Downloaded 1,054 times




Dr Pawan Kumar presented on MRI principles, techniques, and reading. MRI works by using a strong magnetic field to align proton spins in the body. Radiofrequency pulses excite the protons, causing them to emit signals as they relax back to equilibrium. These signals are used to form MRI images. Key hardware includes magnets, gradient coils, and RF coils. MRI contrast depends on tissue T1 and T2 relaxation times and the chosen TR and TE parameters. Different sequences like T1-weighted, T2-weighted, and FLAIR are used to highlight various tissues and pathologies. Contrast agents can also be used to improve tissue contrast on MRI scans.
Presentation by Dr. Pawan Kumar on MRI principles. NMR was discovered by Dr. Rabi; terms introduced by CJ Gorter and Nobel Prize winners Bloch & Purcell.
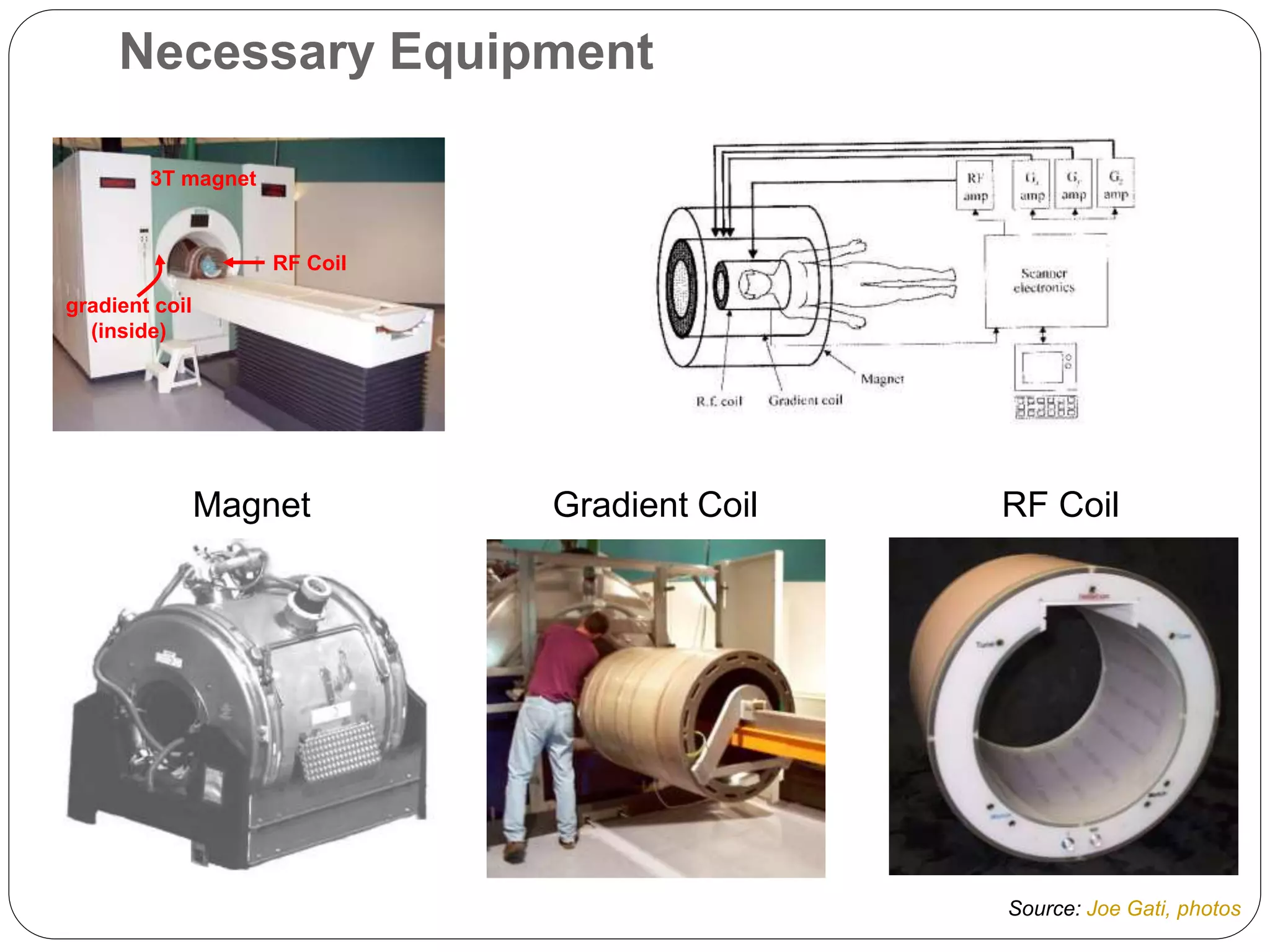
Overview of MRI hardware: permanent, resistive, and superconducting magnets; RF coils for signal transmission and reception.
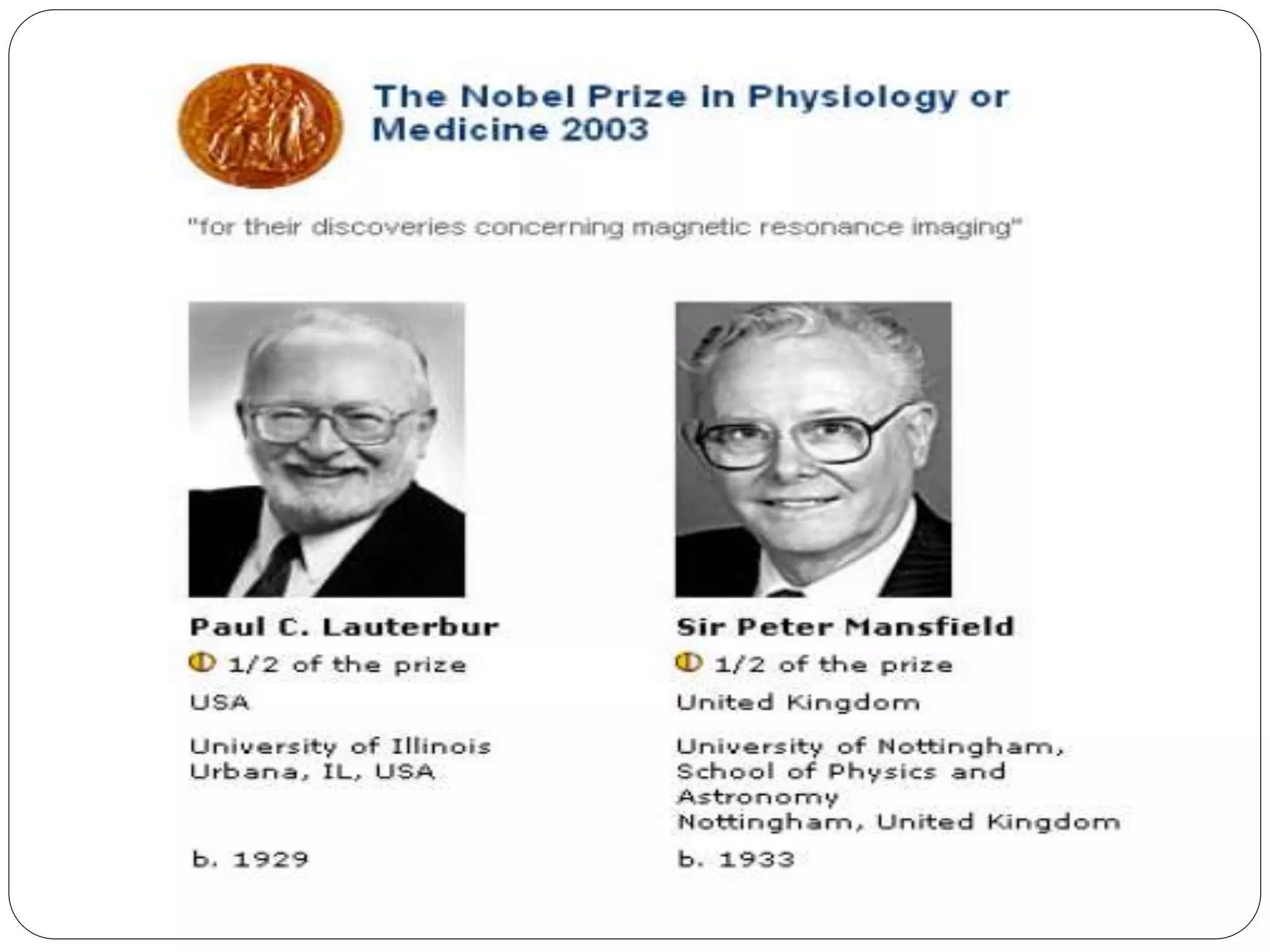
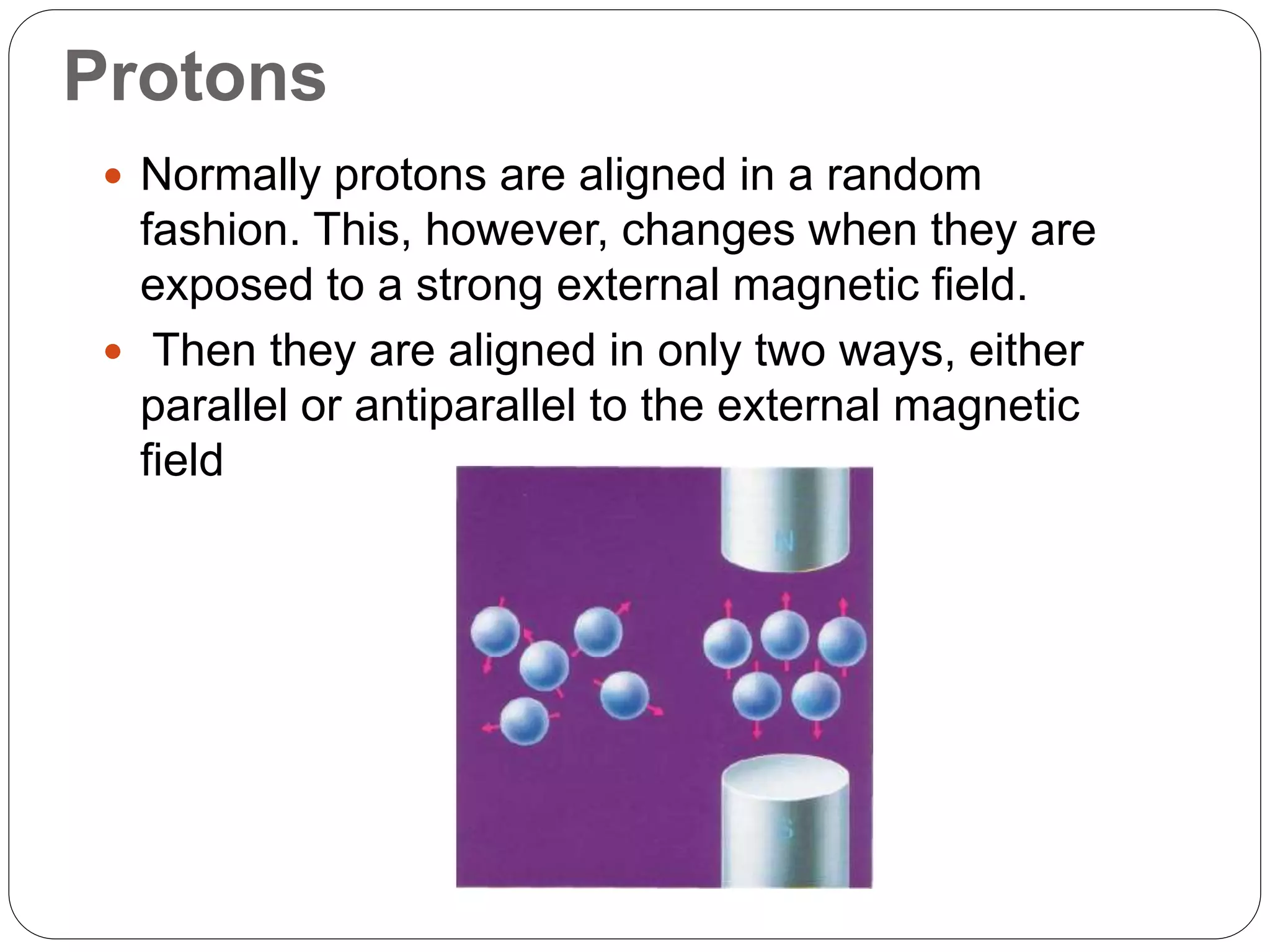
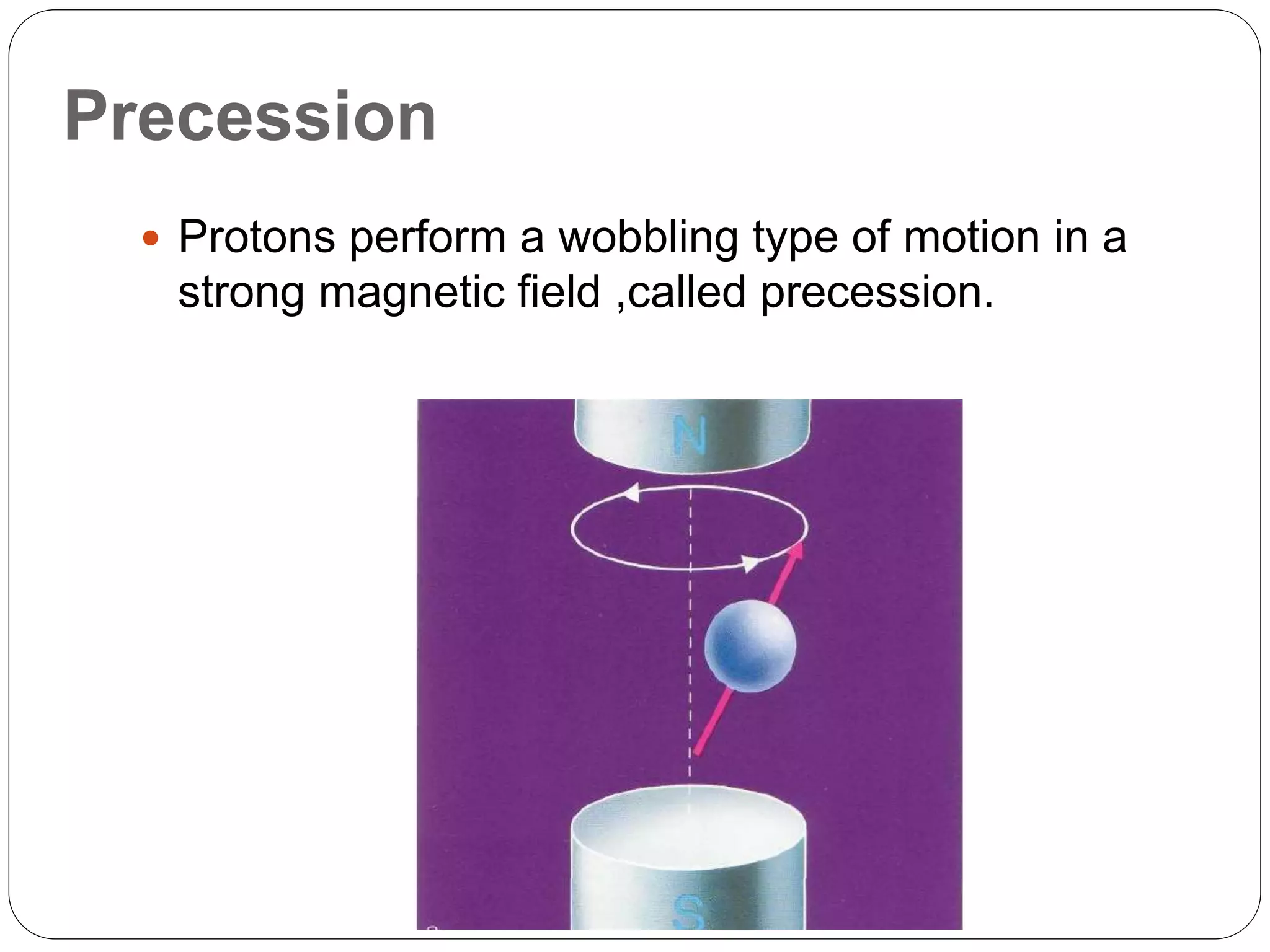
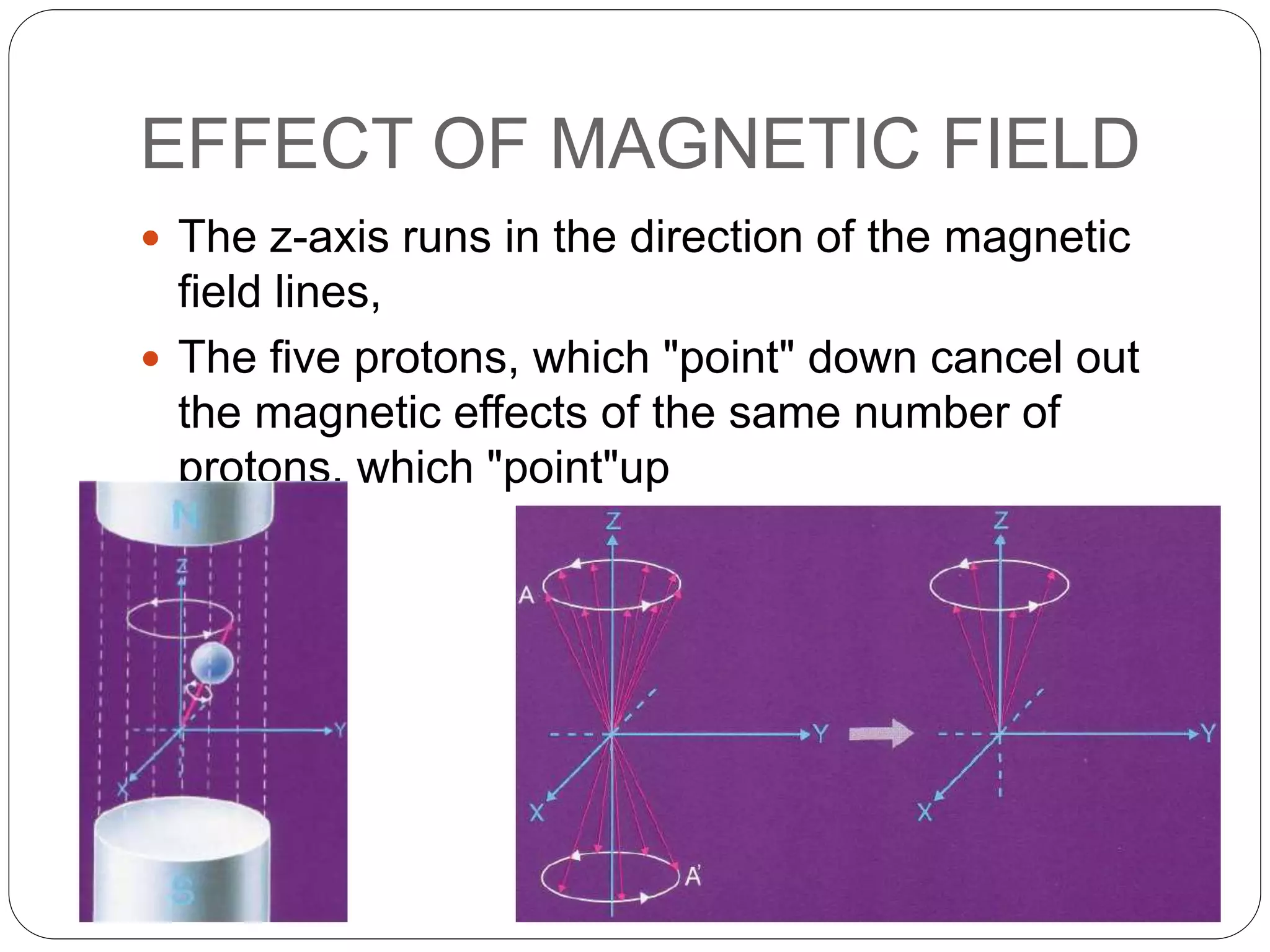
MRI operates on nuclear magnetic resonance principles, focusing on protons’ alignment and precession in magnetic fields.
