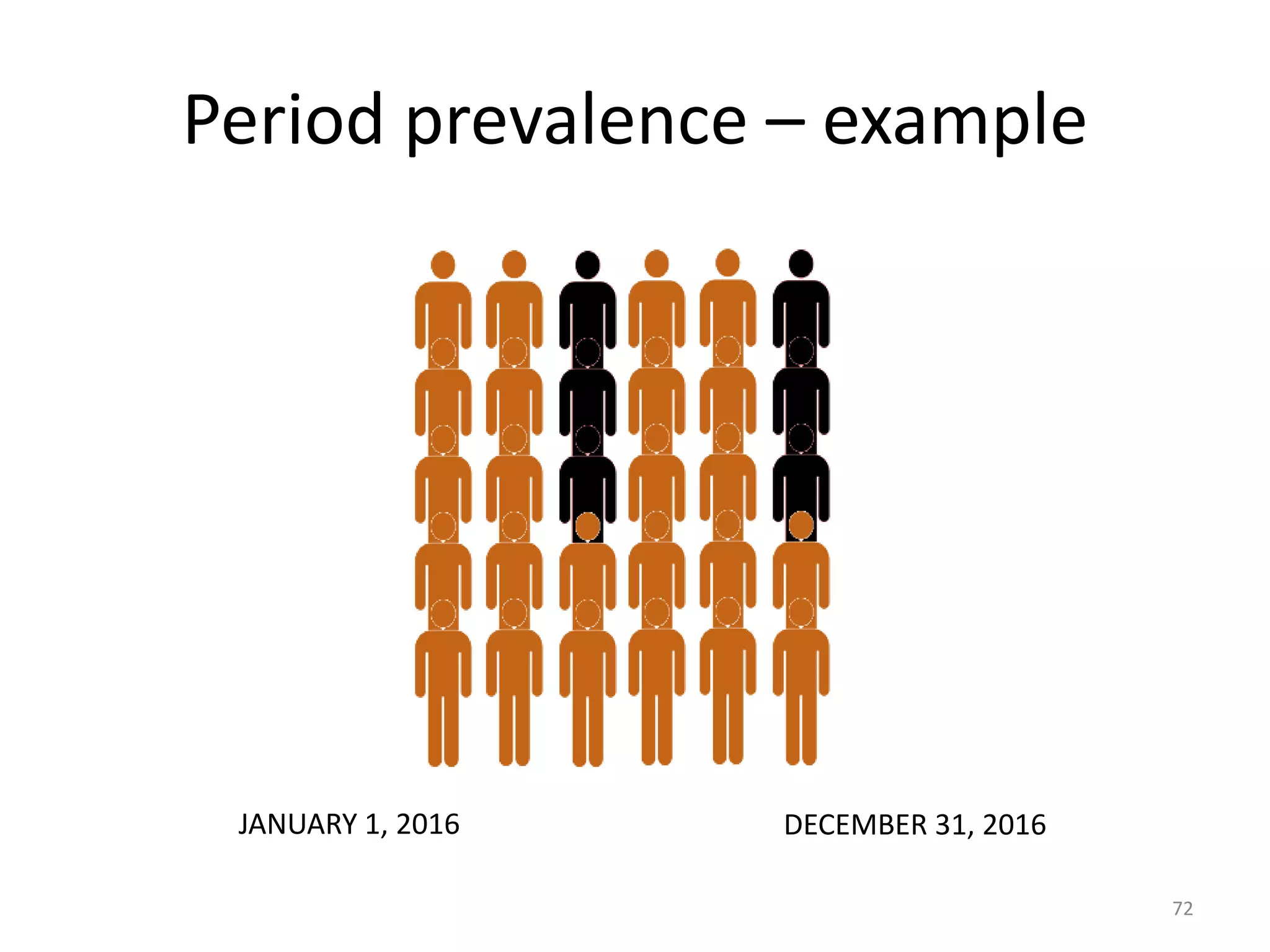
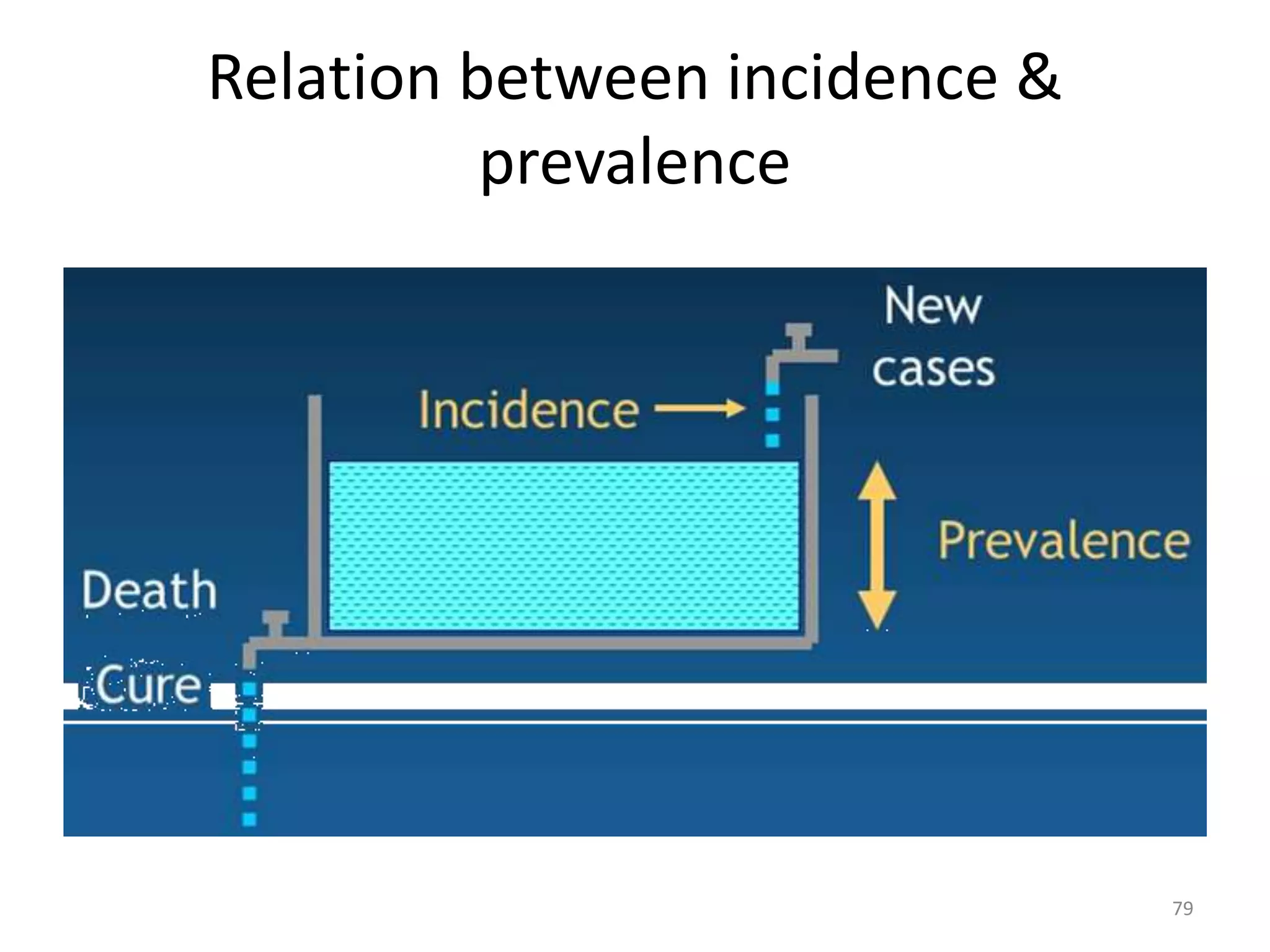



This document provides an overview of basic measurements used in epidemiology. It discusses tools like proportion, rate, and ratio. It also covers various measures of mortality like crude death rate, specific death rate, and proportional mortality rate. Measures of morbidity like incidence and prevalence are explained. The relationship between incidence and prevalence is described. Standardization techniques are introduced to make rates comparable between populations.























































































