Downloaded 1,475 times


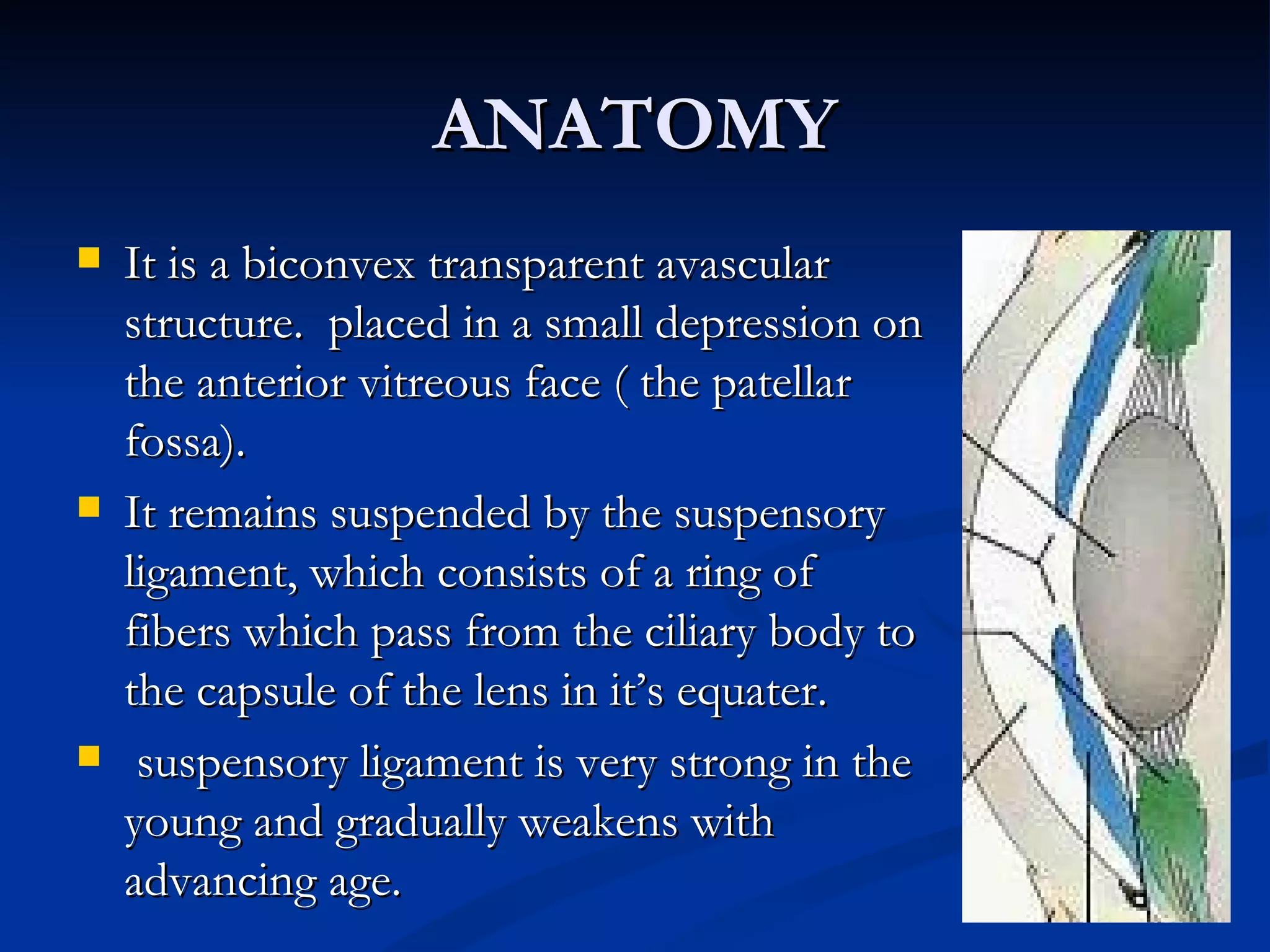








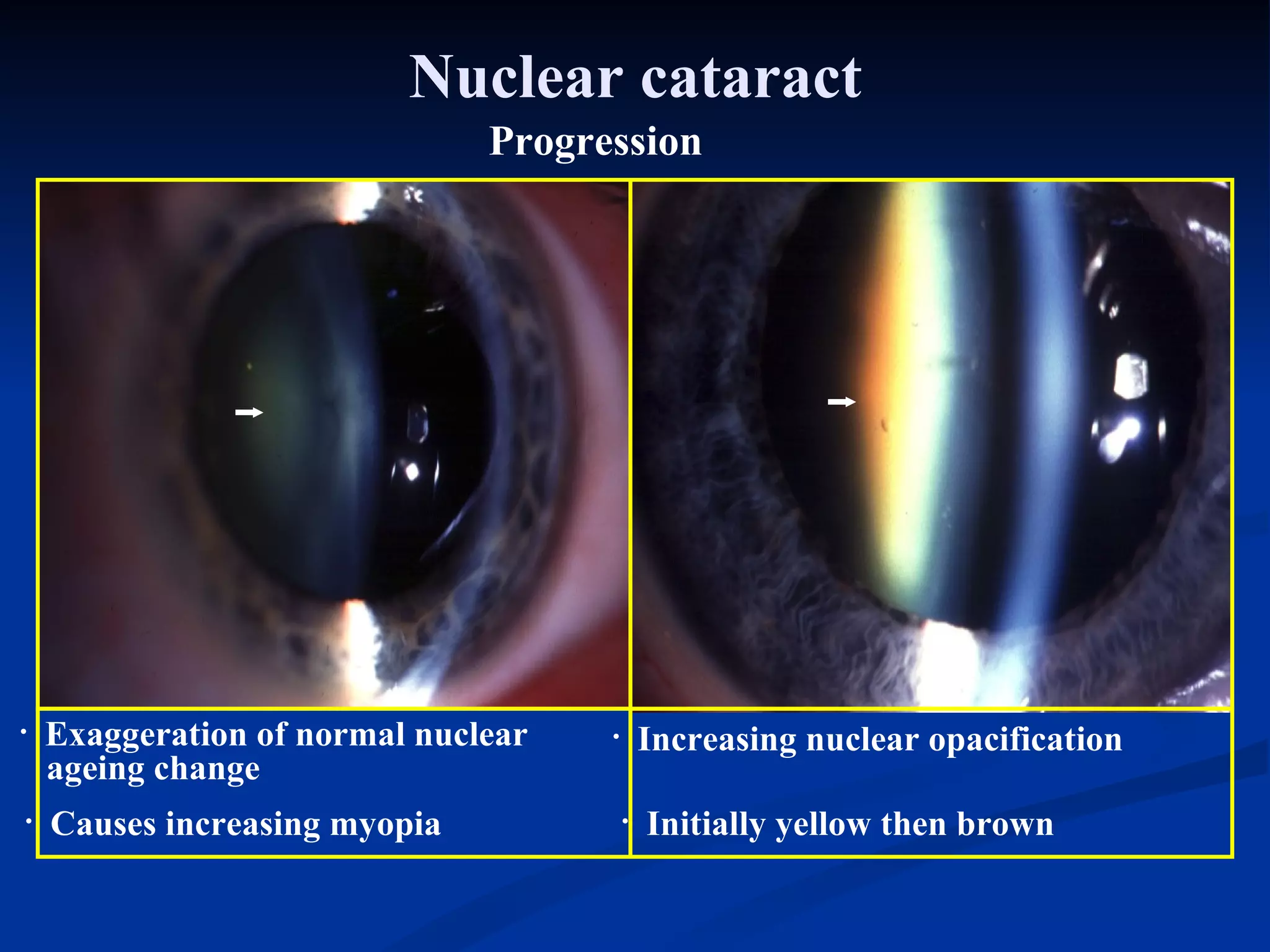



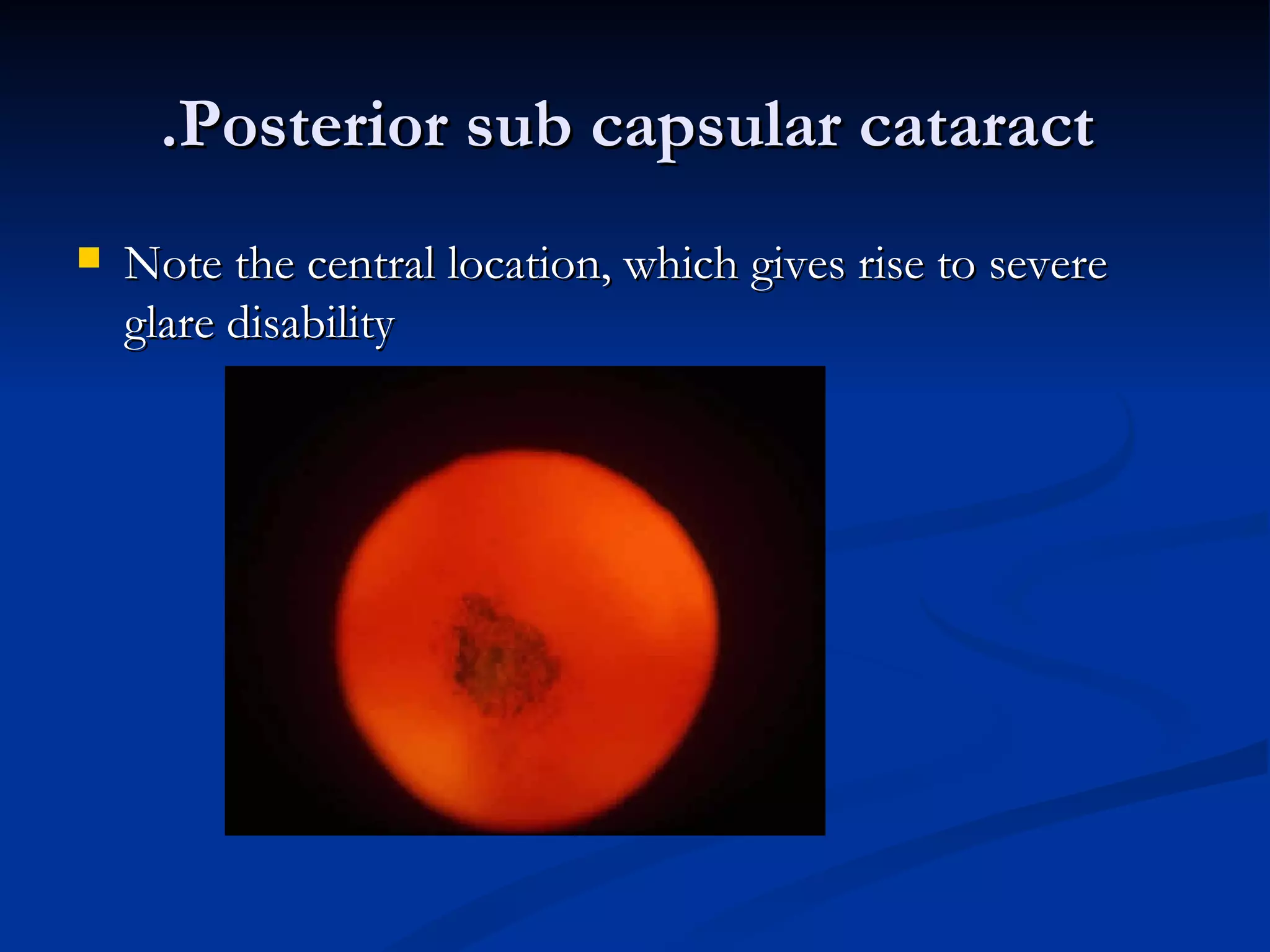

