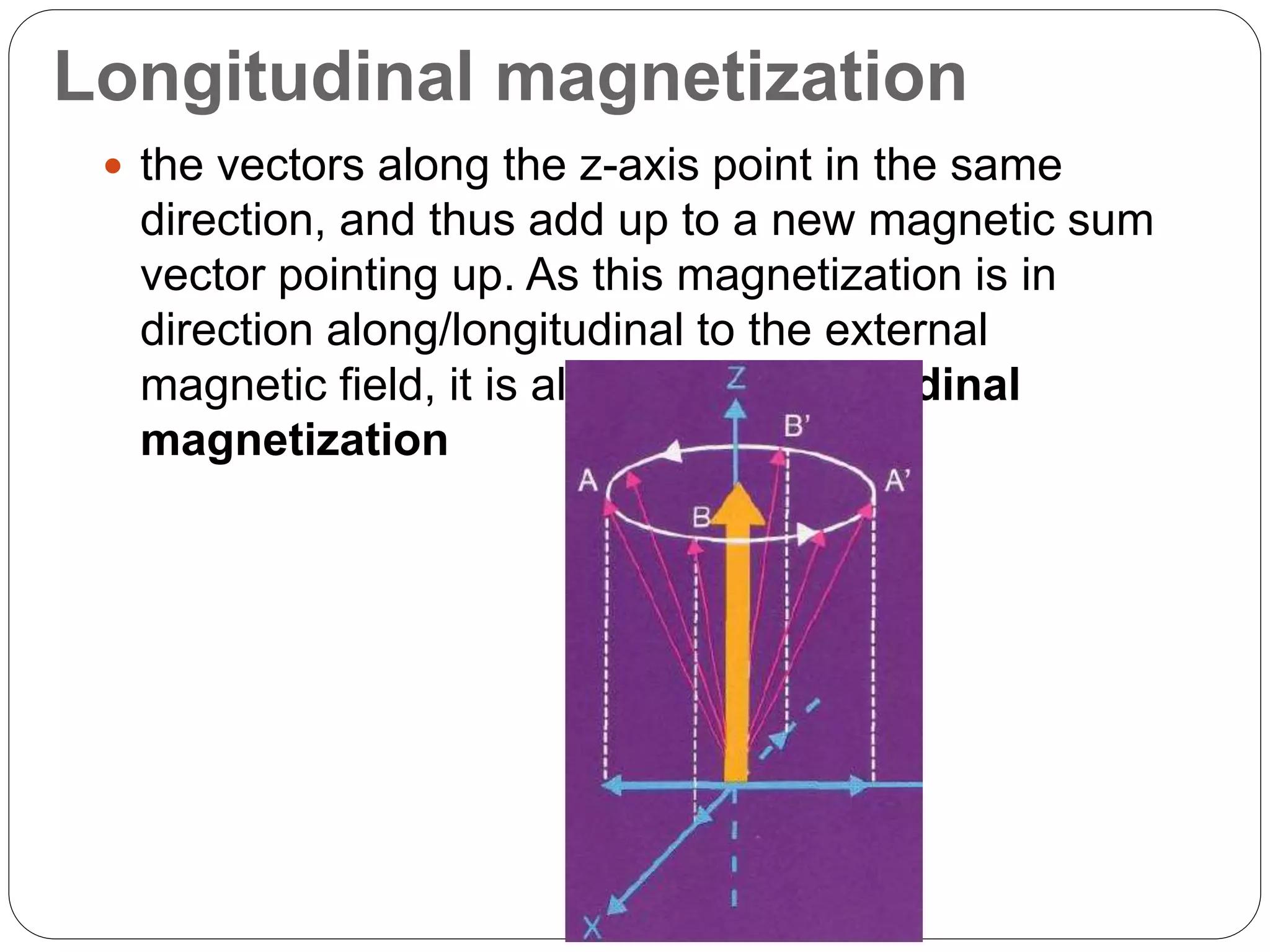
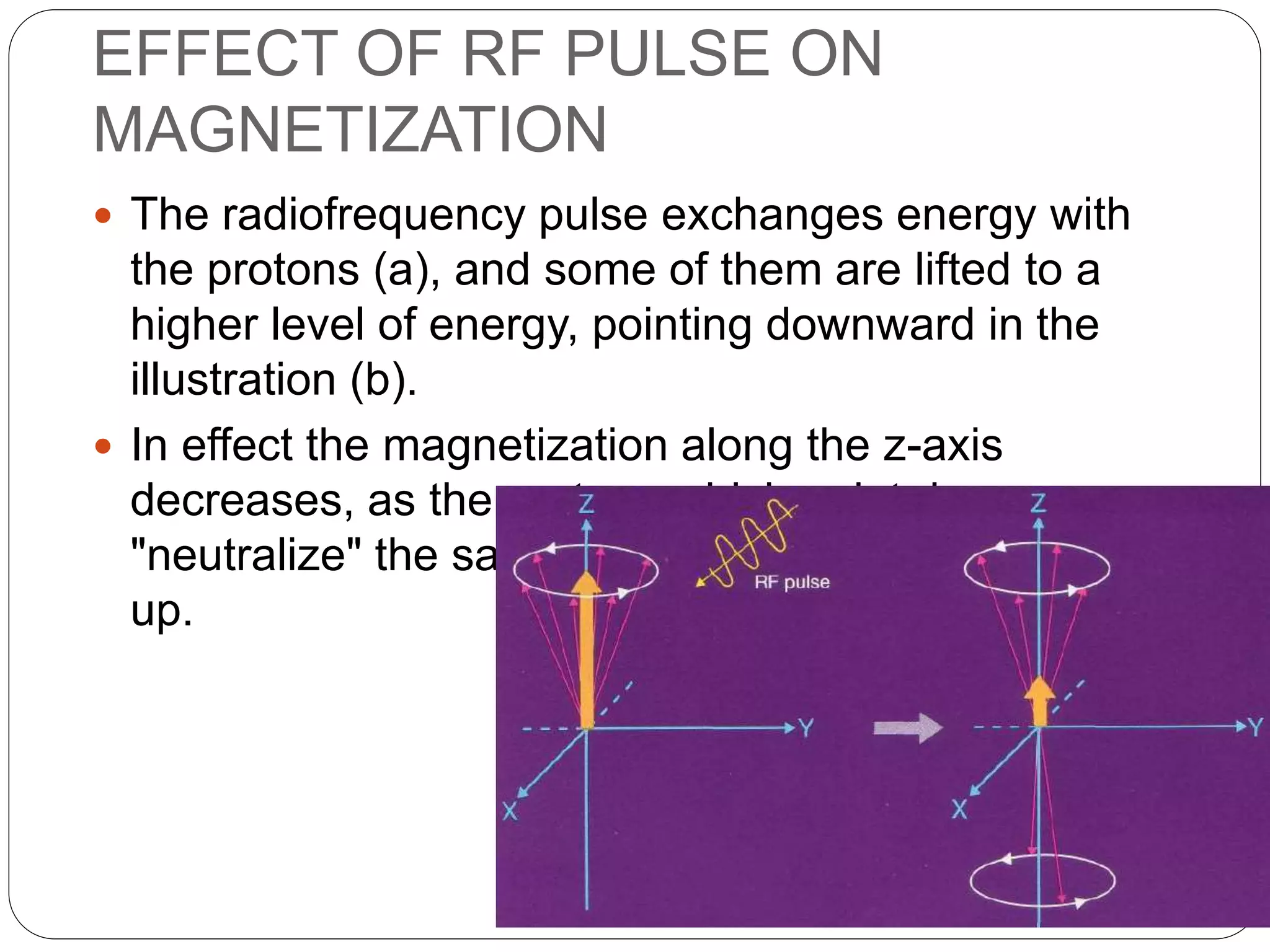
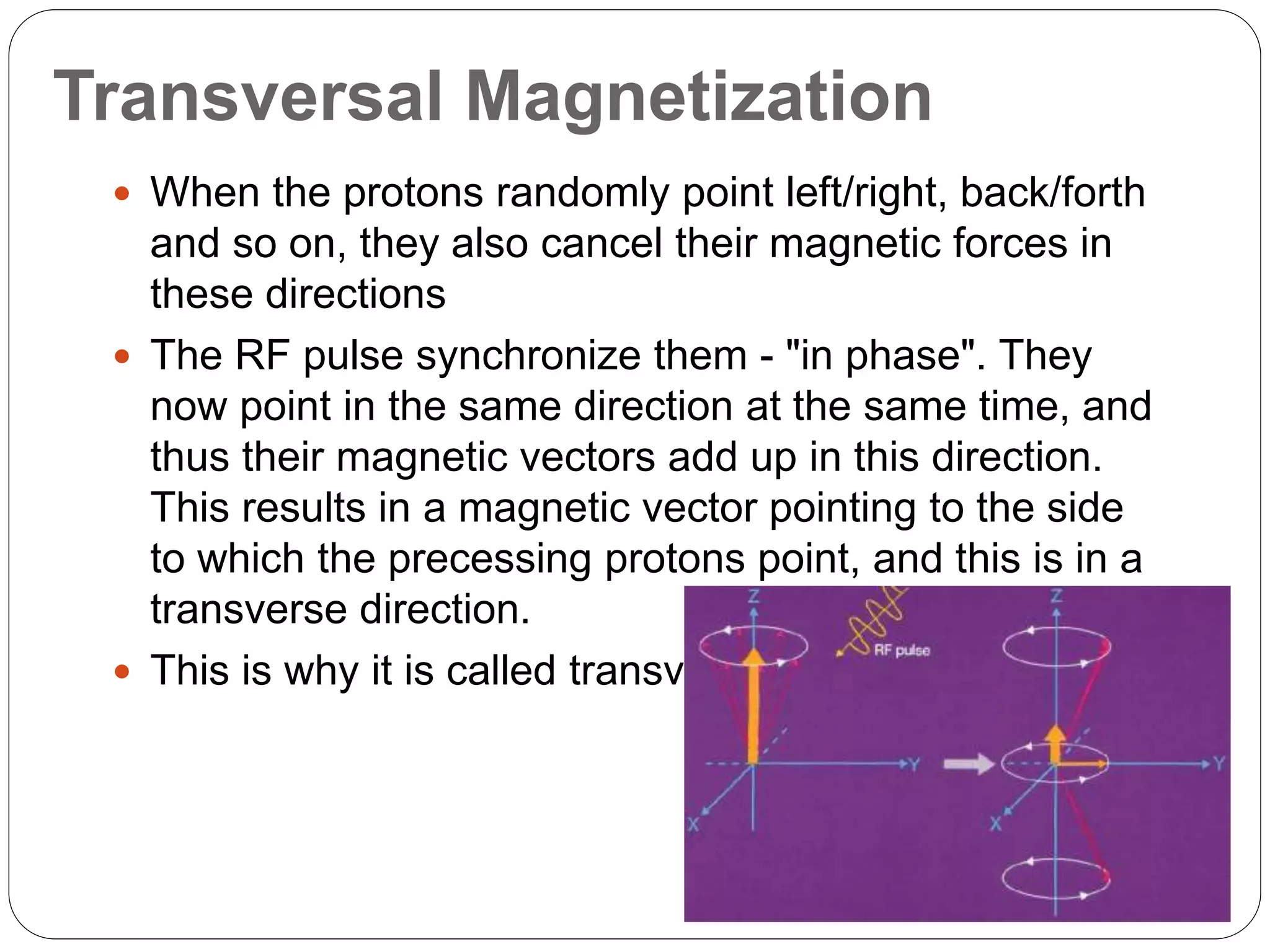
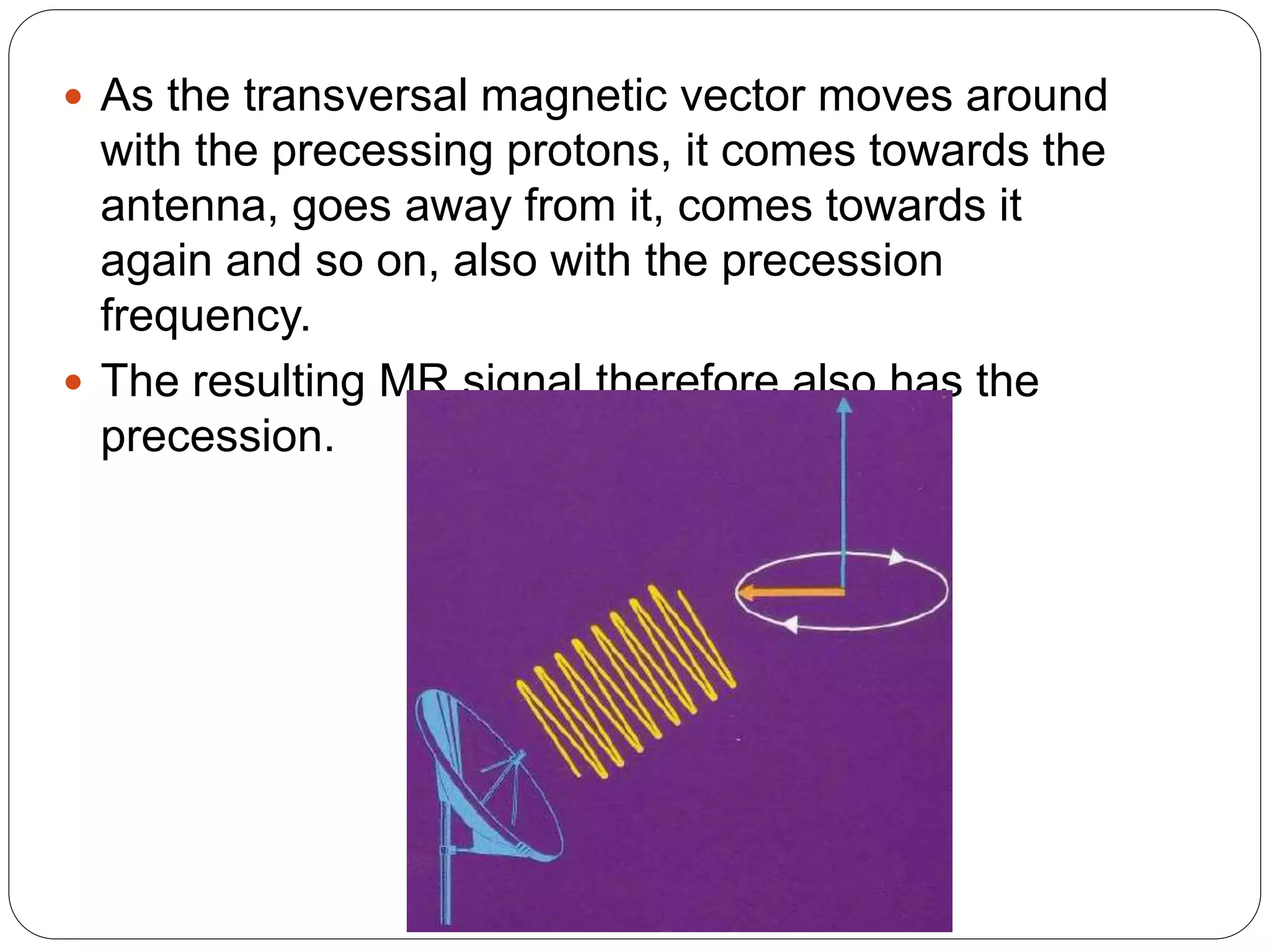
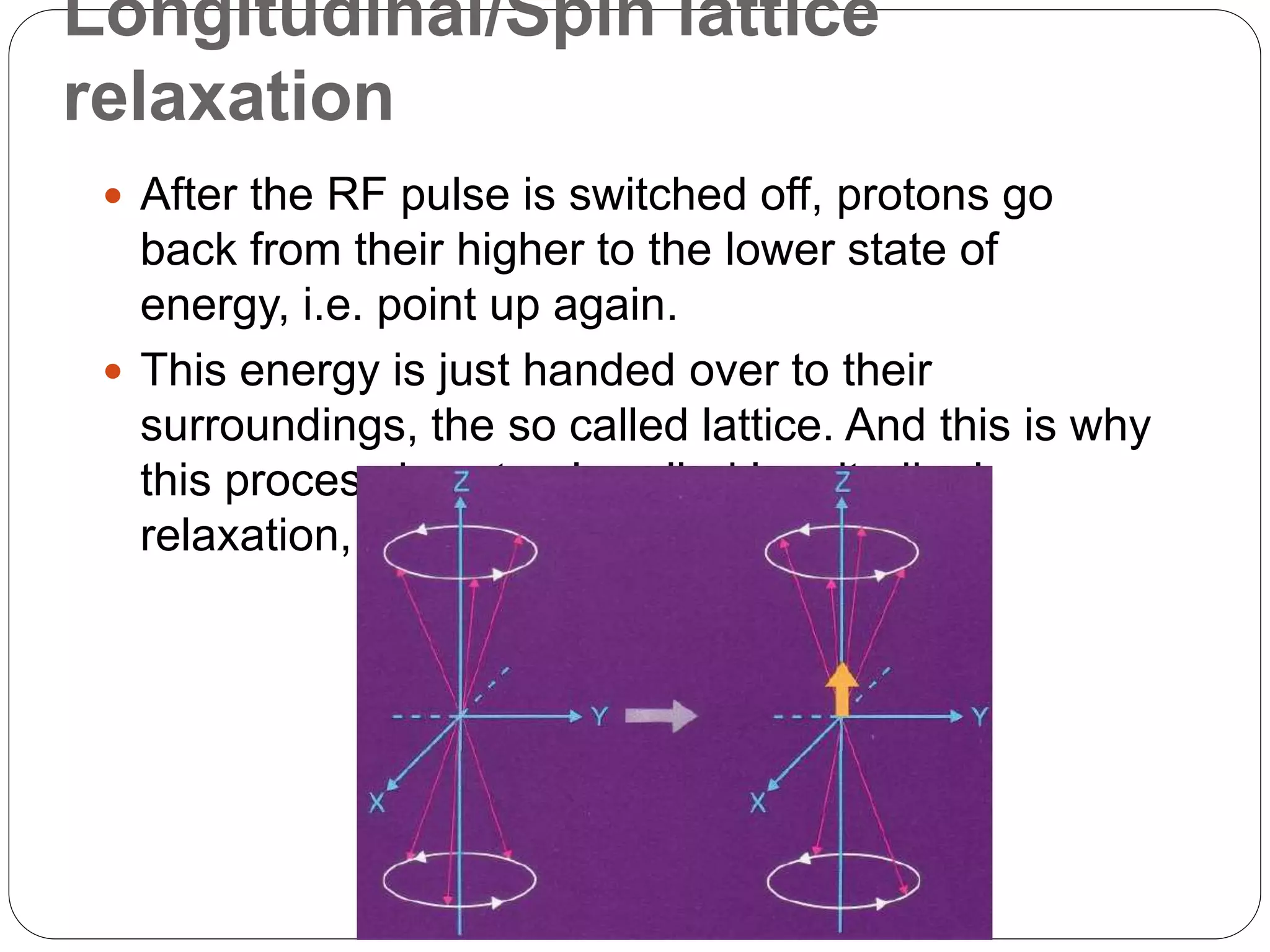
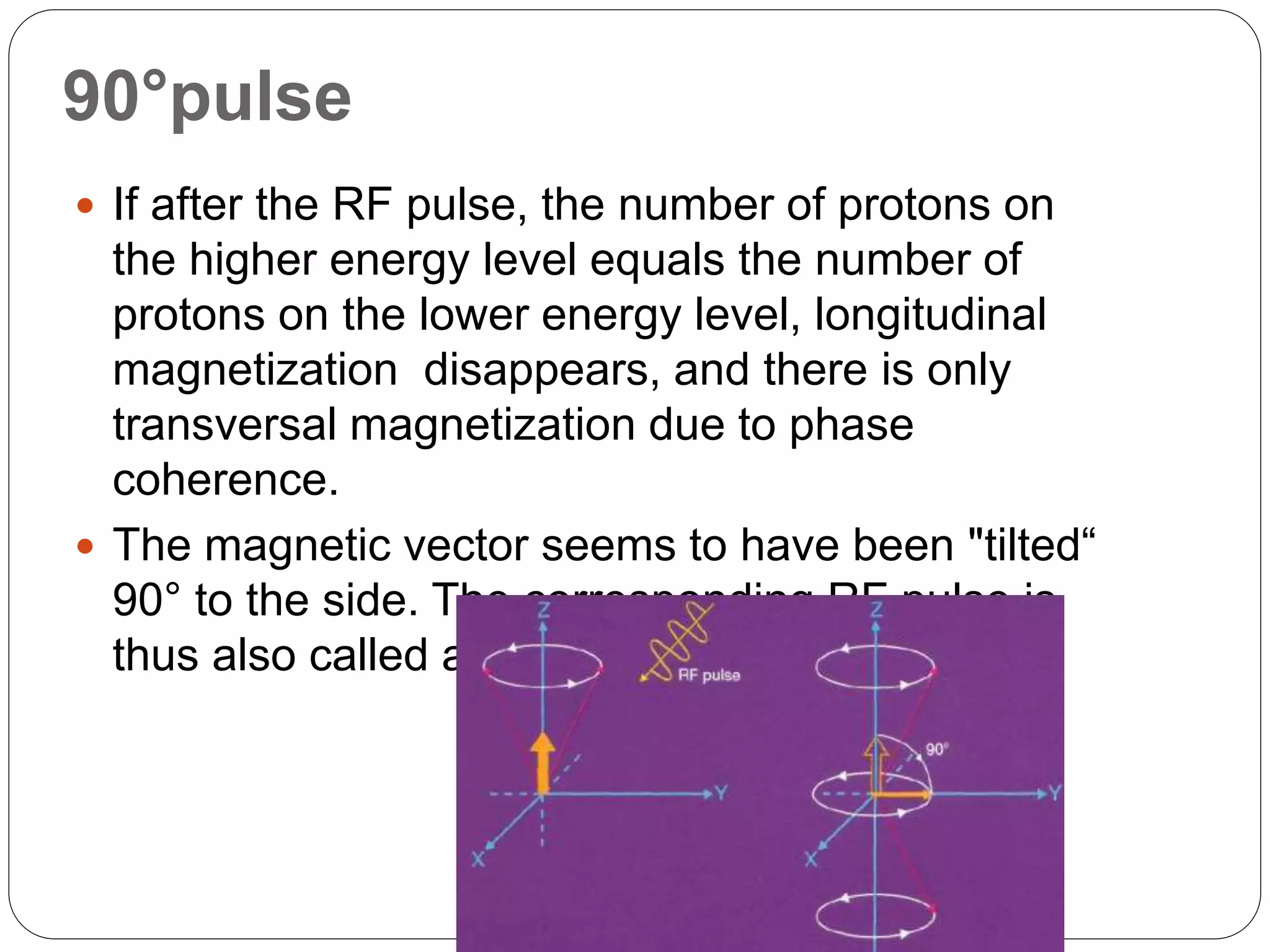
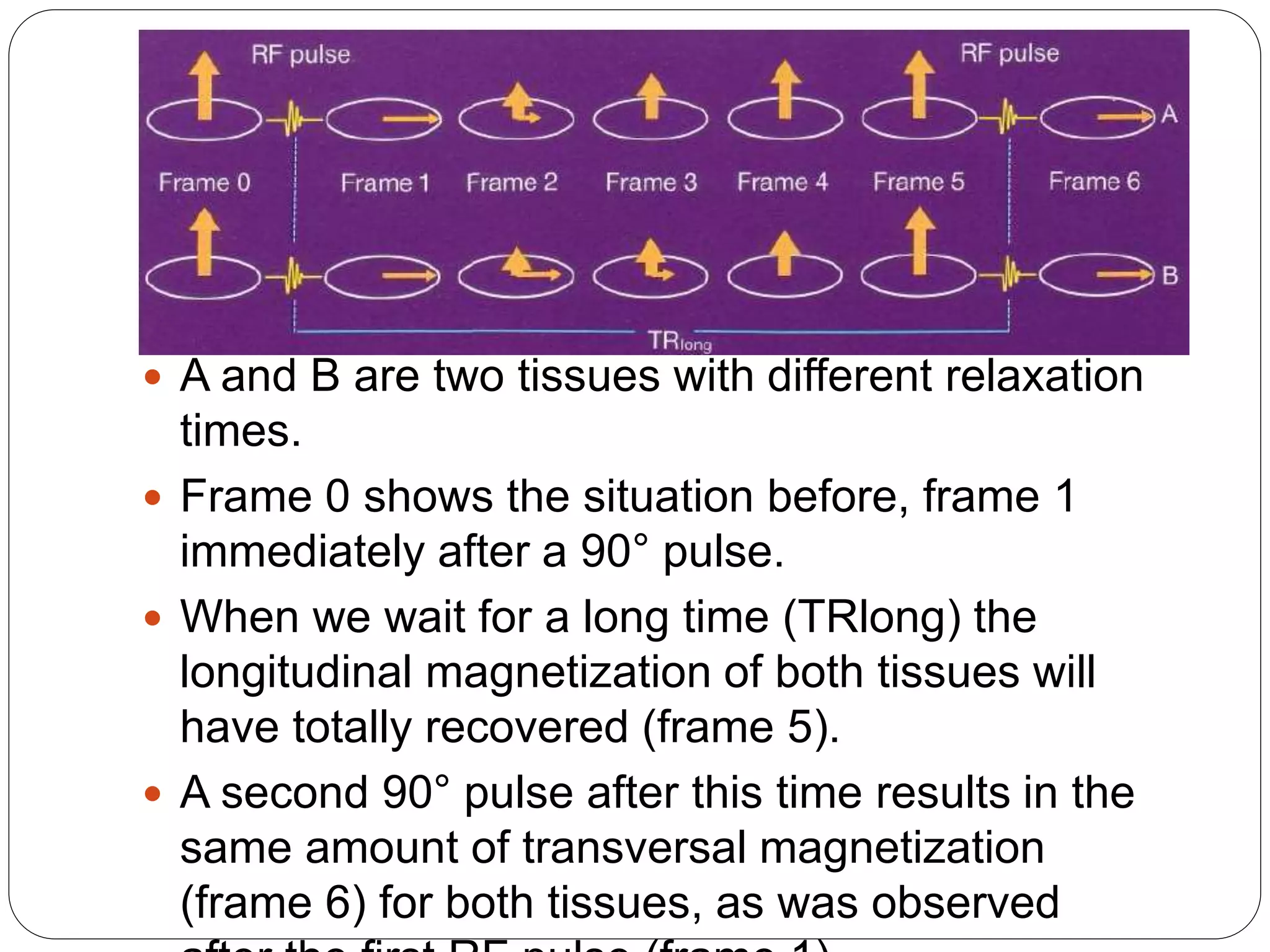
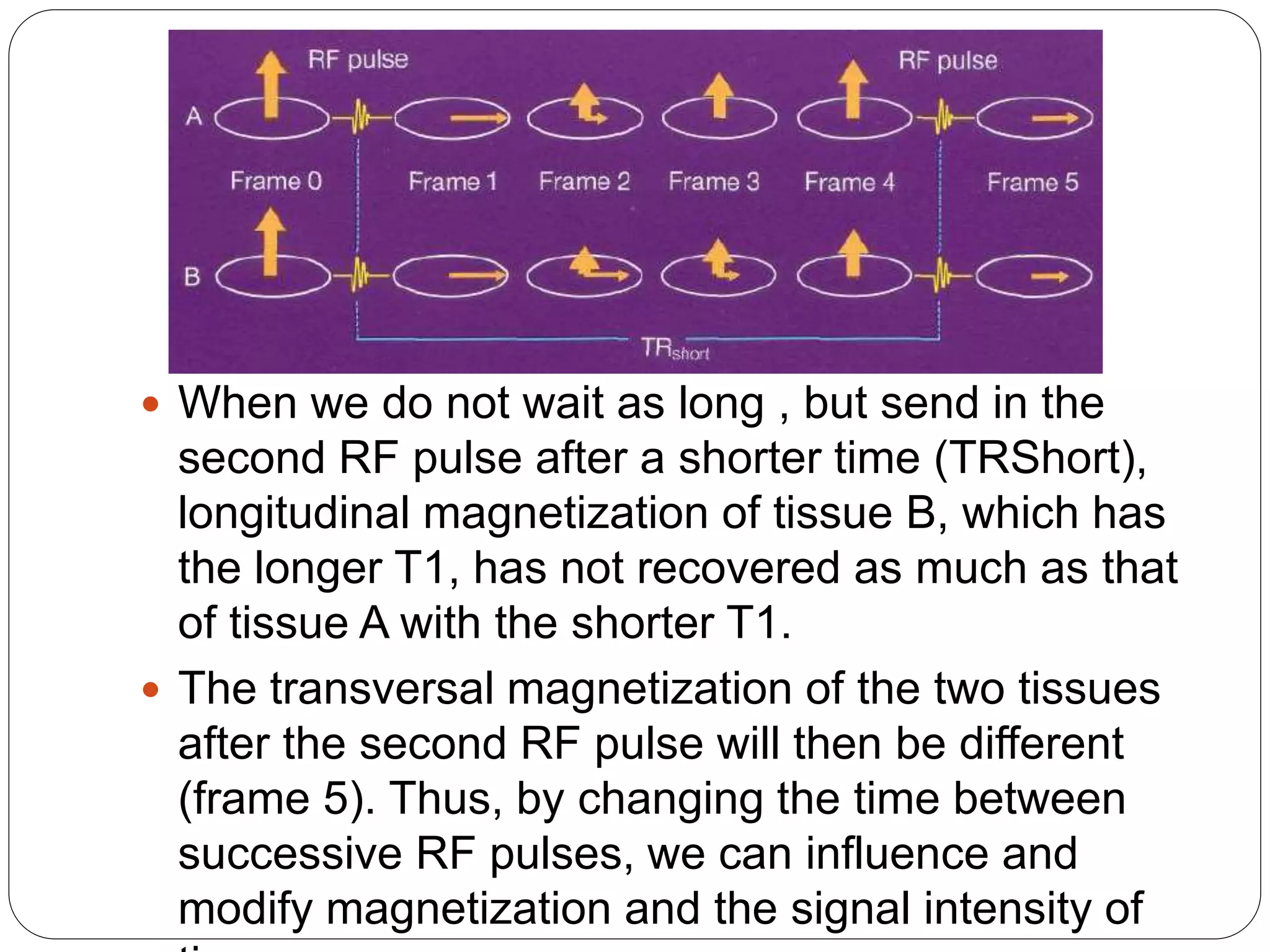
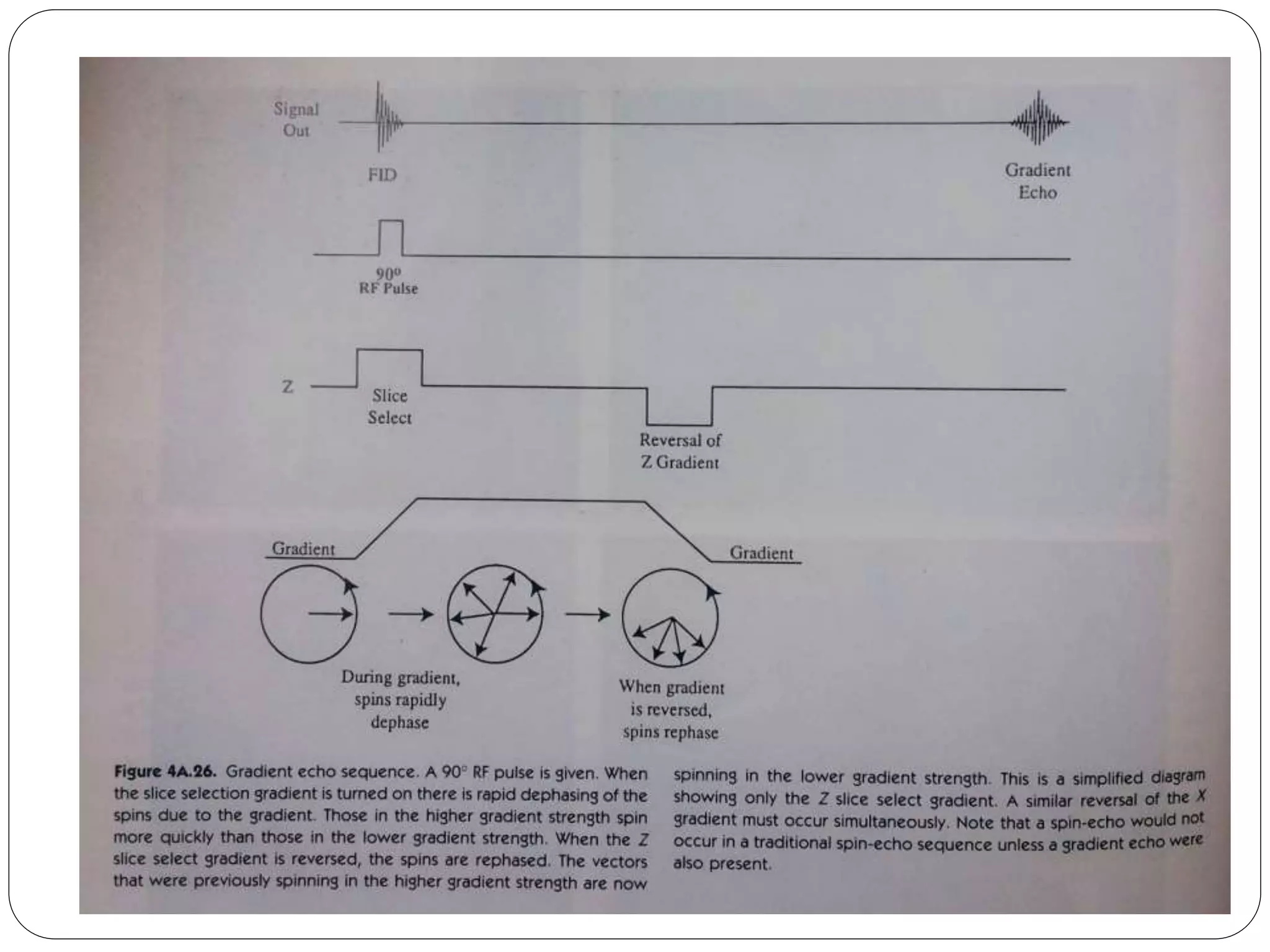
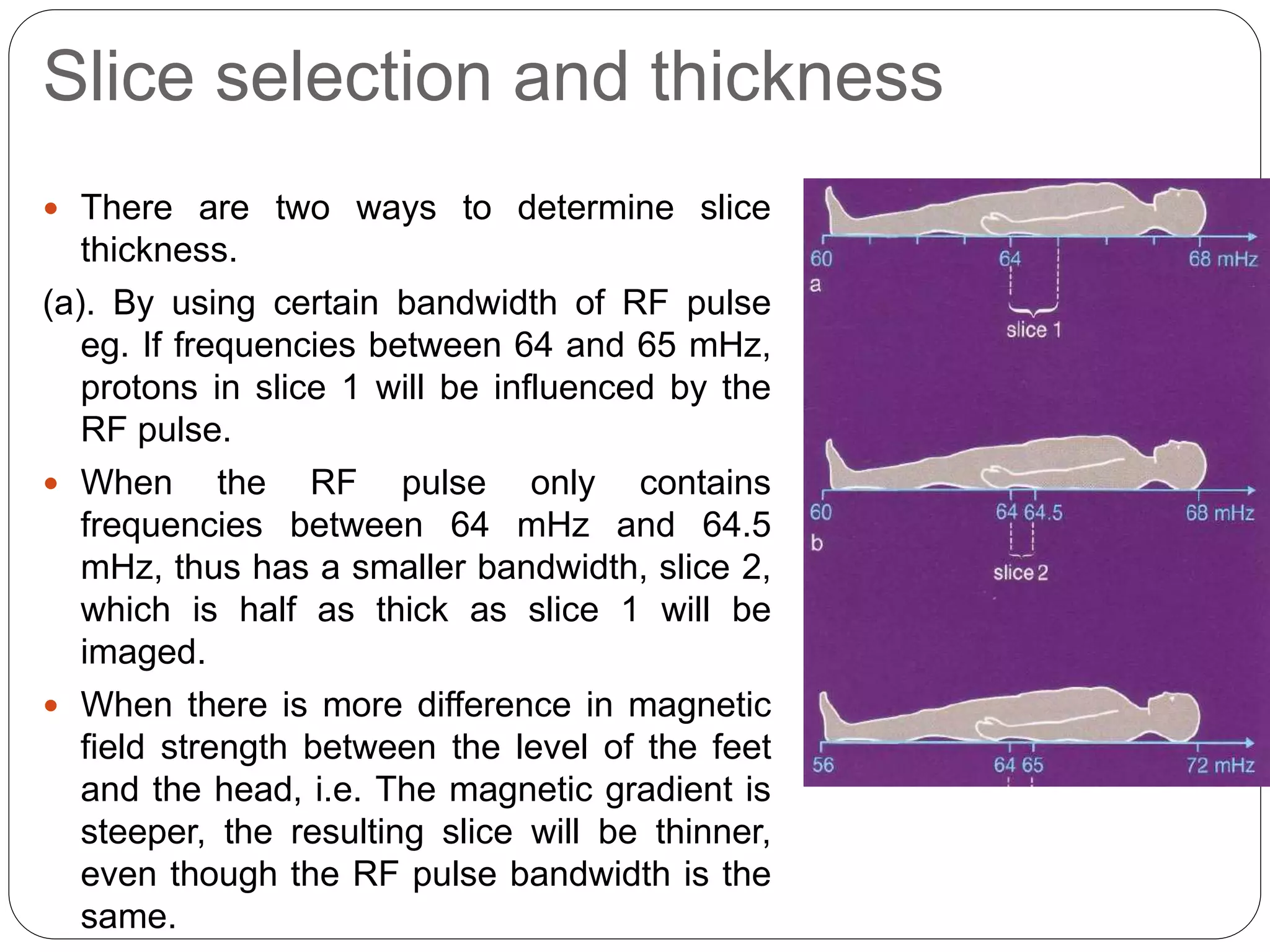
Explains RF pulses' effects on protons’ alignment and magnetization. Concepts of longitudinal and transversal magnetization are clarified.
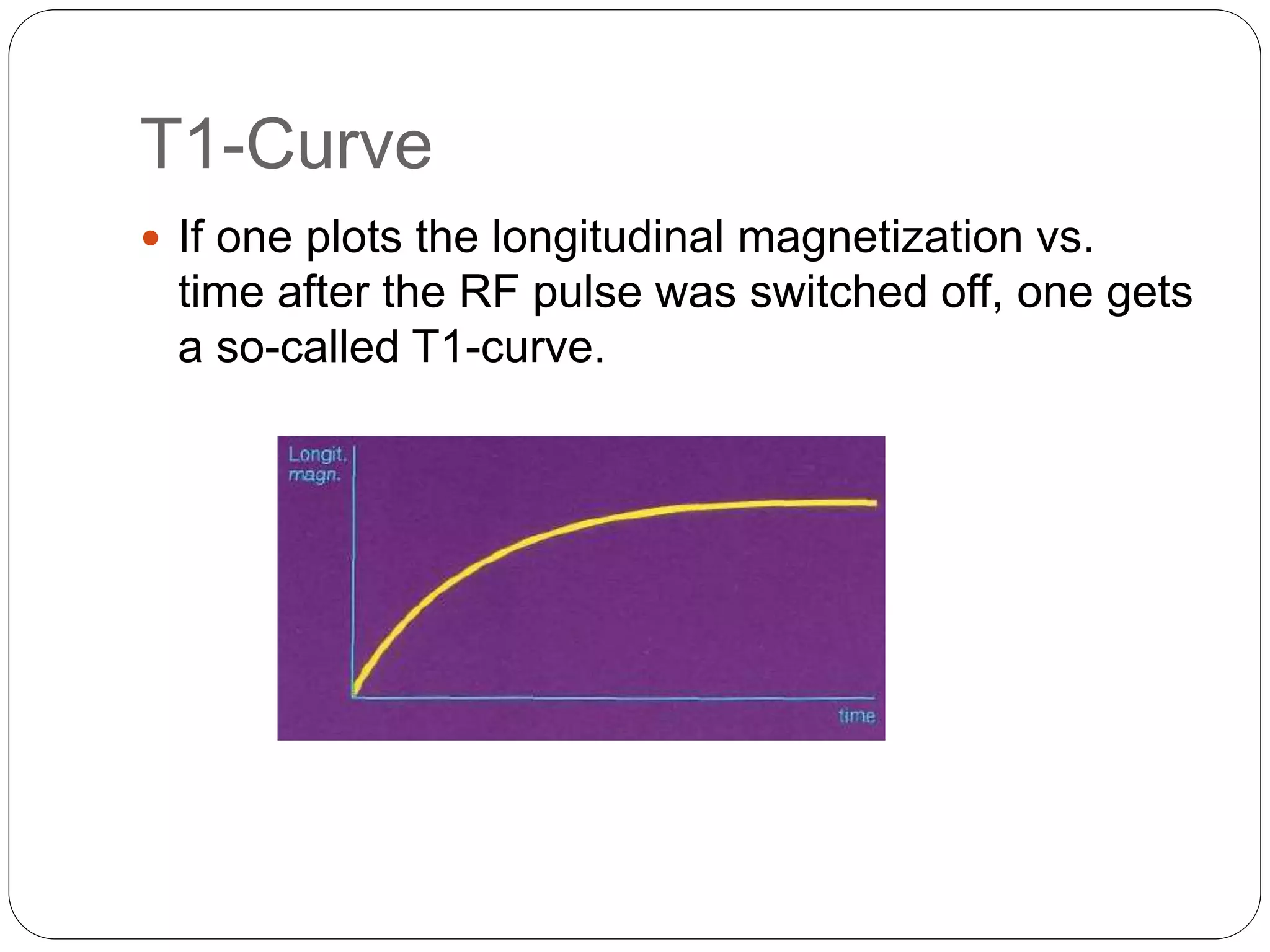
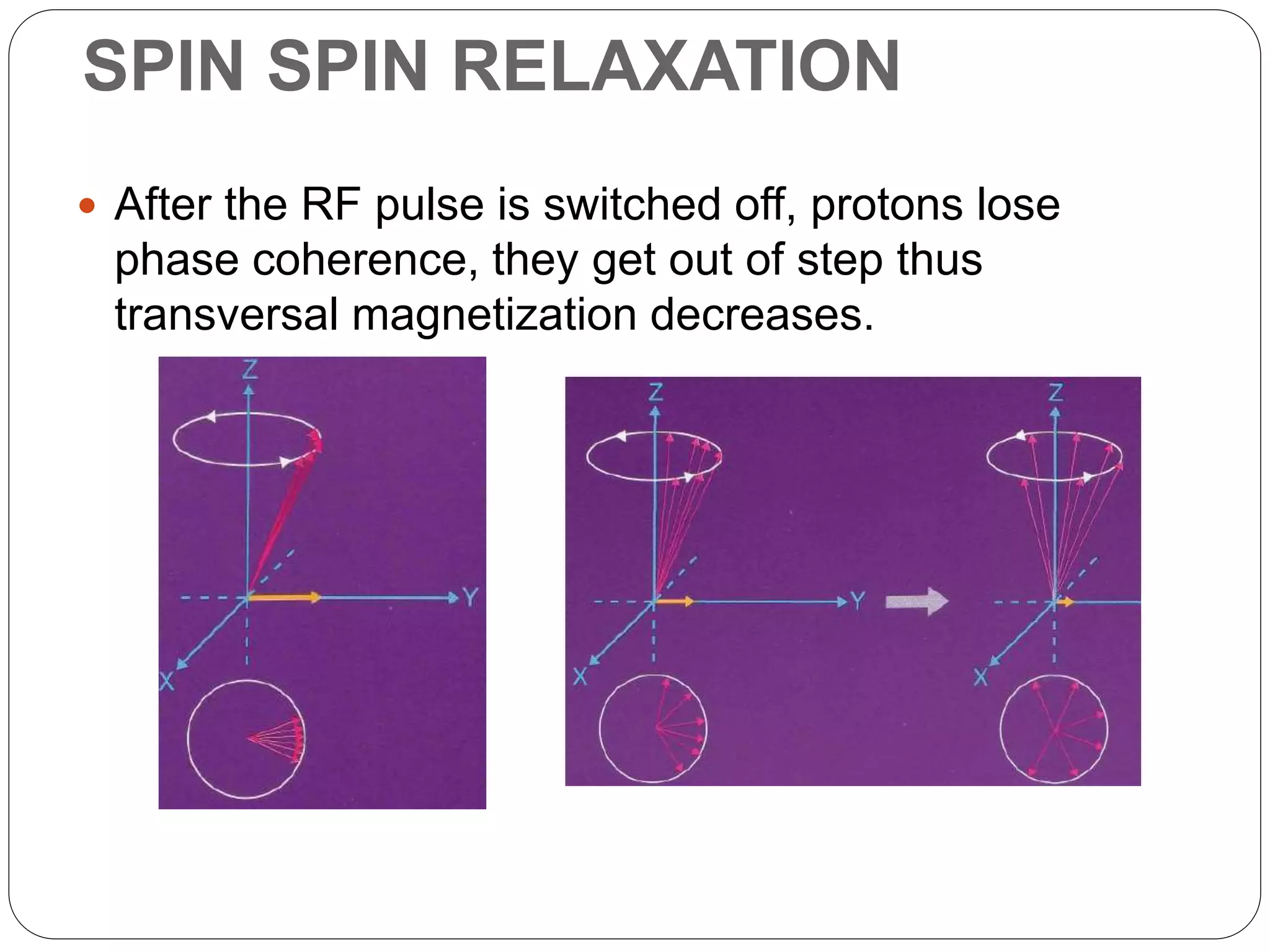
Discusses longitudinal (T1) and transversal (T2) relaxation, their meanings, and their implications in MRI signal representation.