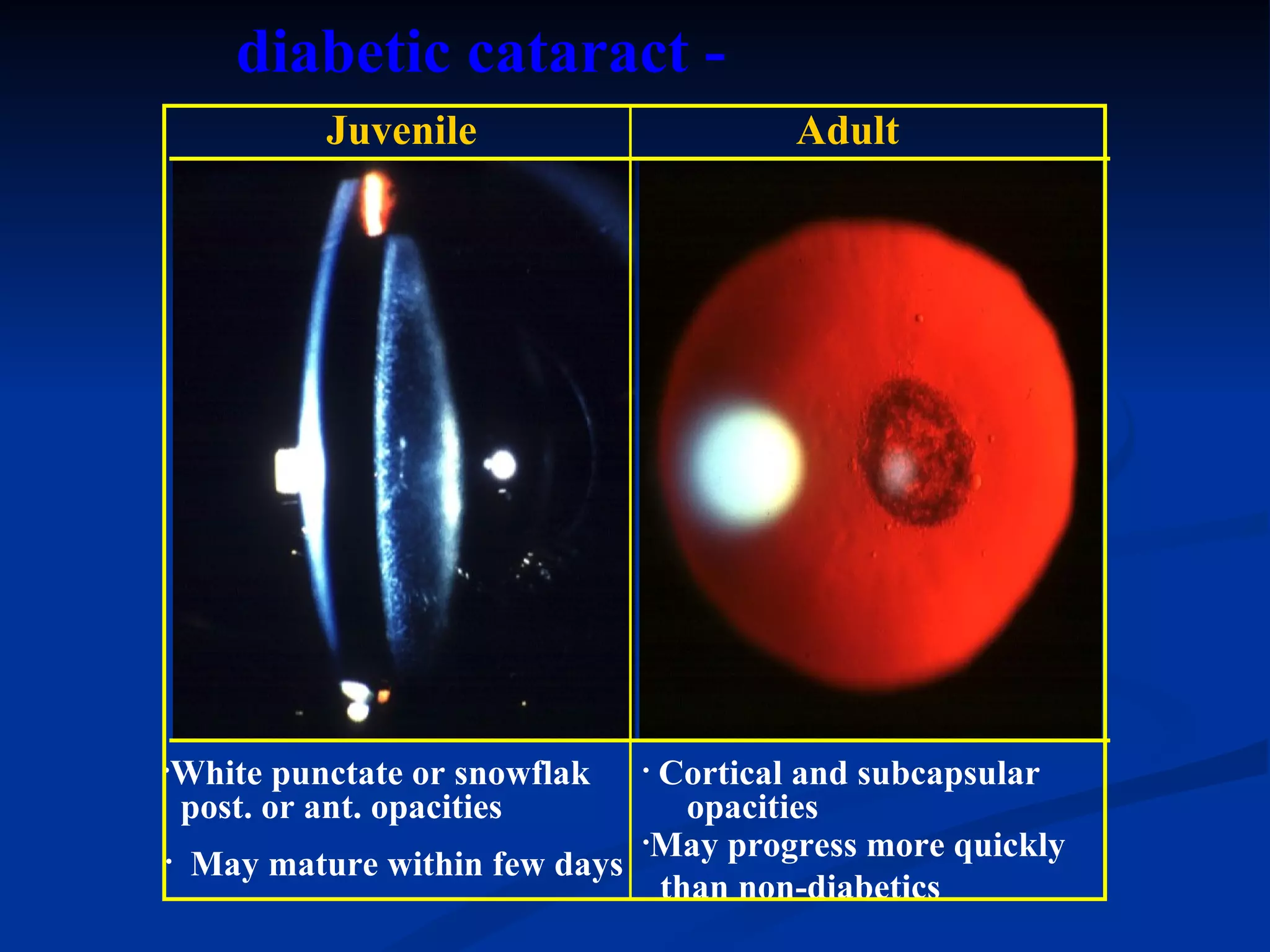






















The document discusses diseases of the crystalline lens, focusing on cataracts. It describes the anatomy of the lens and its layers. There are several types of cataracts described, including age-related (senile), traumatic, and congenital cataracts. Congenital cataracts can be caused by genetic mutations, infections, malnutrition, or other systemic diseases. The morphology, symptoms, and causes of different types of congenital cataracts are explained.











































































