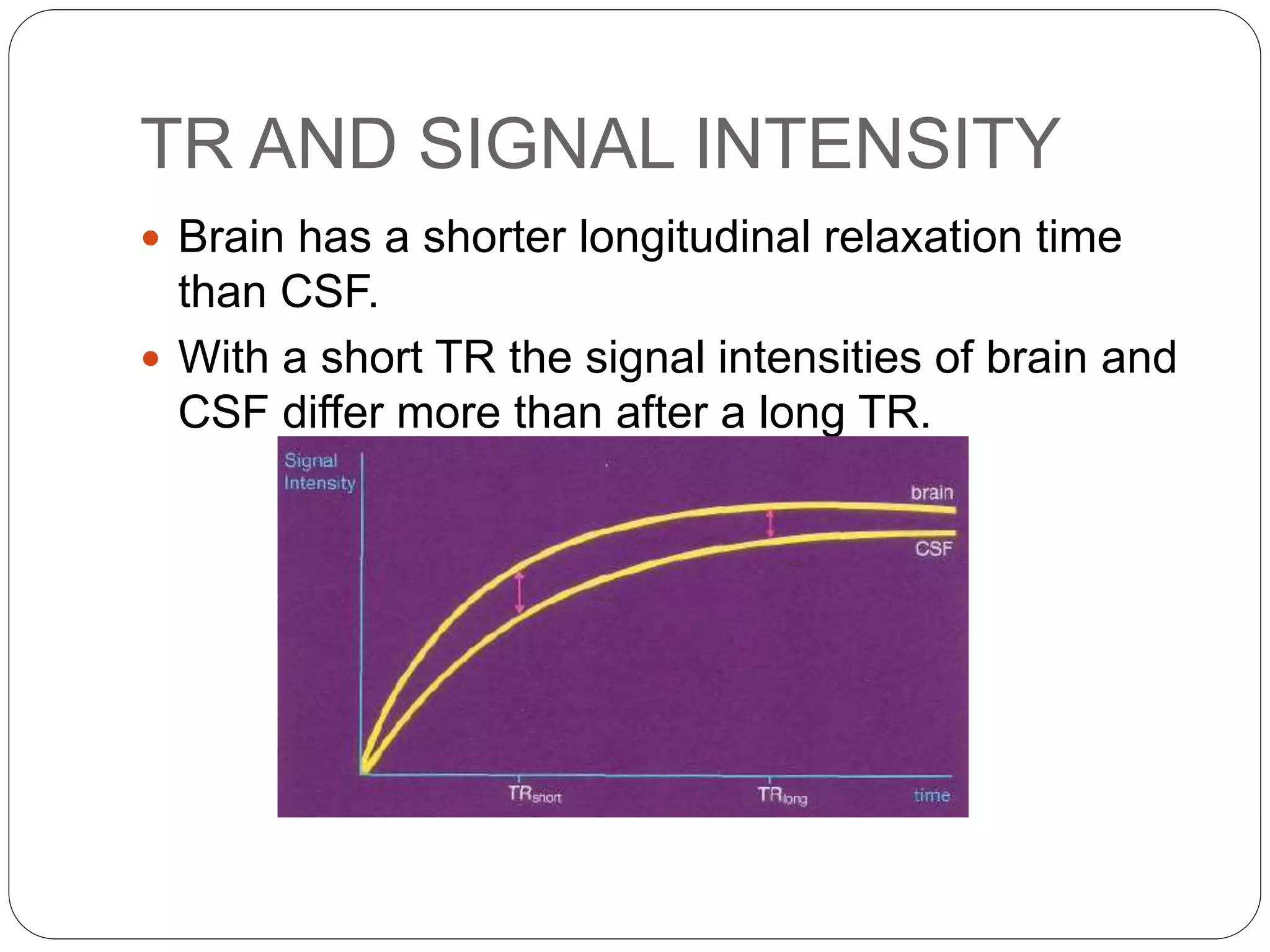
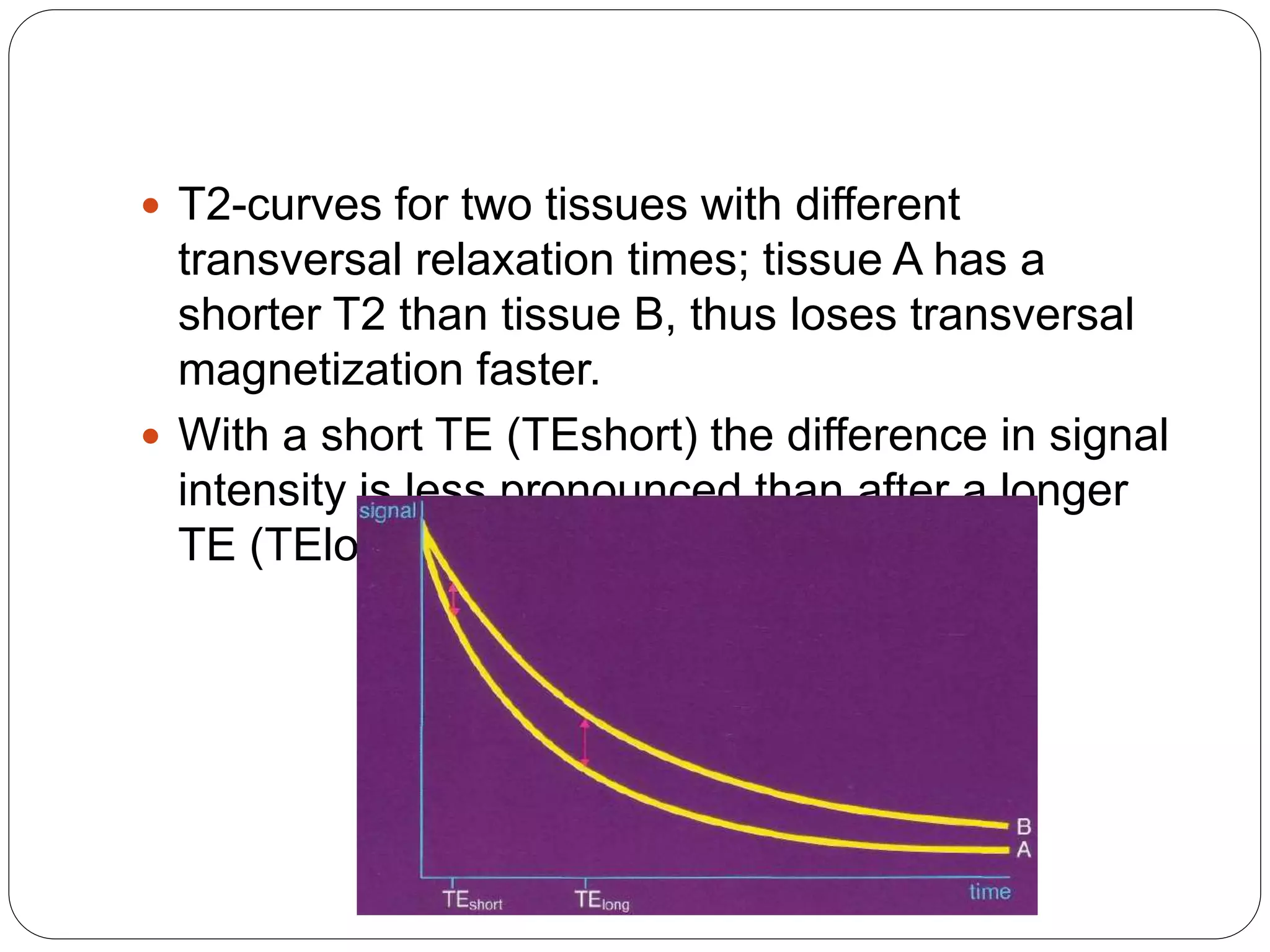
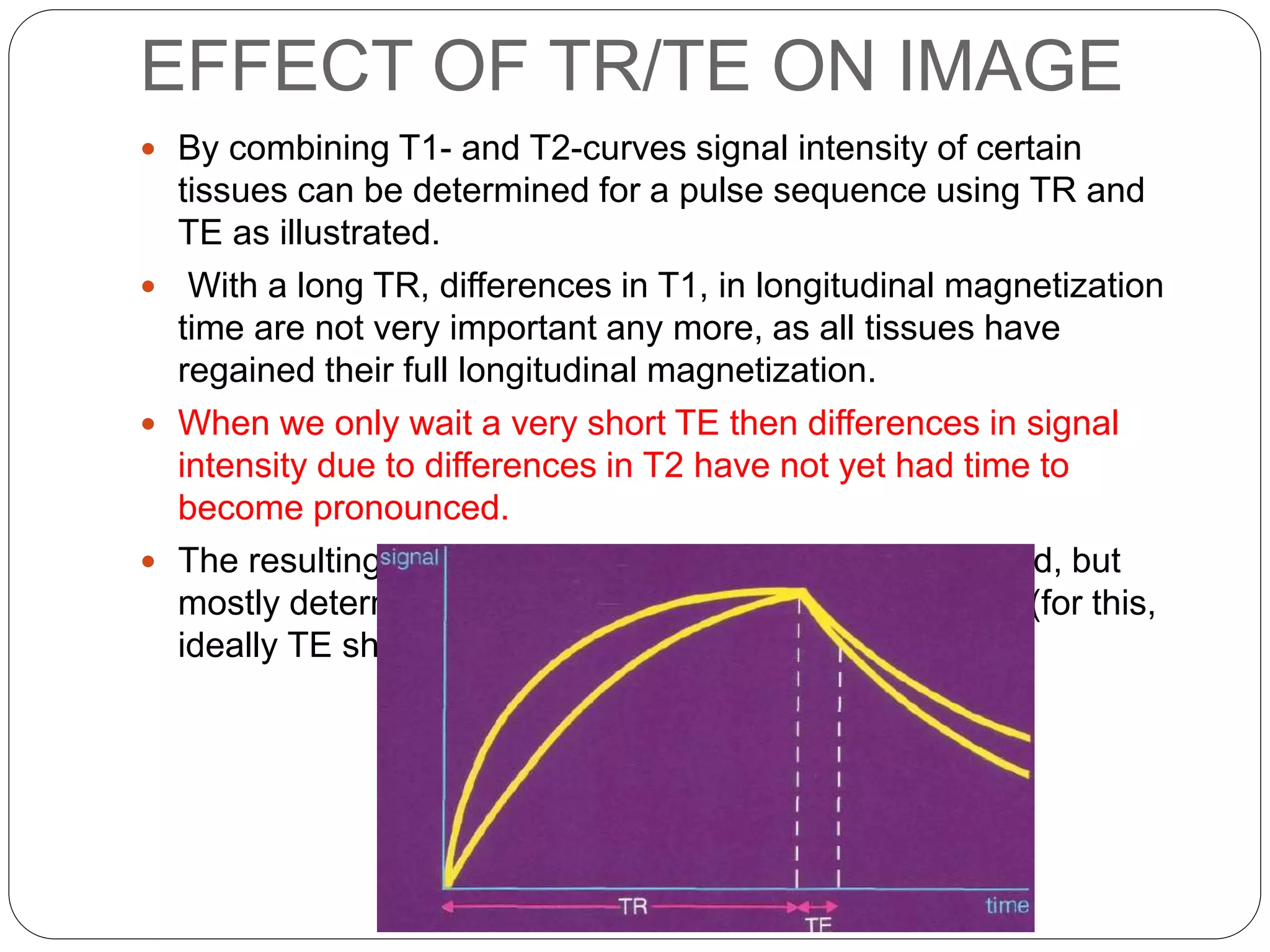
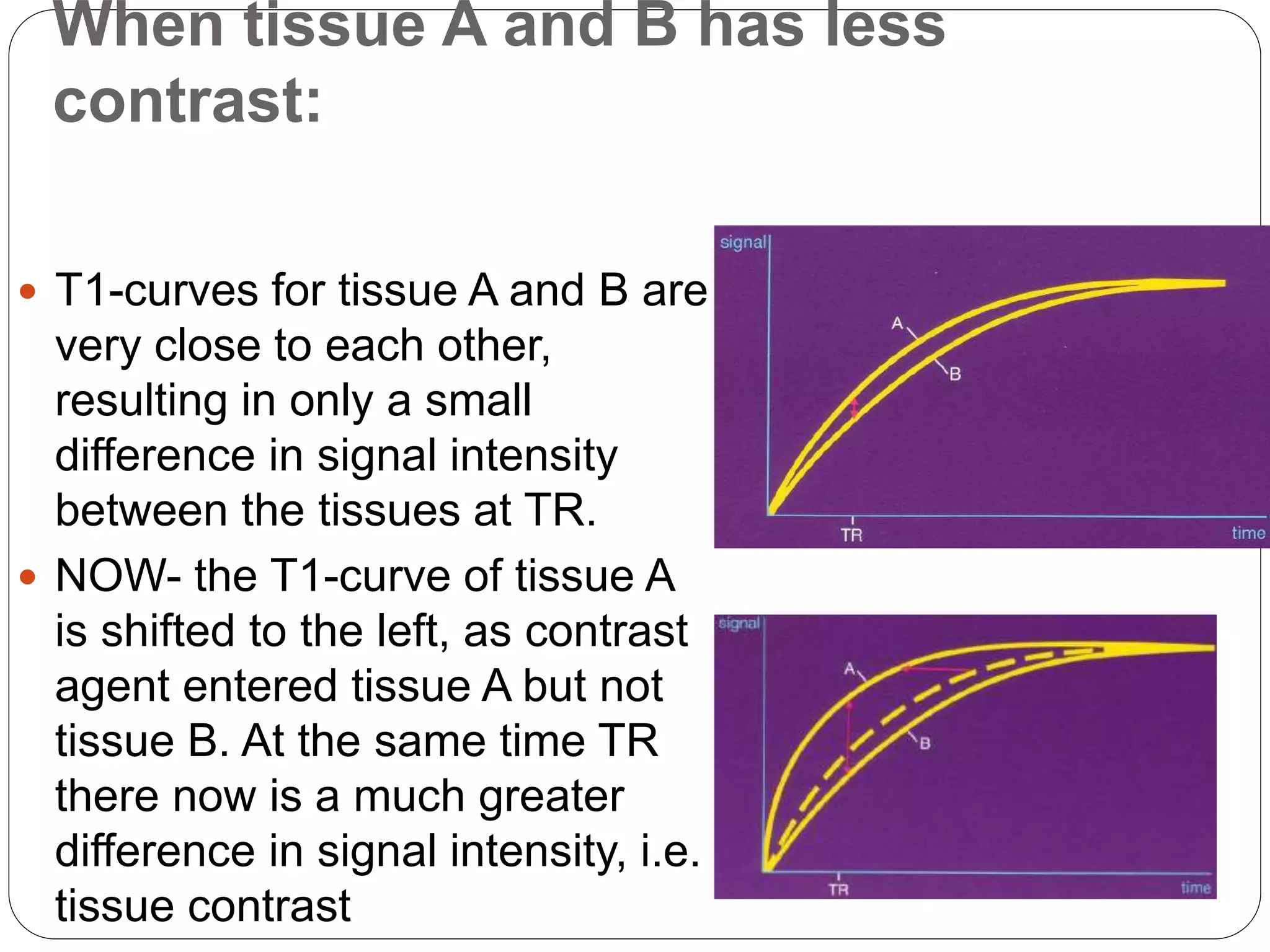
Explains TE and TR timings in MRI, how they affect signal intensity across different tissues with varying relaxation times.
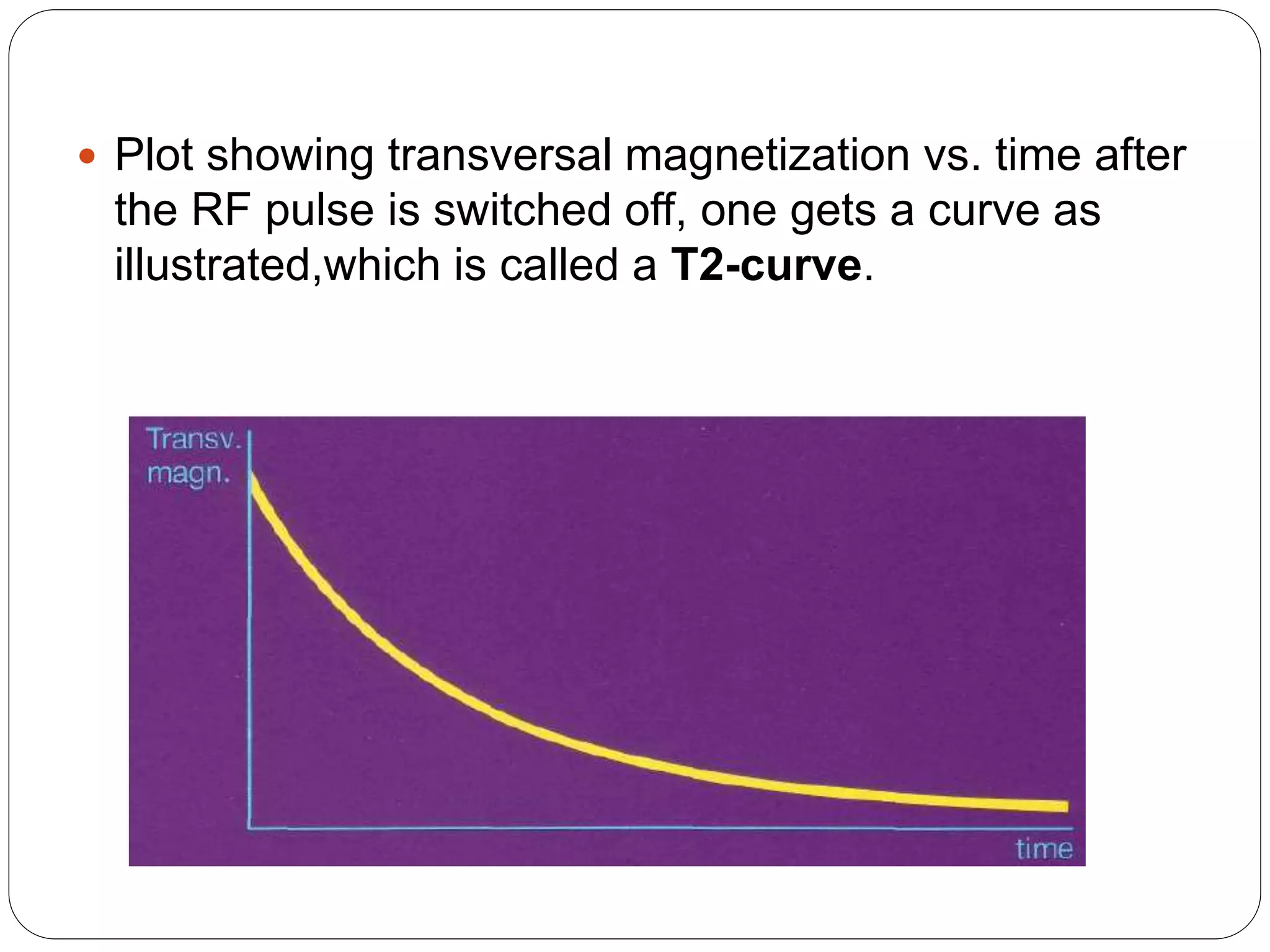
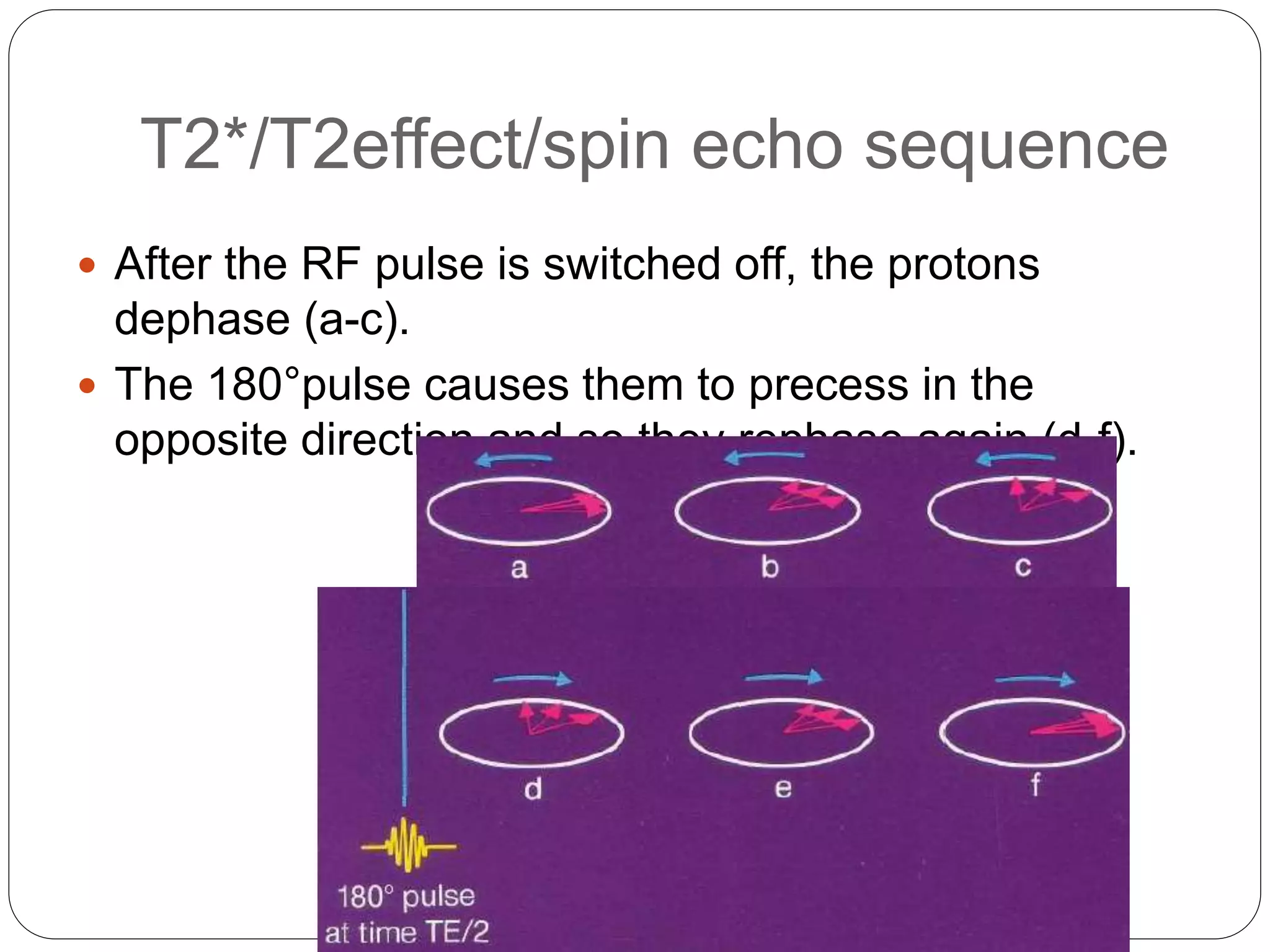
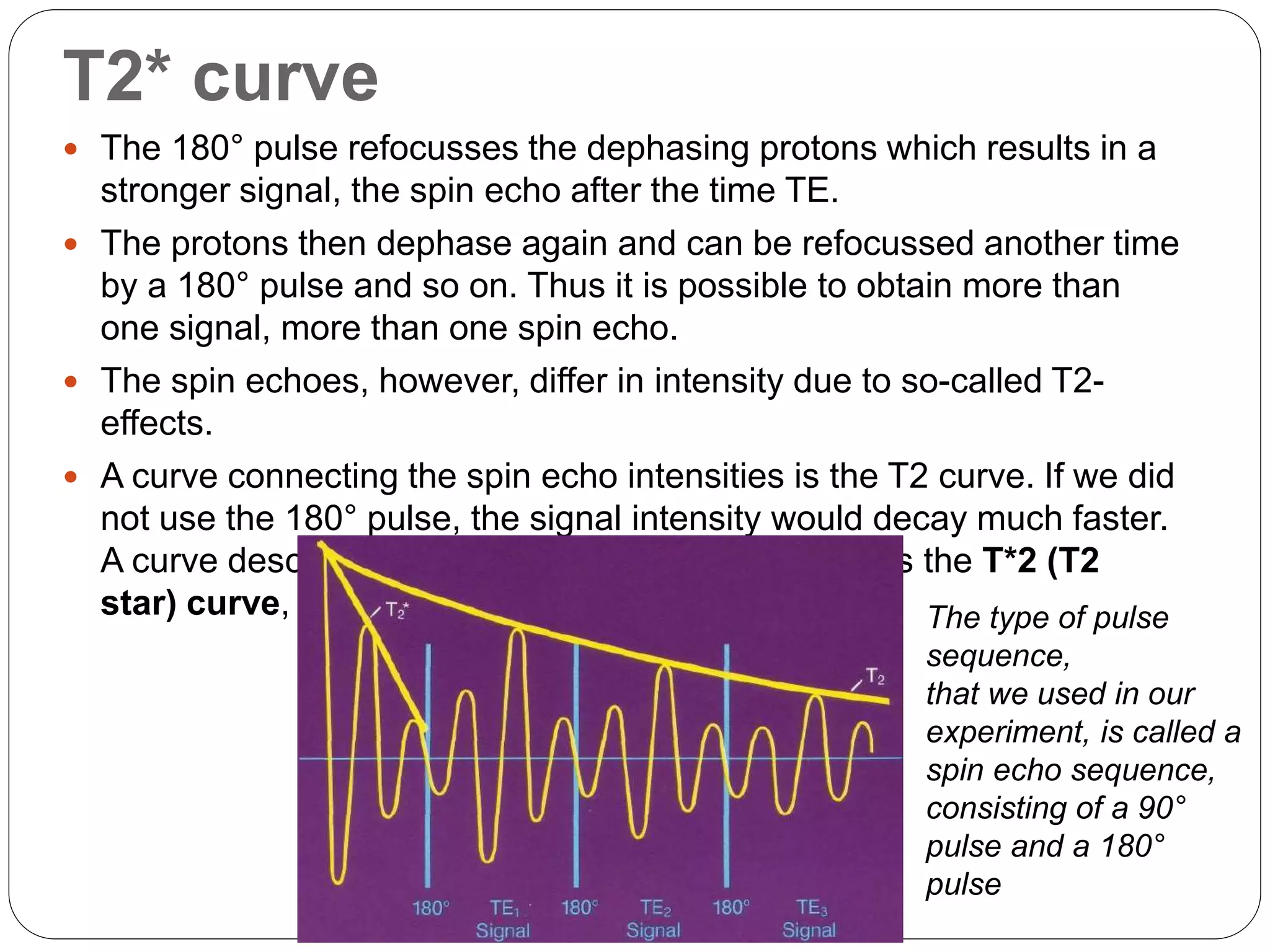
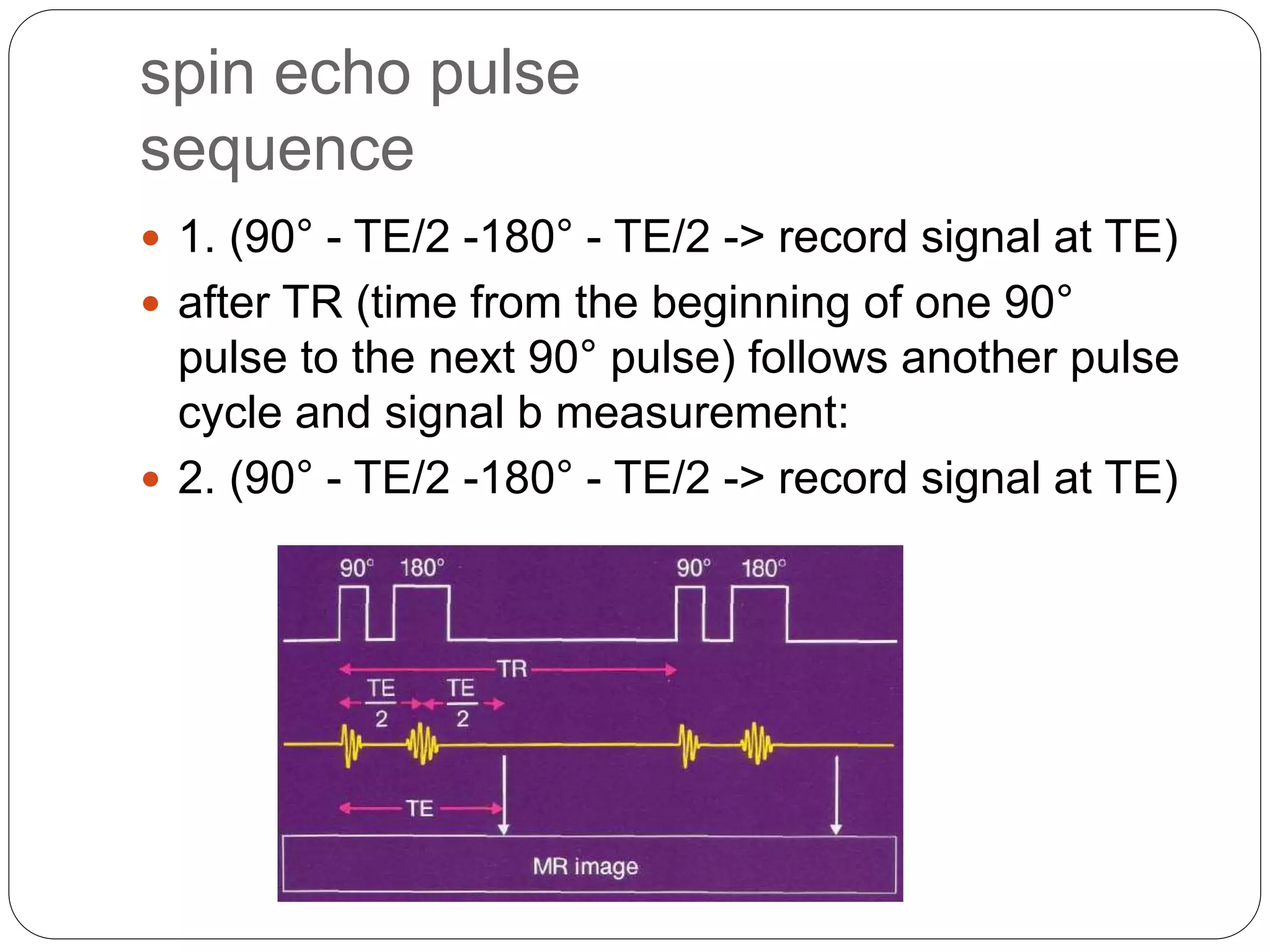
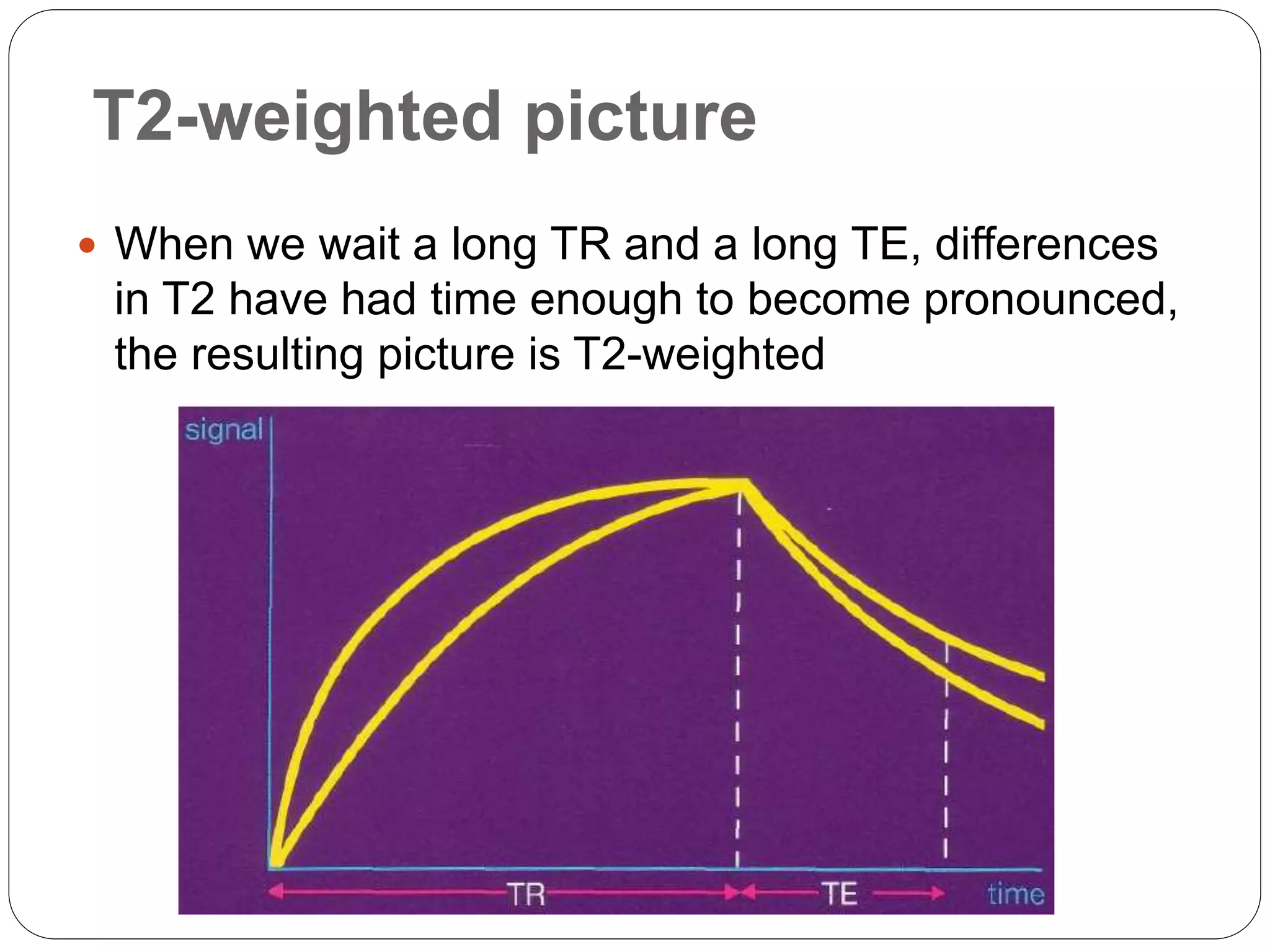
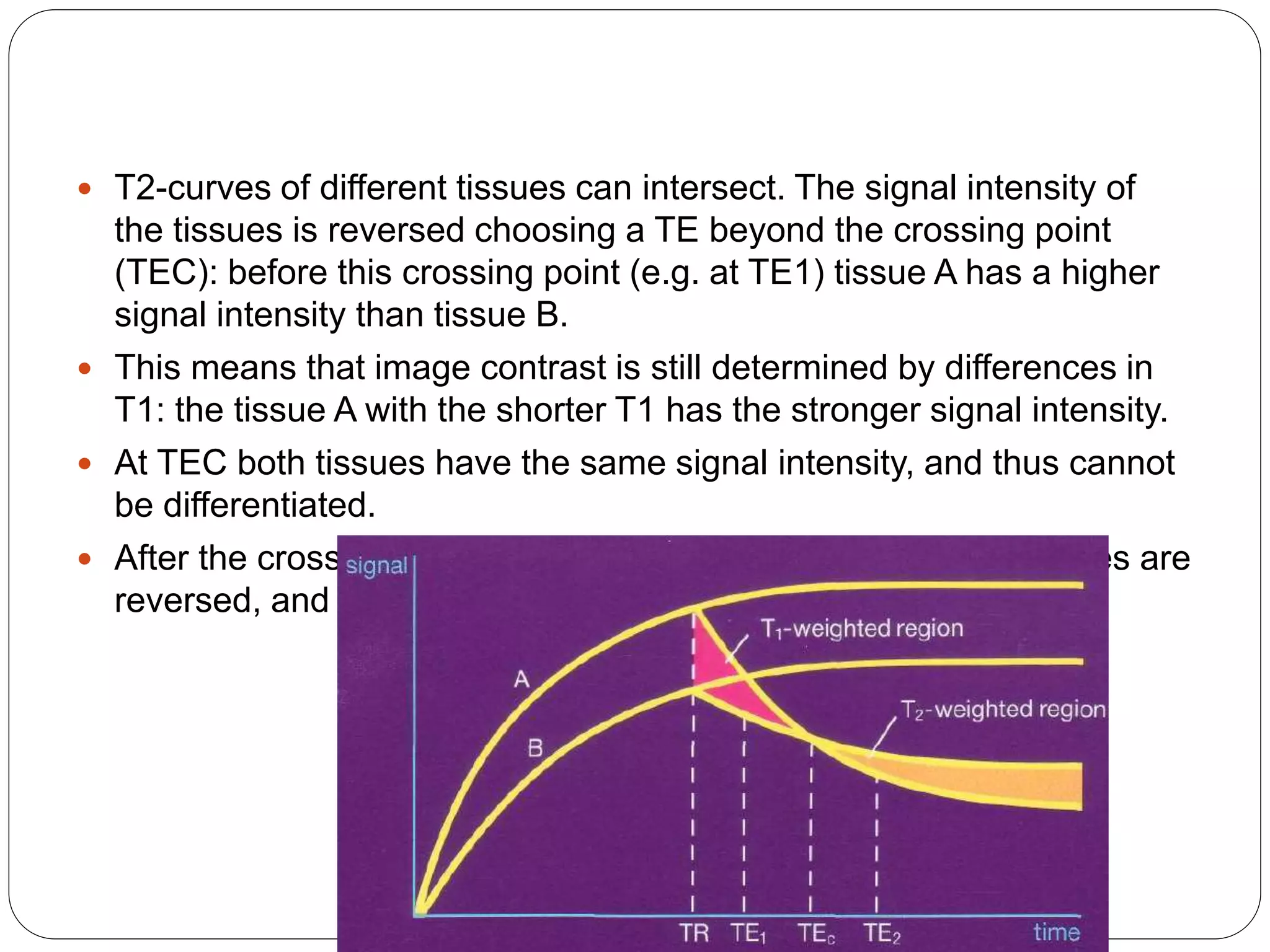
Discussion on T2-weighted images, emphasizing spin echo sequences and the significance of T2 curves in different tissues.
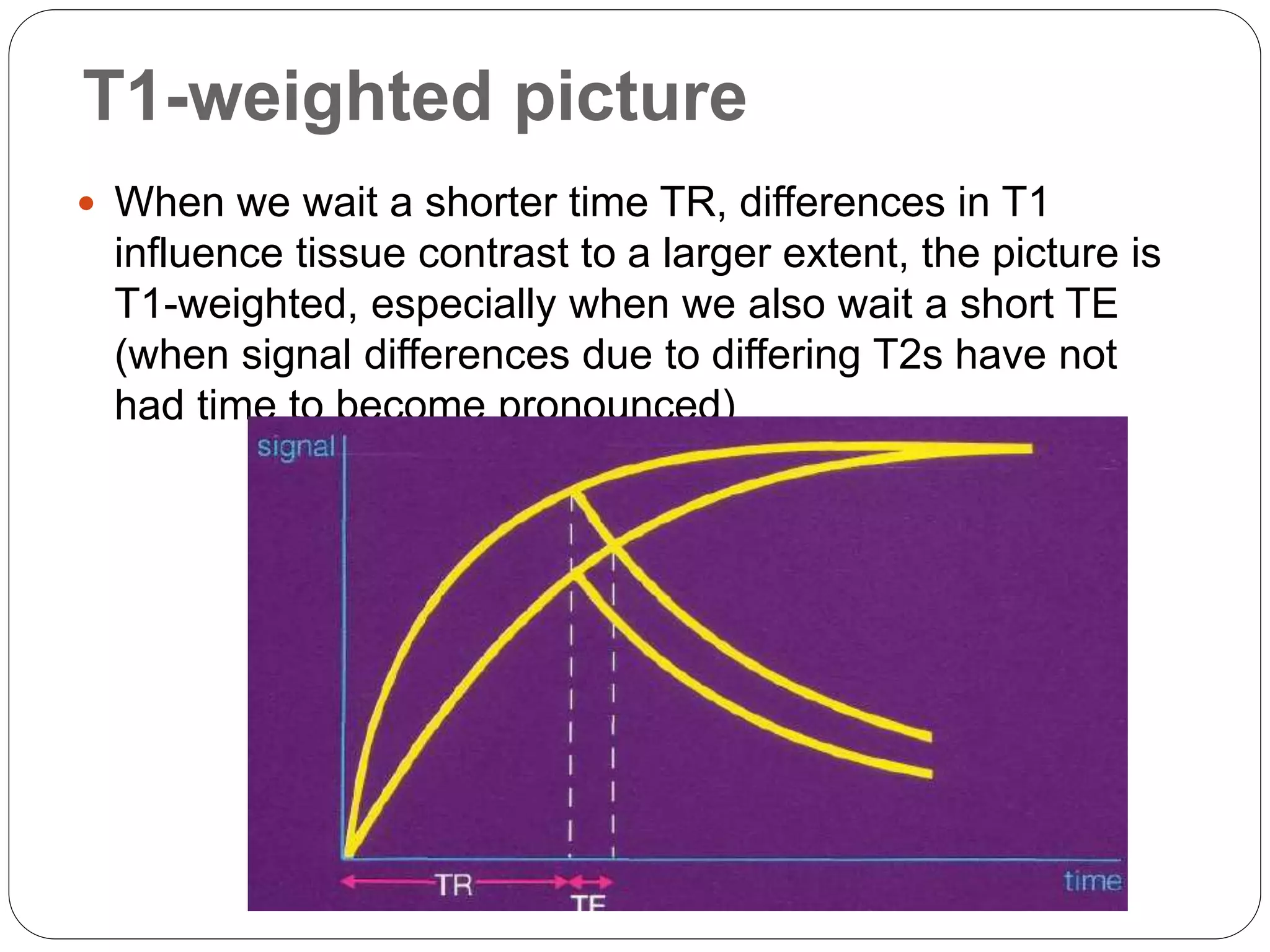
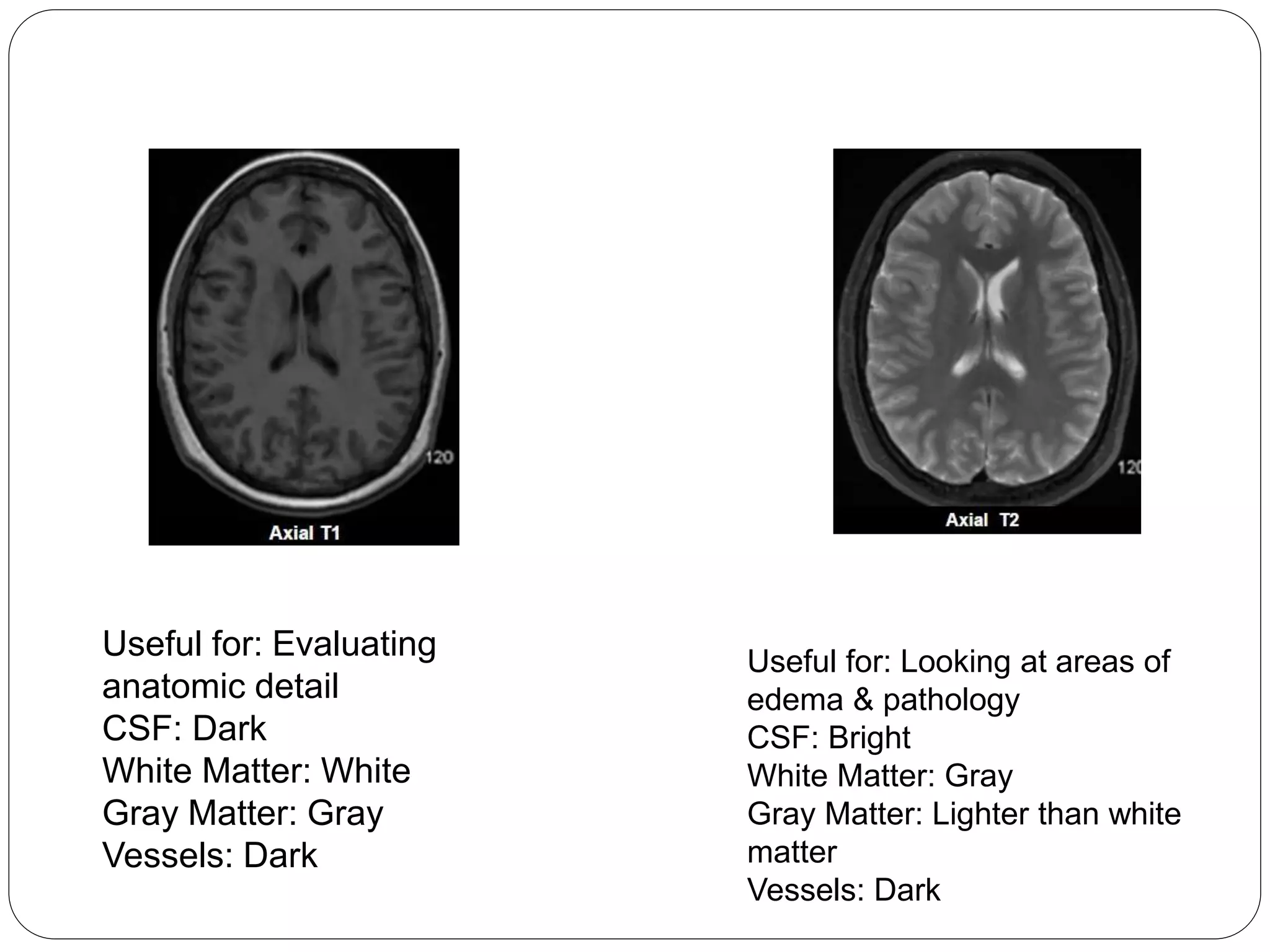
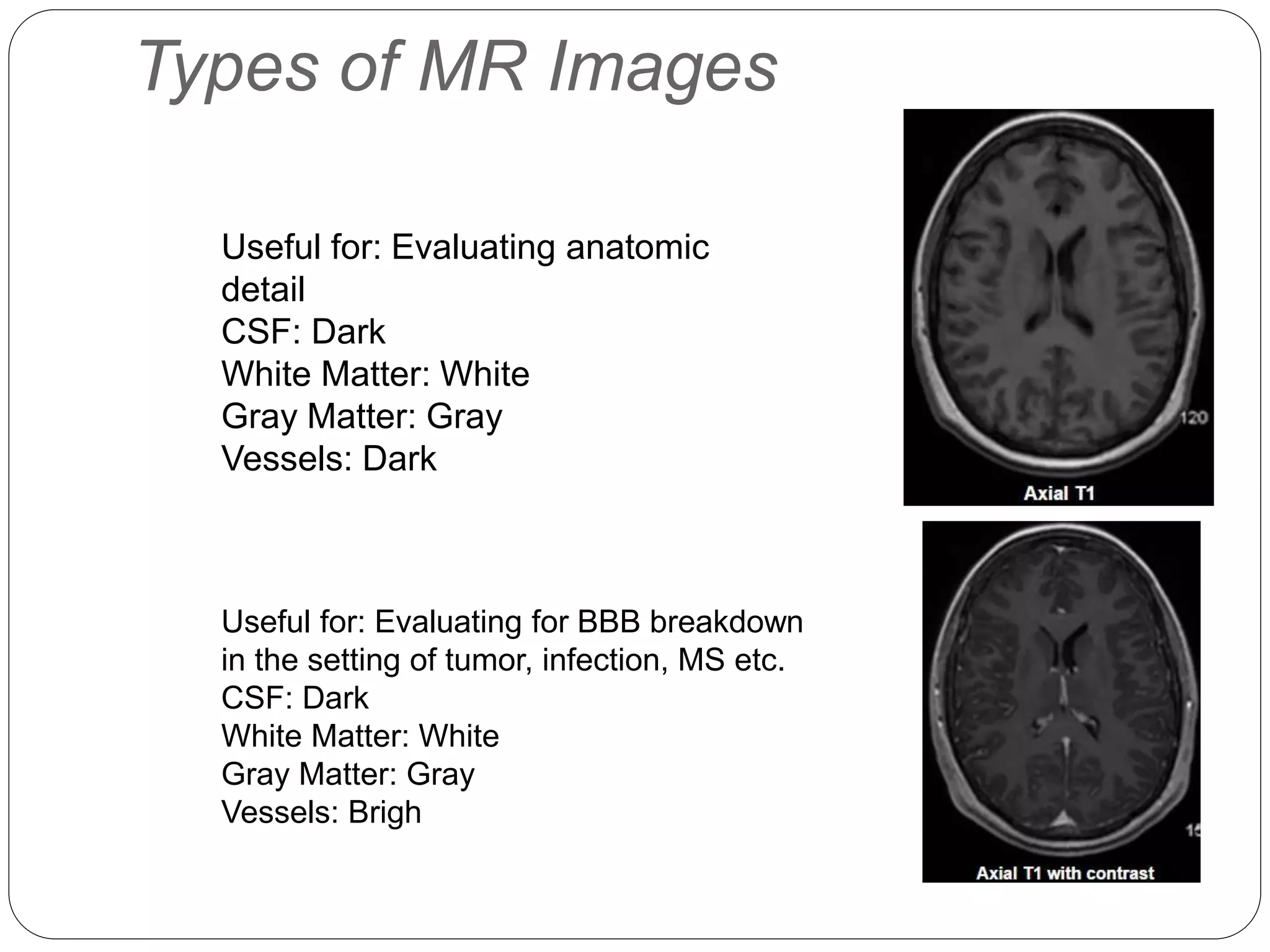
Definitions of short vs long TR/TE, effects on T1-weighted and T2-weighted imaging contrasts, including tissue appearance.
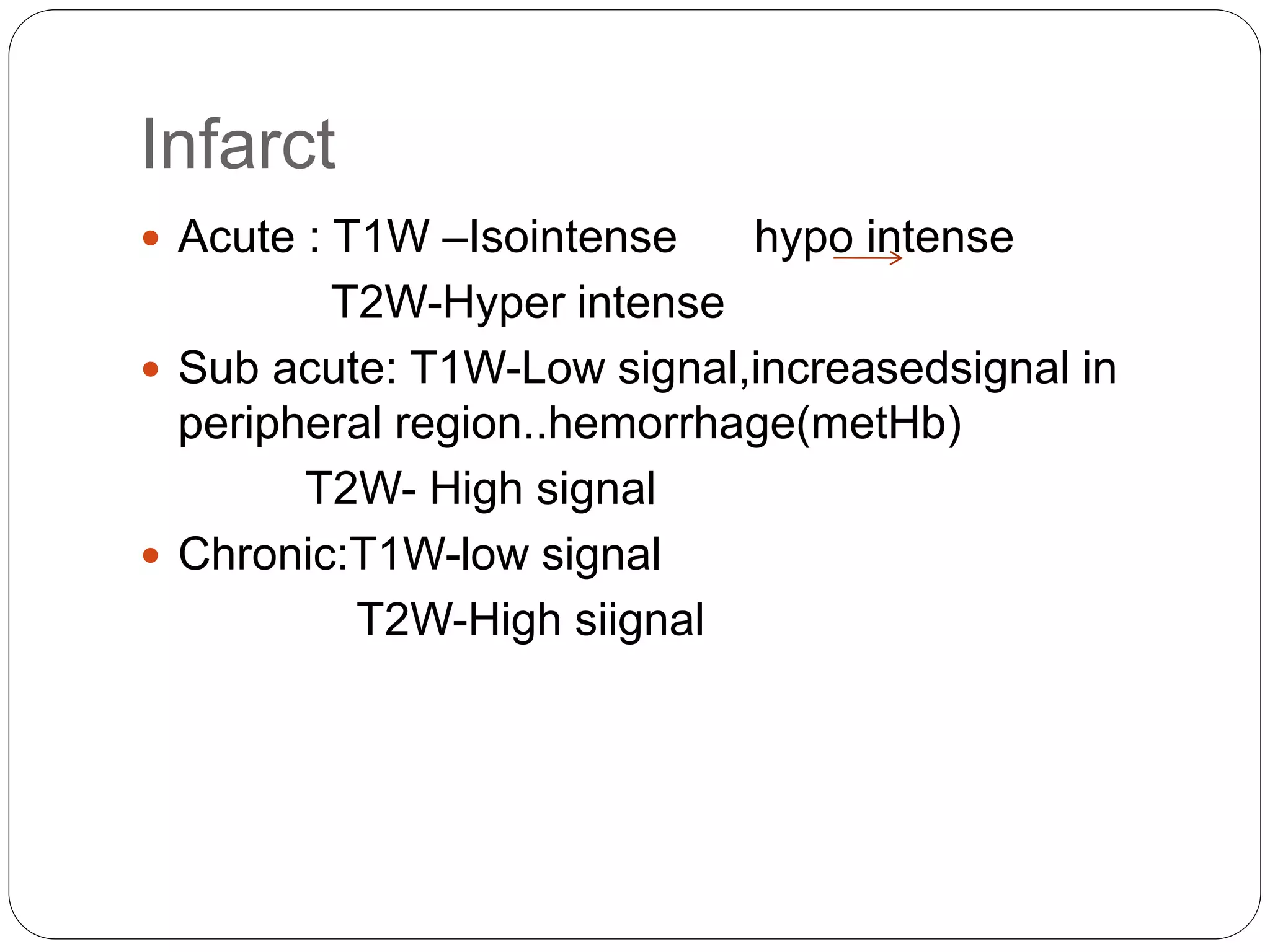
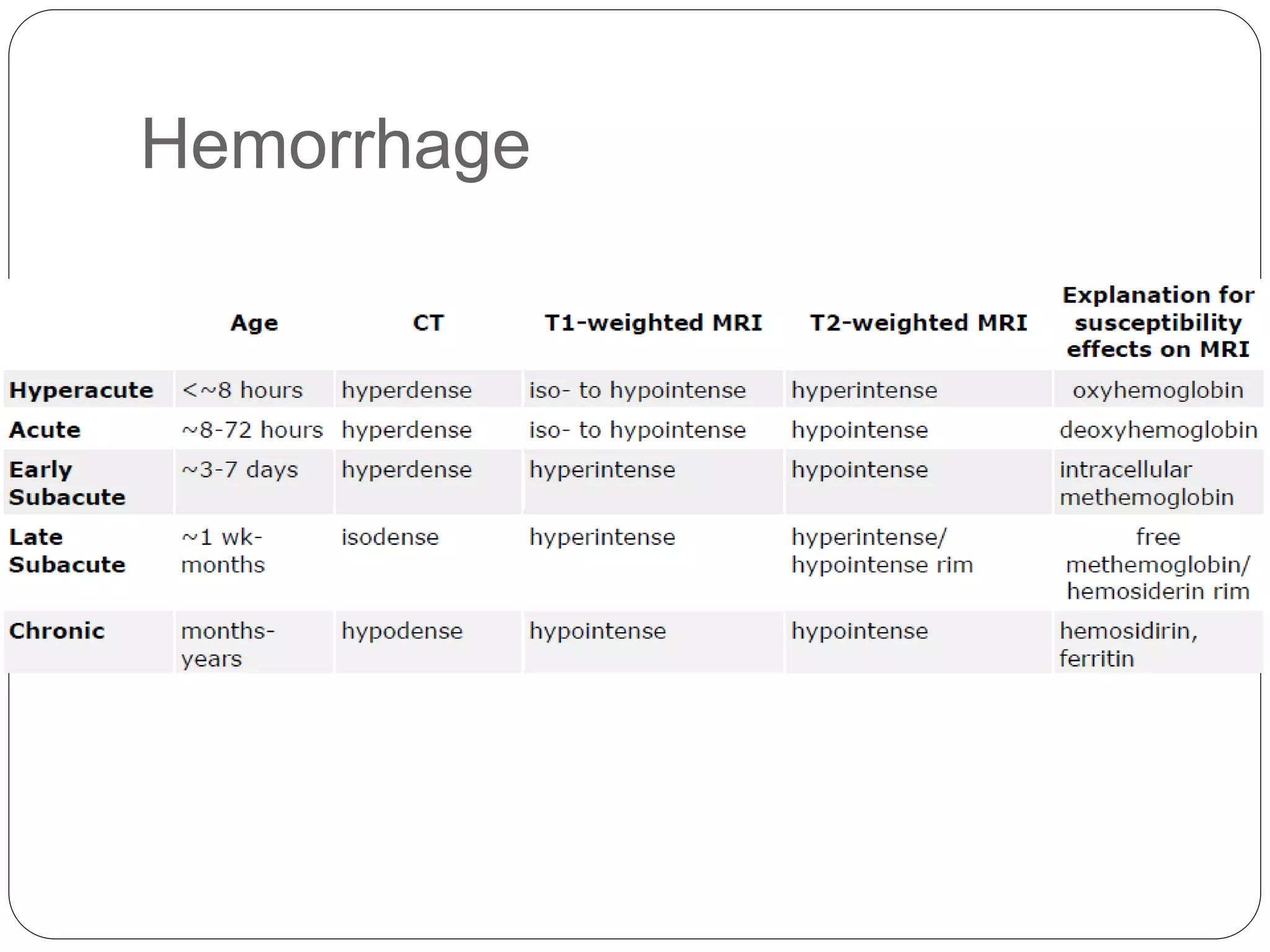
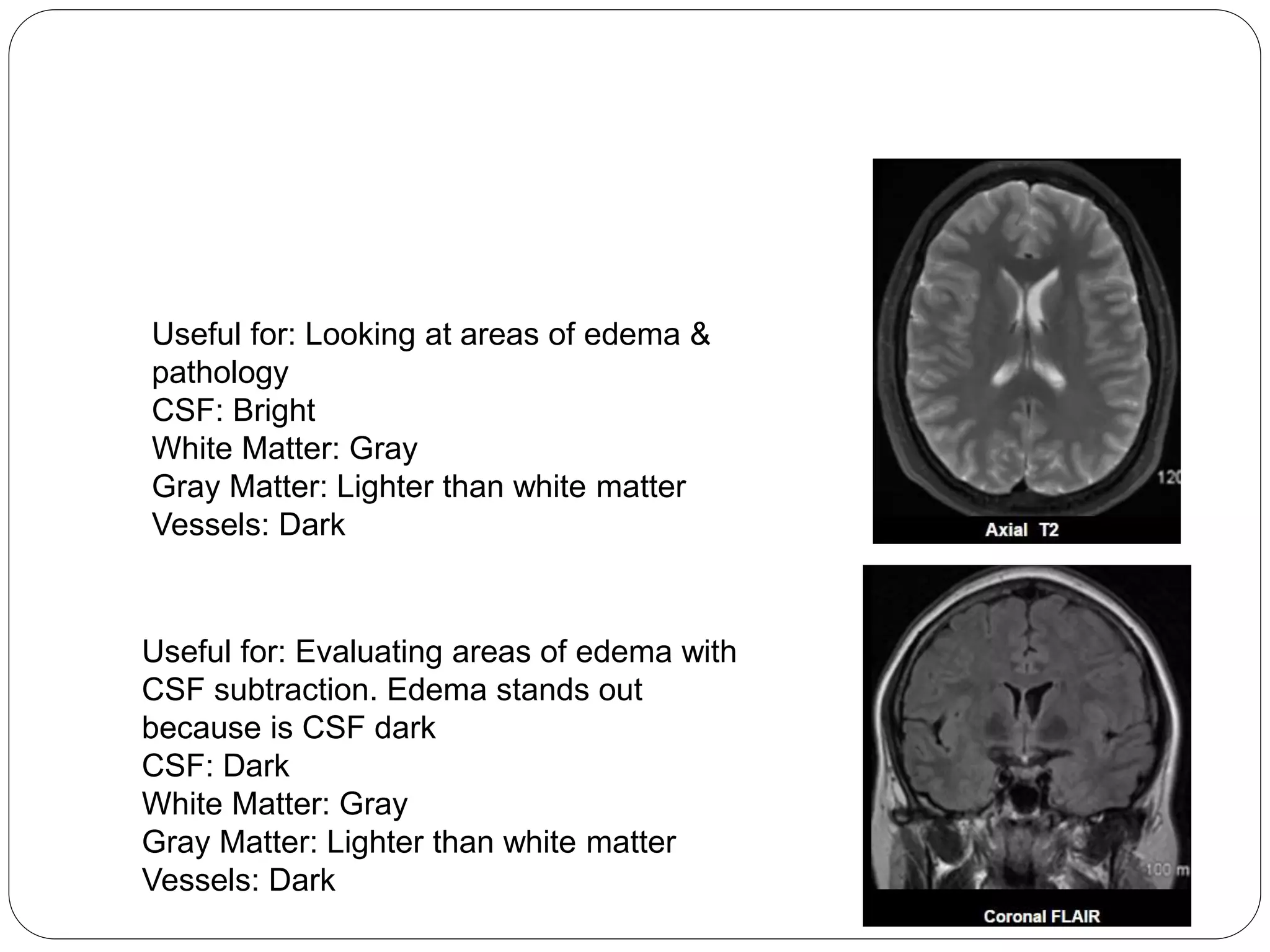
Details on bright/dark appearances for various tissues in T1 and T2-weighted images, facilitating the diagnosis of conditions.
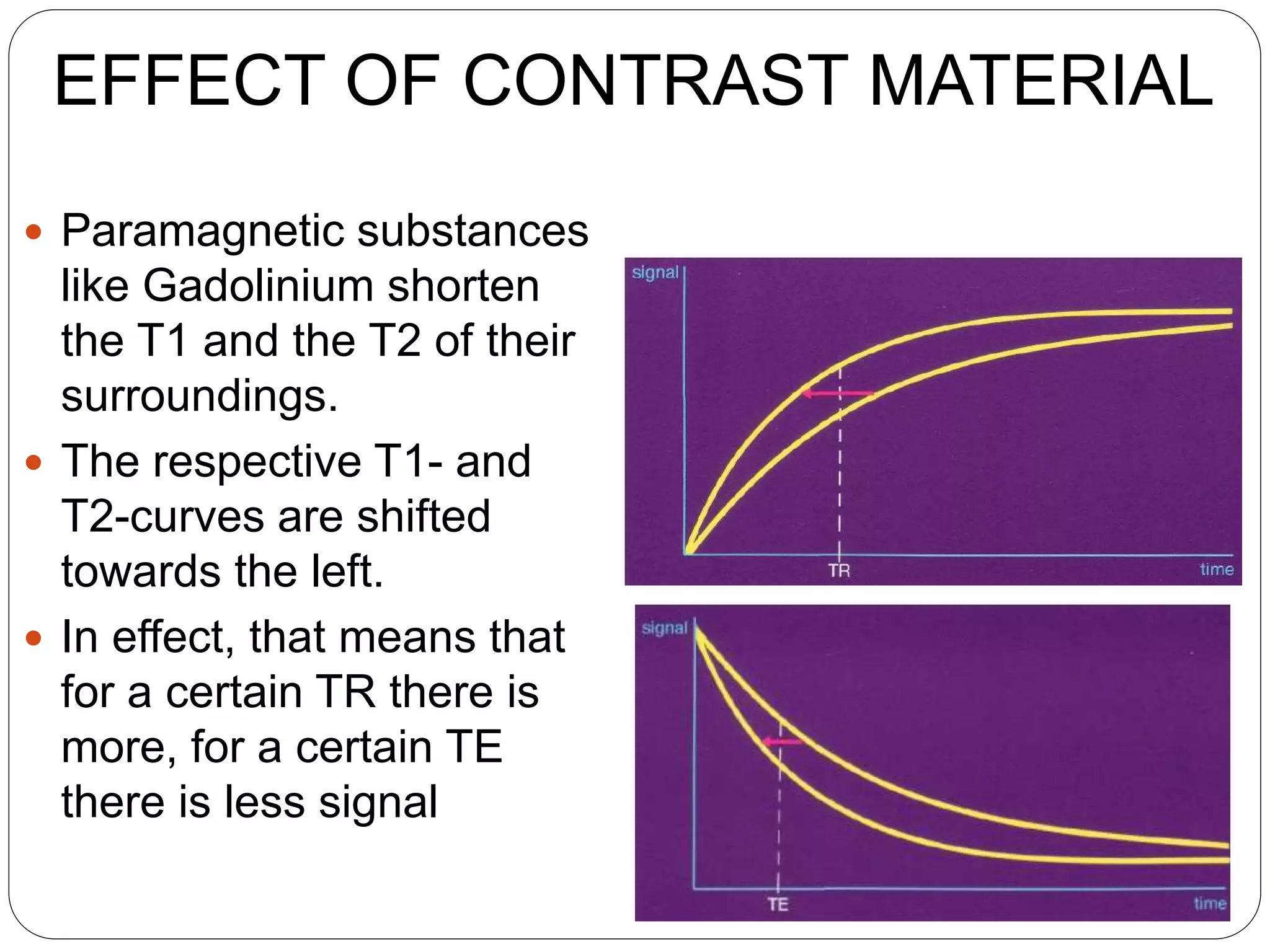
Differentiating various conditions using T1W and T2W images, including details about injury characteristics and contrast material effects.
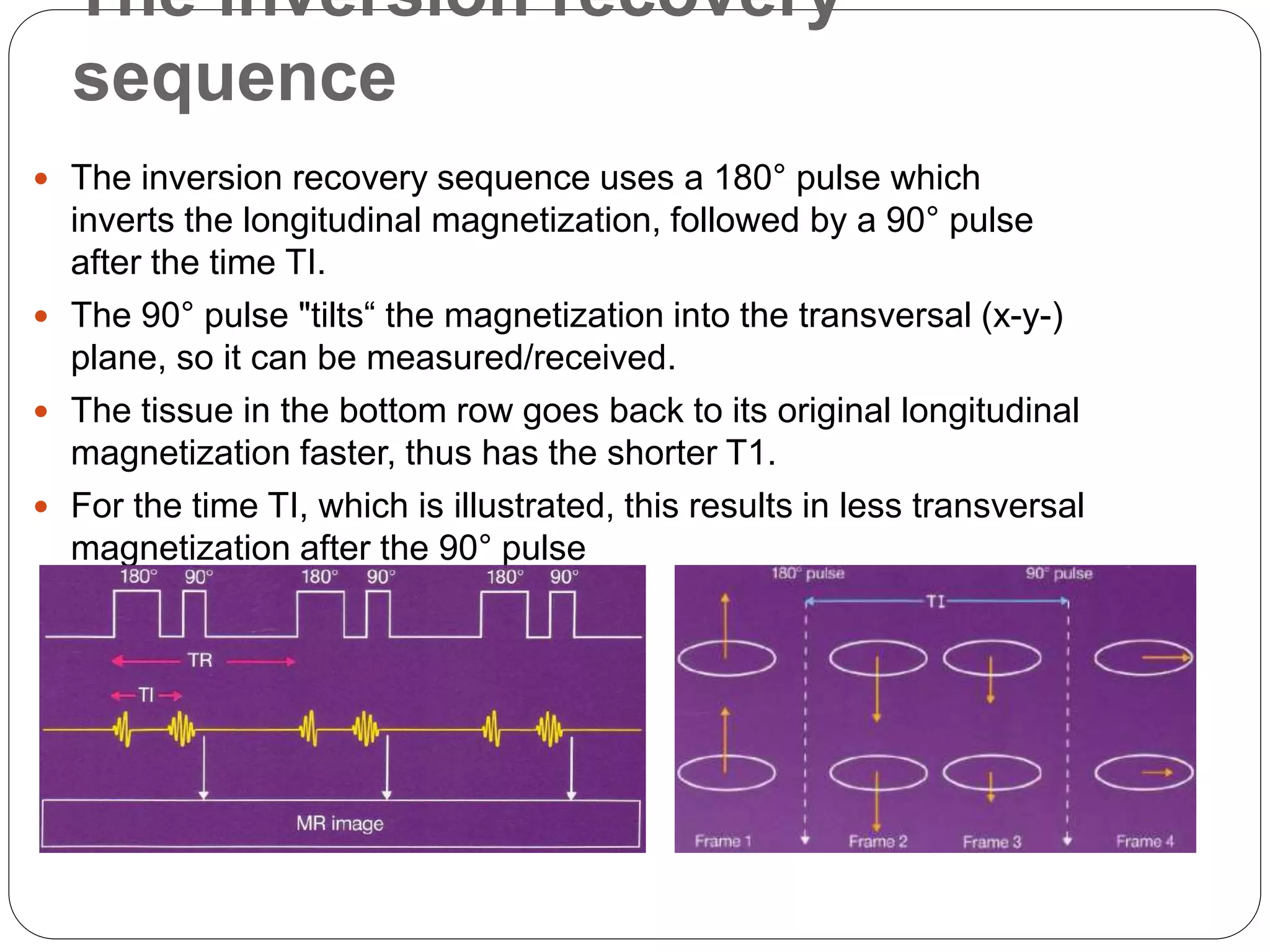
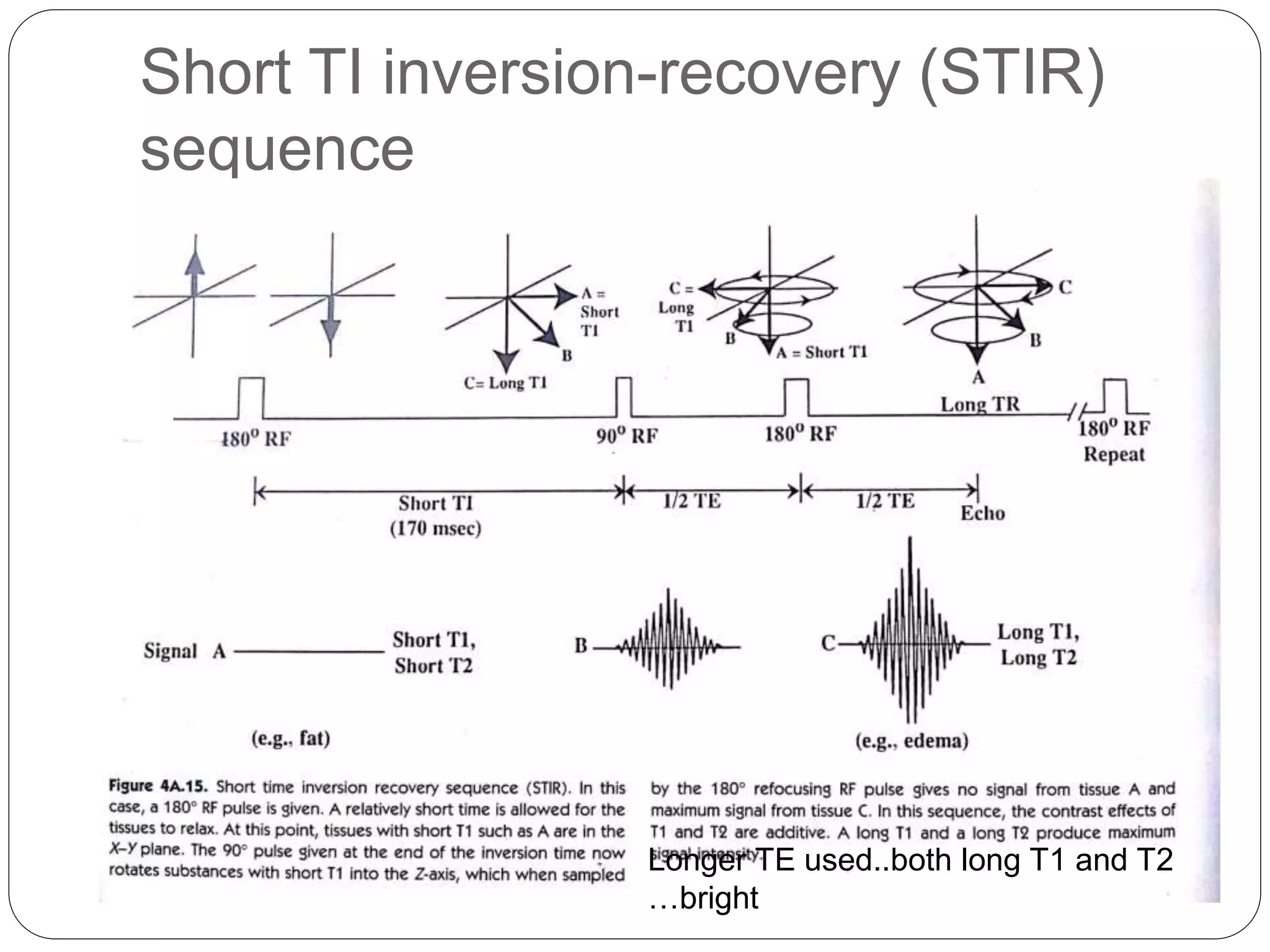
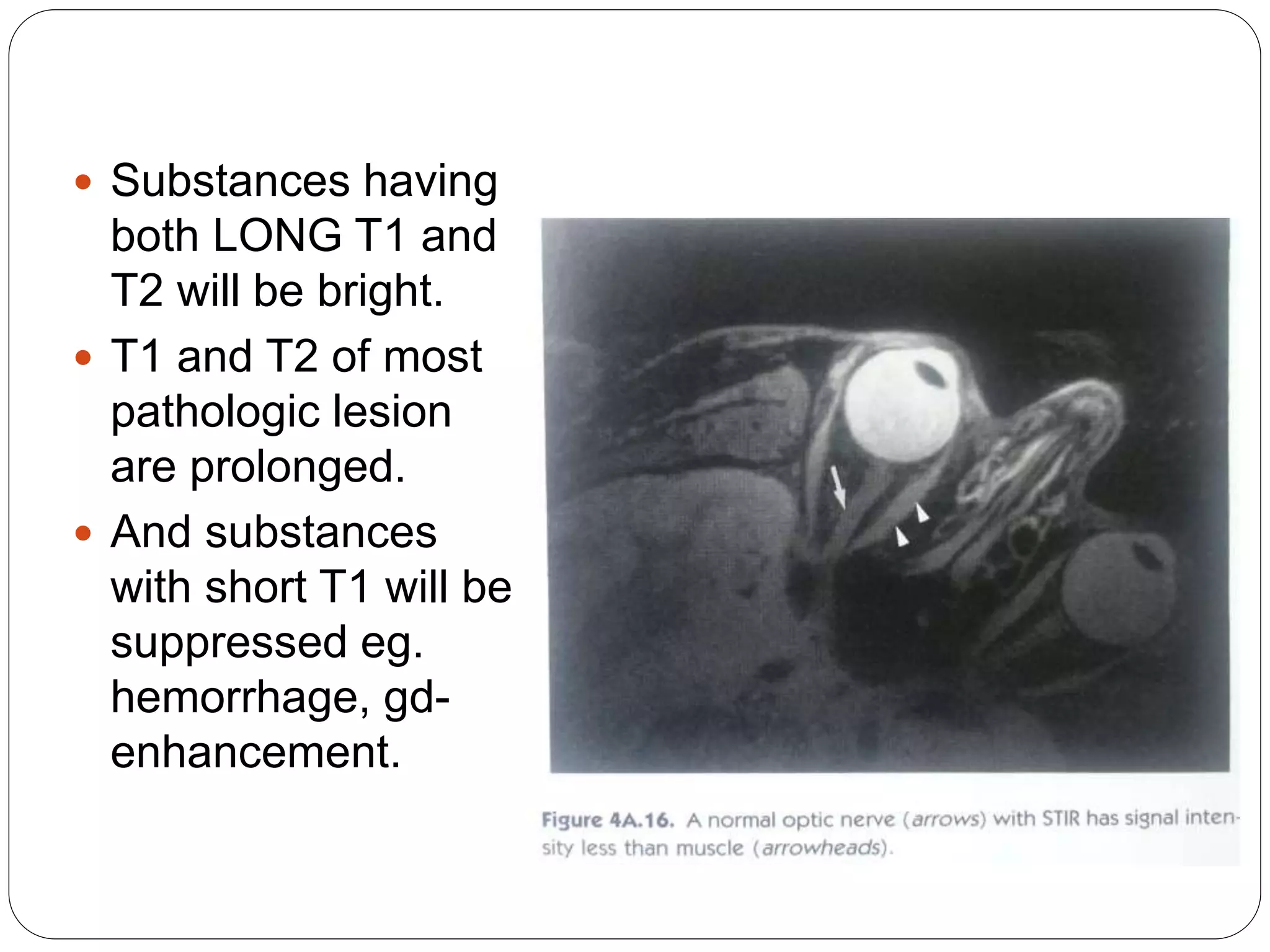
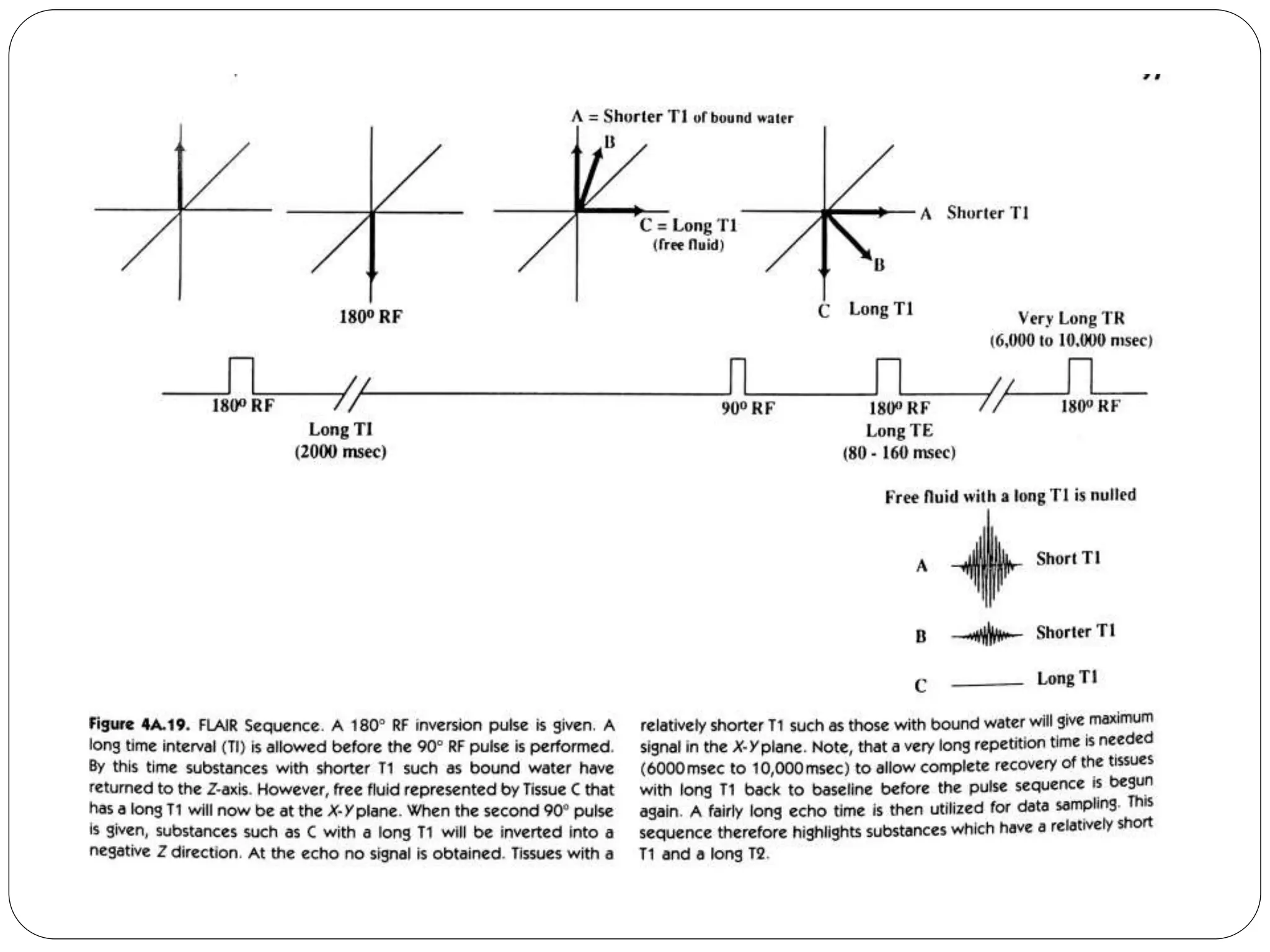
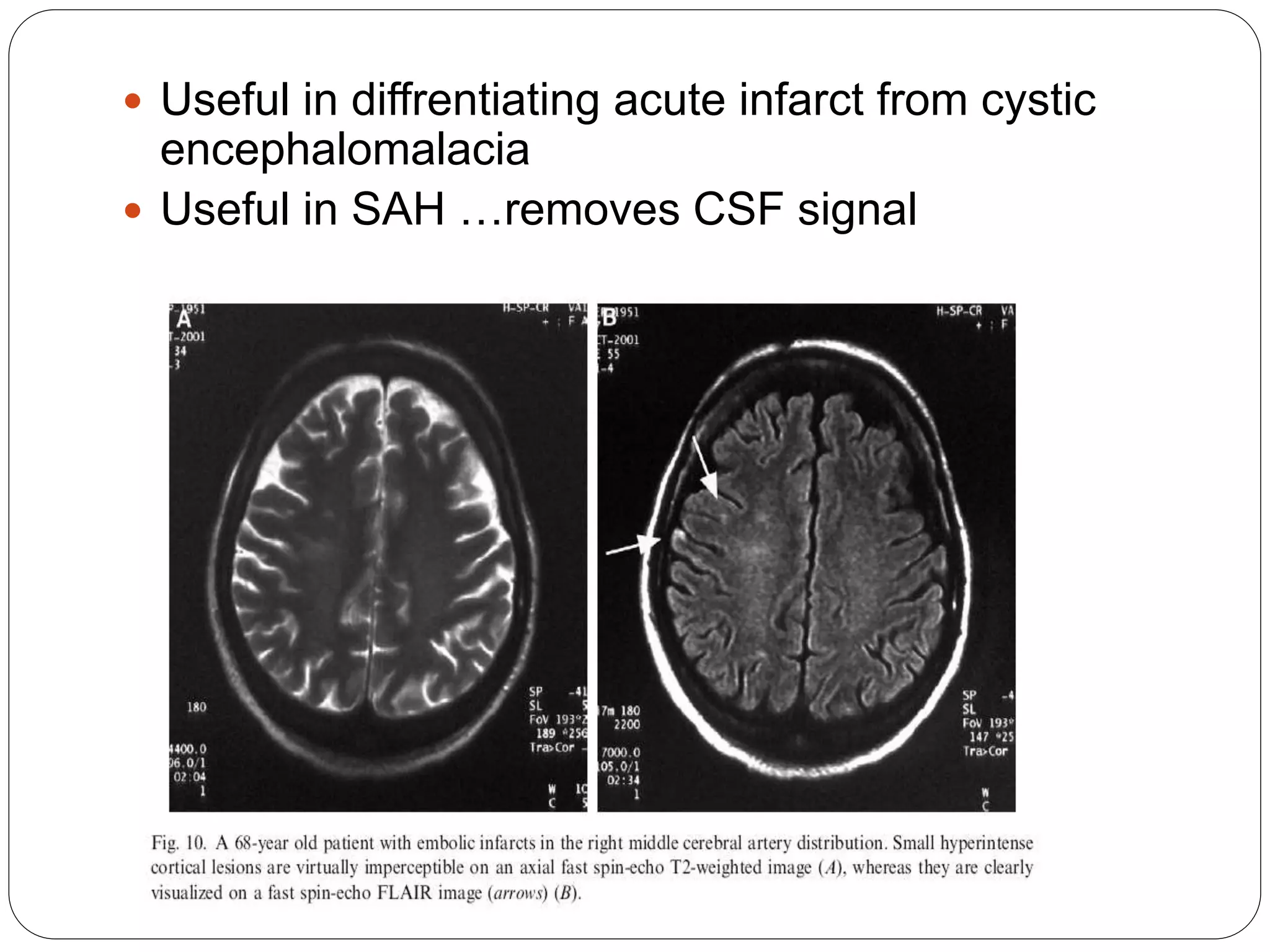
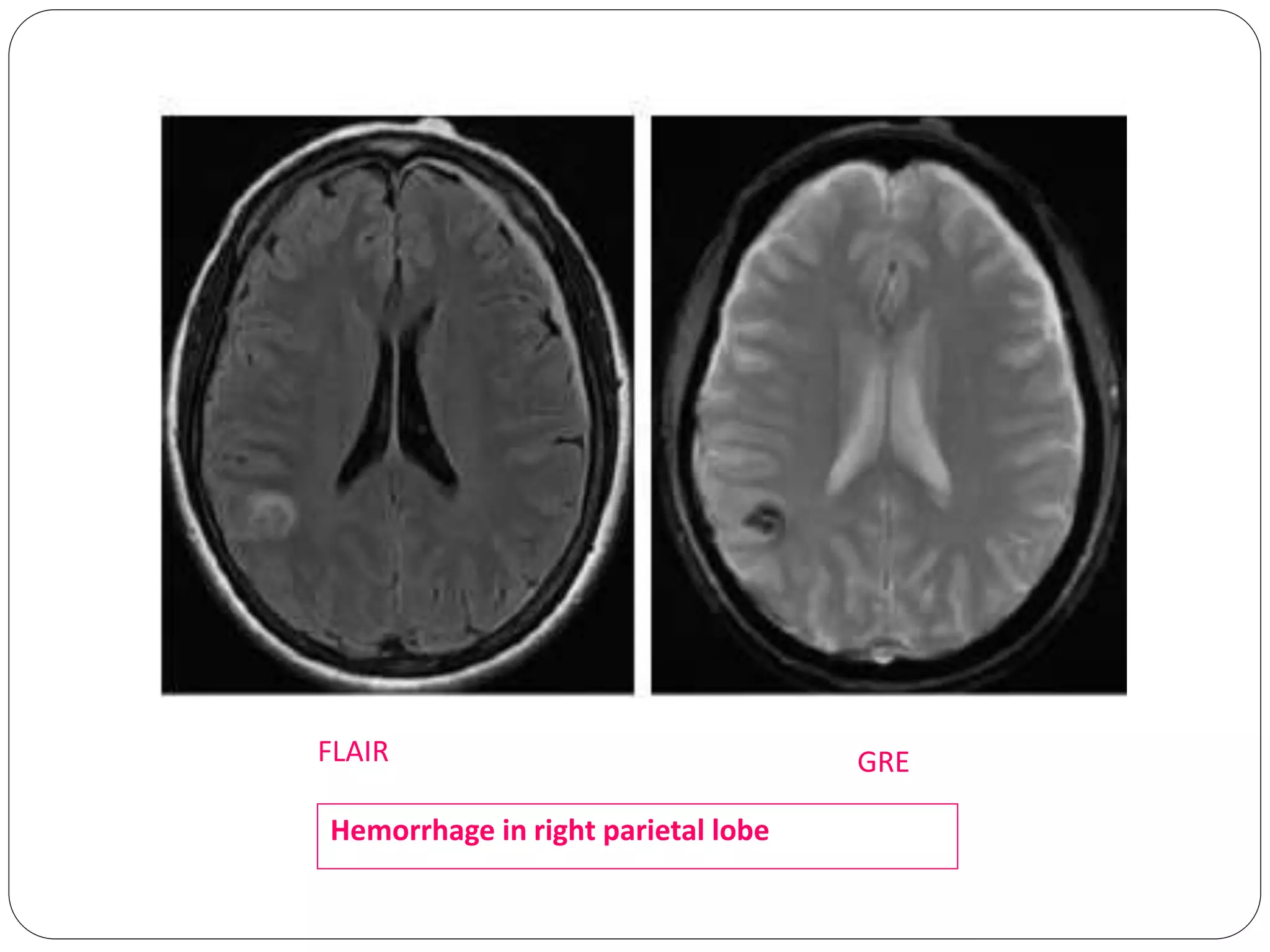
In-depth look at inversion recovery sequences, including STIR and FLAIR, and their applications in brain pathology.
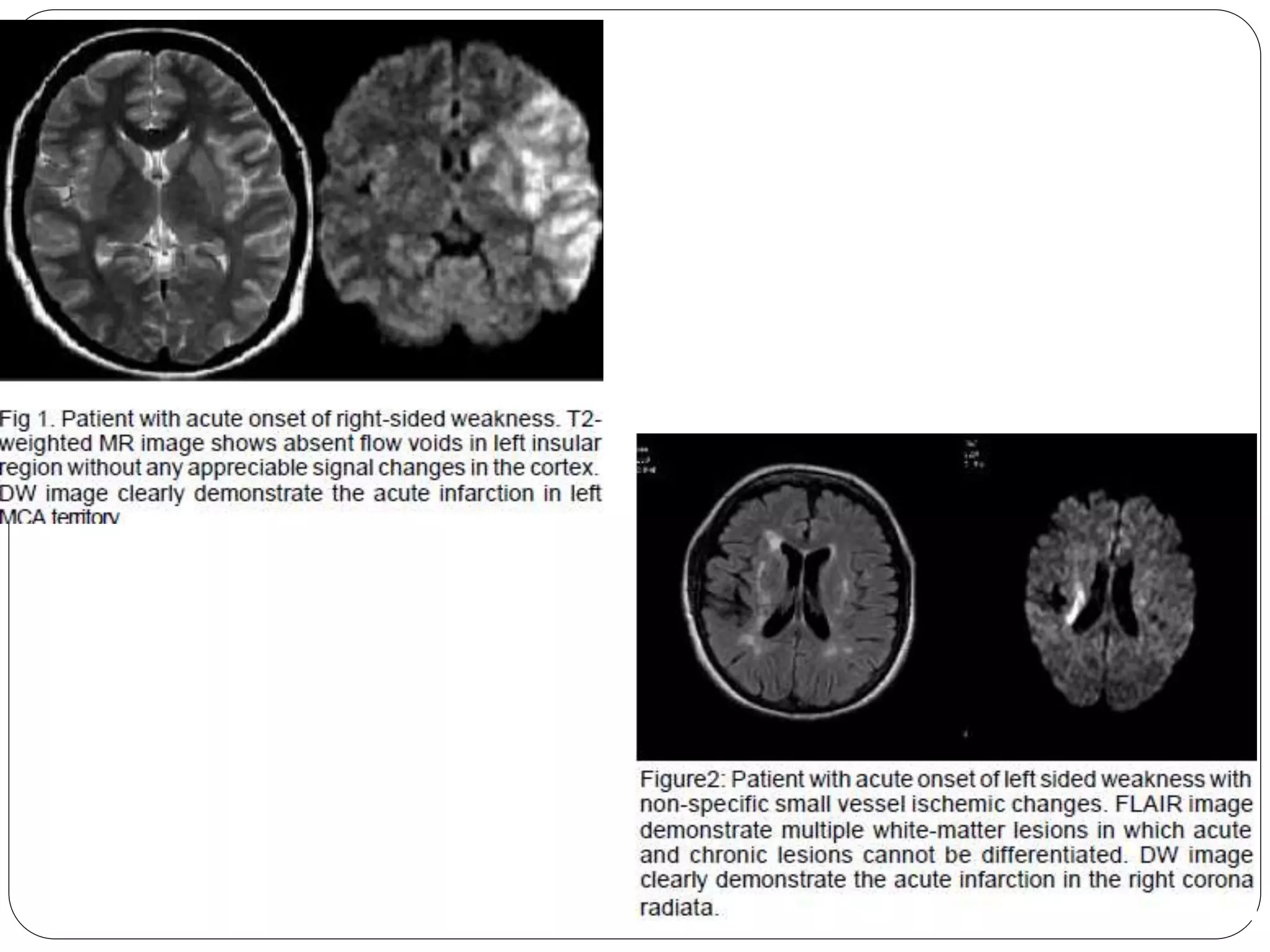
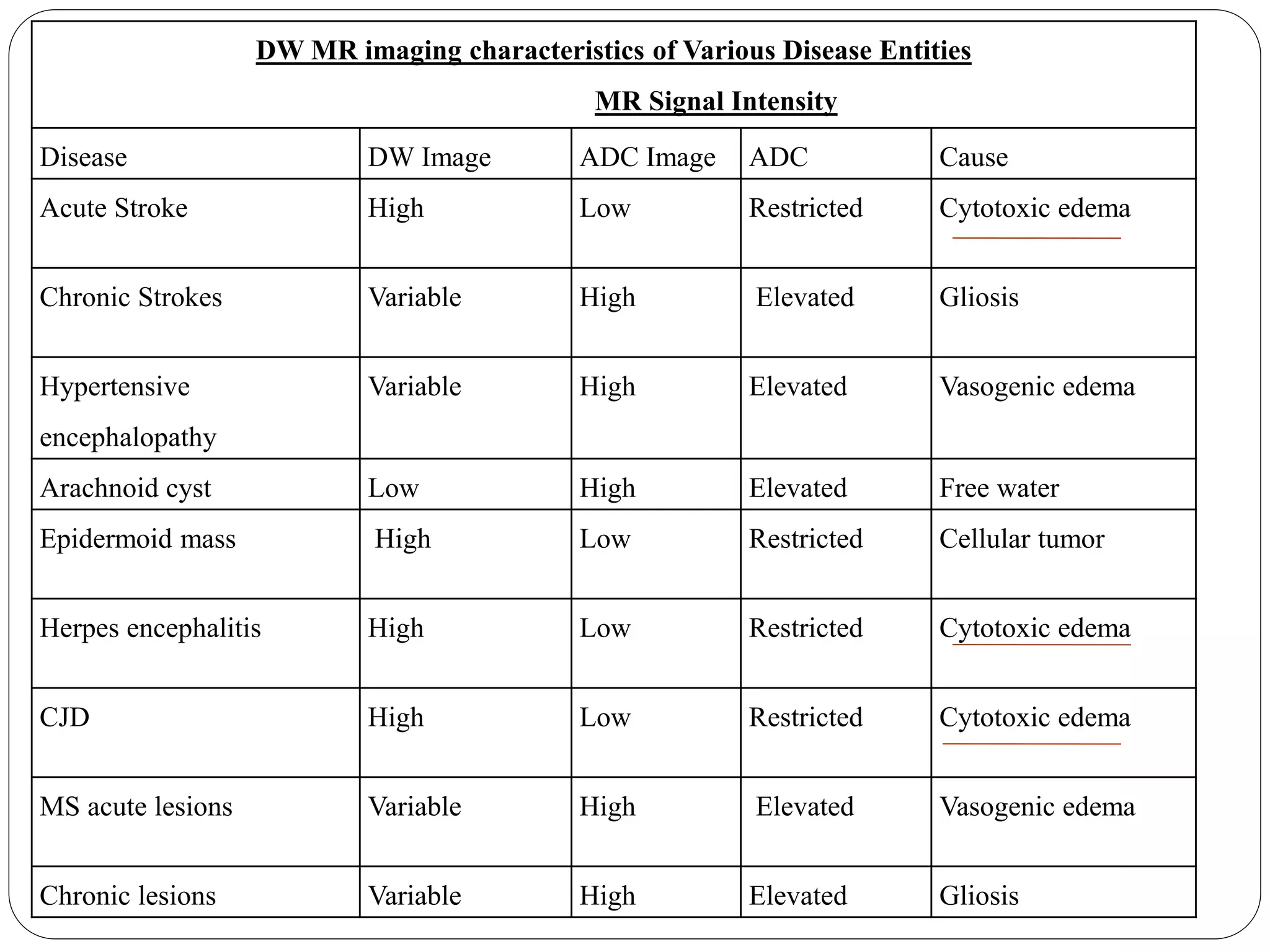
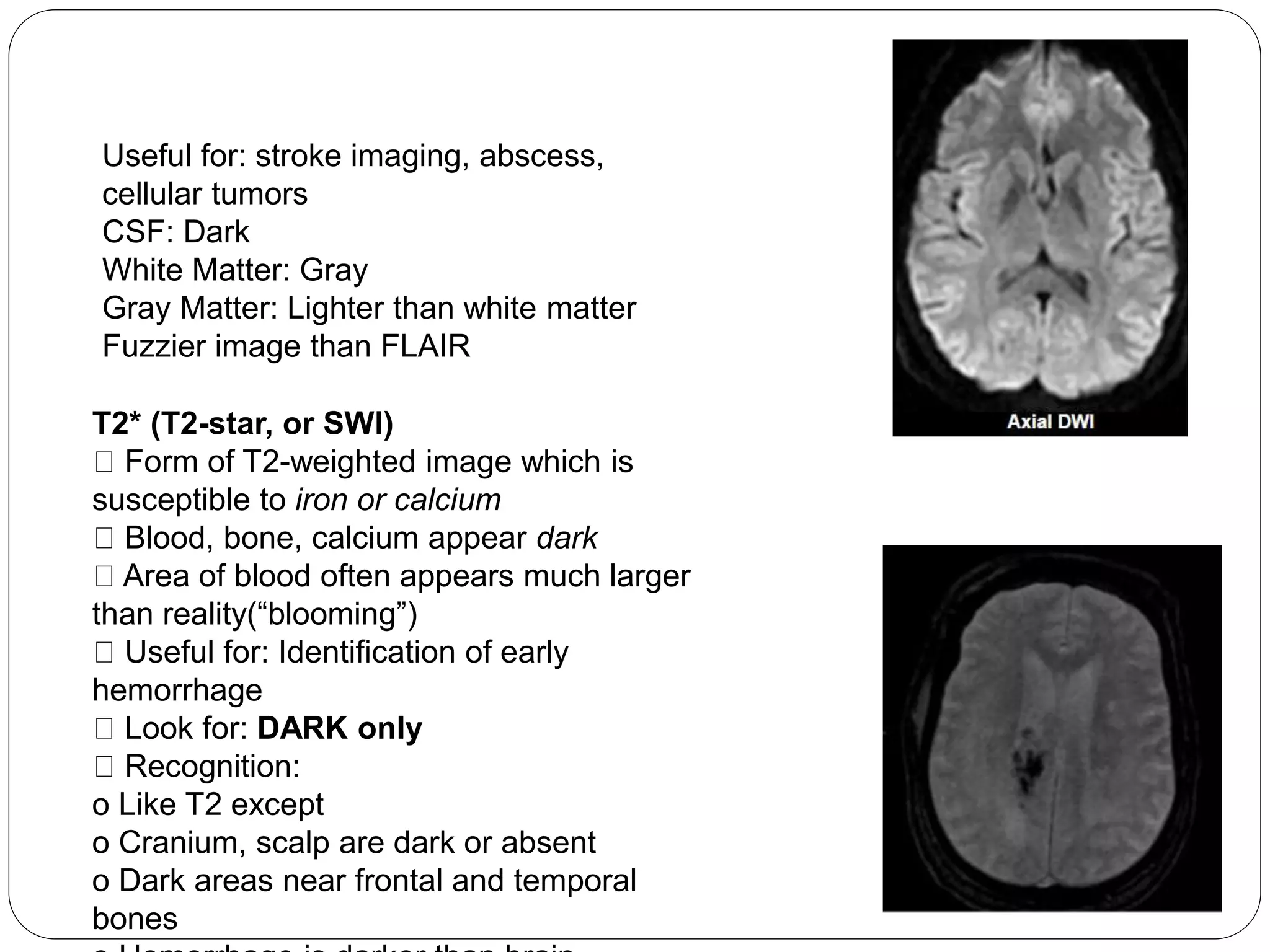
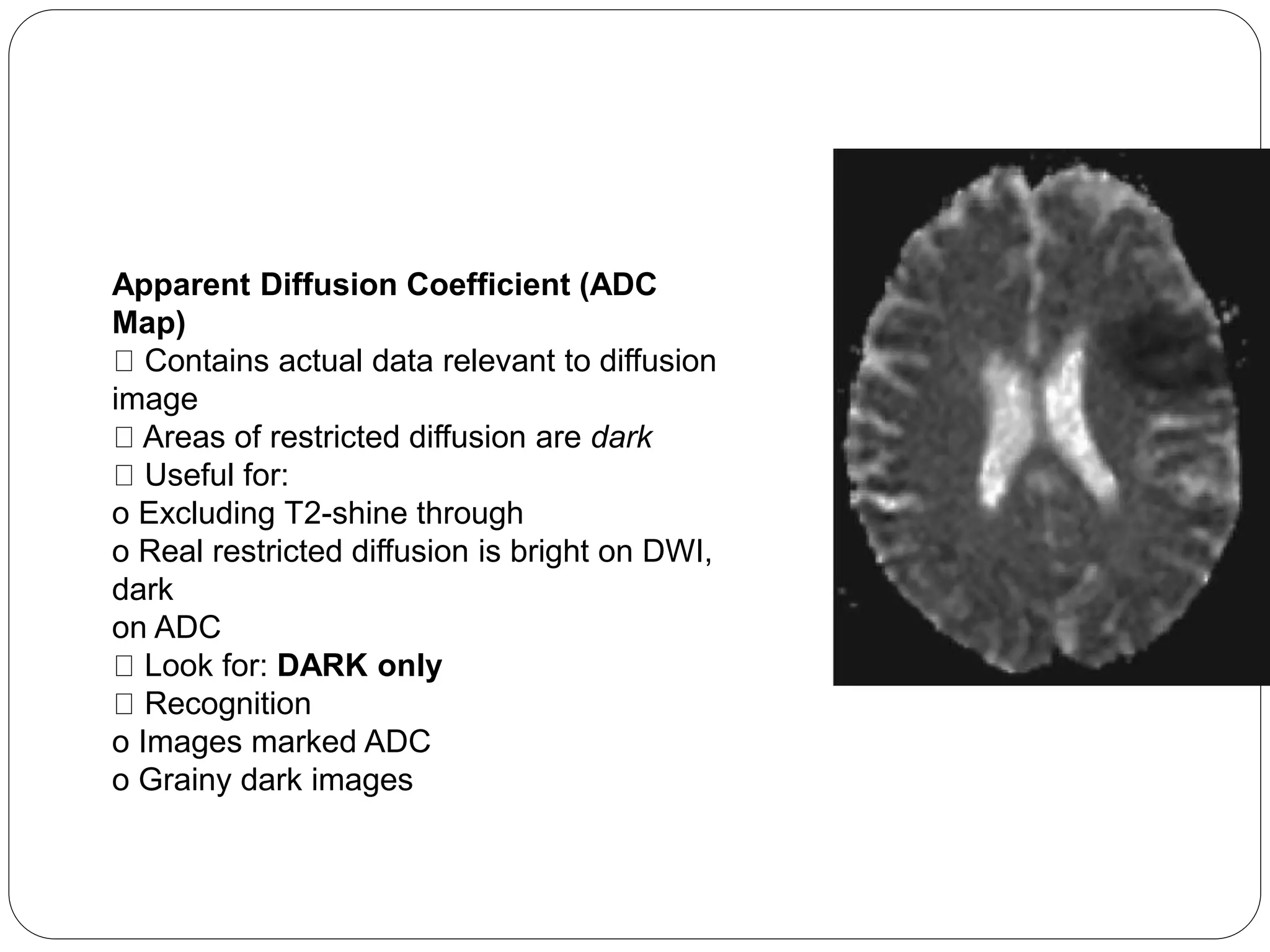
Explains diffusion-weighted MRI, ADC metrics, and their relevance for assessing acute stroke and differentiating lesions.
Evaluation metrics for stroke using DW imaging, significance of ADC in differentiating between acute and chronic lesions.
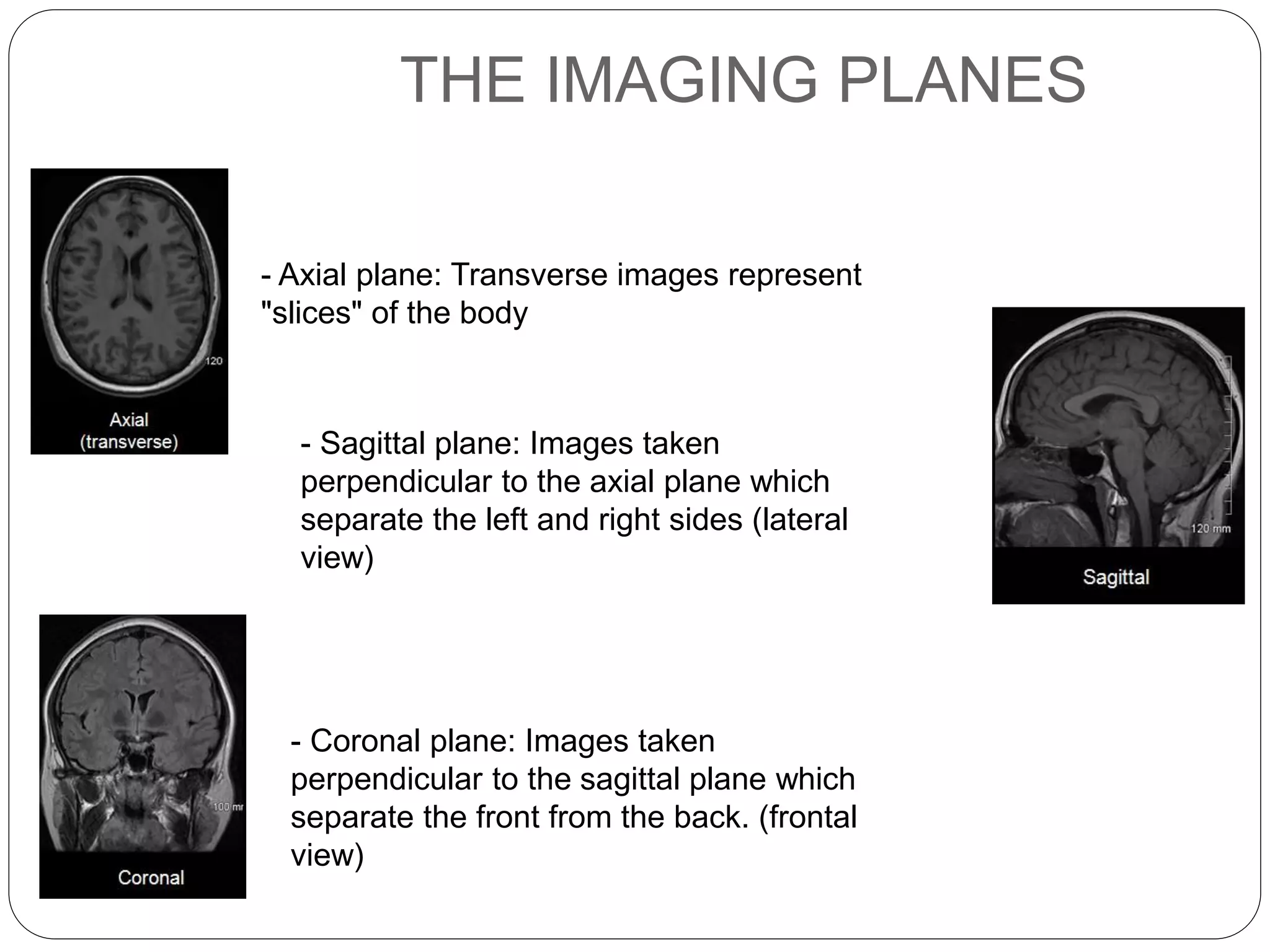
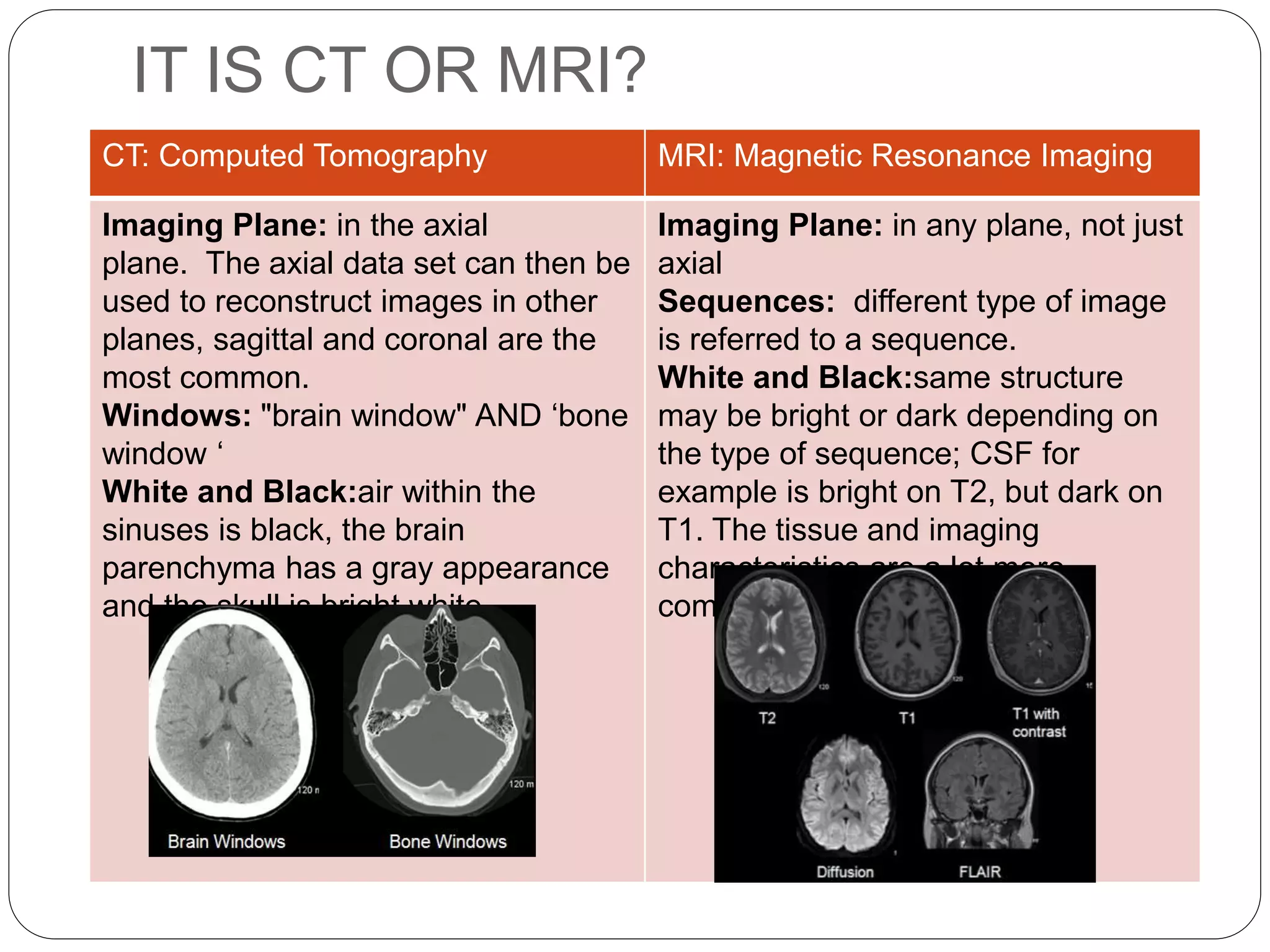
Description of MRI imaging planes, how to interpret MR images regarding hyperintensity and isointensity, and CT vs MRI differences.
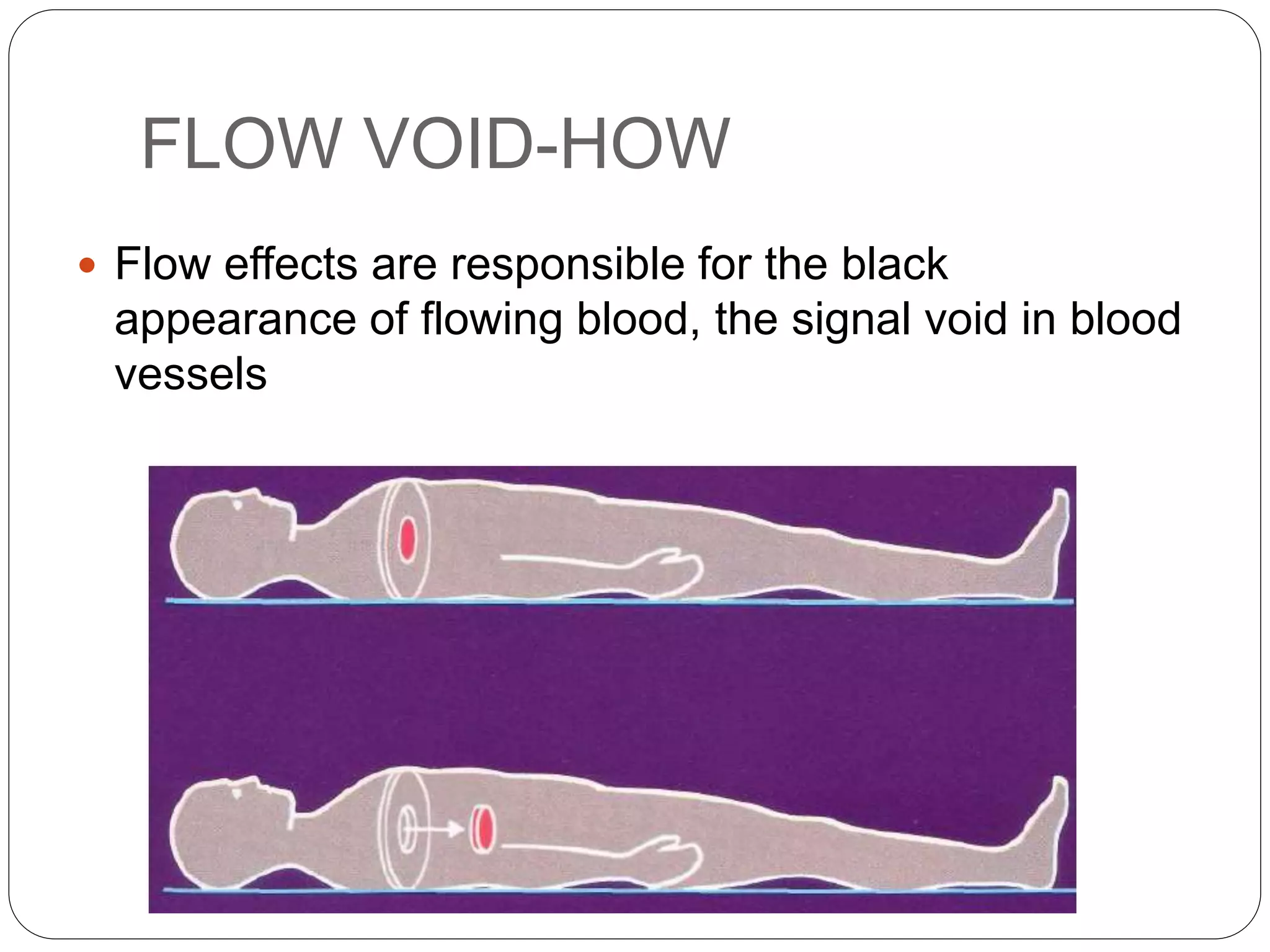
Details the use of various MR sequences in clinical evaluation. Discusses artifacts in MR imaging and their implications.
Thank you note from the presenter, concluding the educational session on MRI.