INTRODUCTION
● The lensis a transparent, biconvex structure
● The lens provides ~15 D refractive power
● The lens is derived from surface ectoderm cells overlying
the optic vesicle
● Lens transparency depends on the regular arrangement of
the lens fibers and of the cytoplasm within the fibers
● their disorganisation results in the development of cataract.
3.
● Cataract isdefined as opacity of clear lens which reduces
amount of light entering eye and results in deterioration of
vision.
● Cataract is the leading cause of preventable blindness.
4.
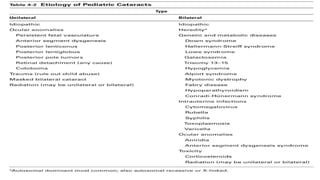
ETIOLOGICAL CLASSIFICATION :
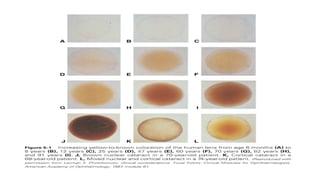
1. Congenital cataract
2. Acquired cataract
a. Age-related cataract
b. Toxic – smoking, drugs
c. Radiation
d. Systemic diseases
e. Ocular diseases
f. Trauma
g. Metabolic
Congenital Cataract:
presentat birth.
Infantile cataracts develop during the first year of life
fairly common, occurring in 1 of every 2000 live birth
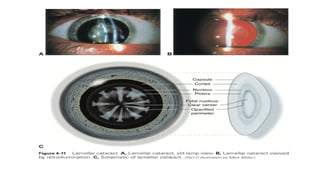
Lamellar :
Mostcommon
Bilateral and symmetric,
Opacifications of specific layers or zones of the lens
Opacified layer that surrounds a clearer center and is itself
surrounded by a layer of clear cortex.
Lamellar cataract disc shaped configuration.
Horseshoe shaped opacities riders.
14.
Polar :
● Subcapsularcortex and capsule of the anterior or posterior
pole of the lens.
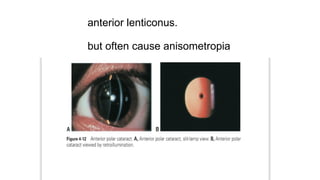
● Anterior polar cataracts small,bilateral, symmetric,
nonprogressive opacities that do not impair vision
● association with other ocular abnormalities
microphthalmia
persistent pupillary membrane,
Posterior polar cataracts
●profound decrease in vision than anterior polar cataracts
● positioned closer to the nodal point.
● Familial : usually bilateral and autosomal dominant.
● Sporadic : unilateral,
associated with remnants of the tunica vasculosa lentis
lenticonus or lentiglobus.
17.
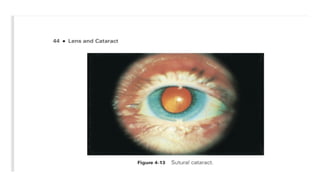
Sutural / Stellatecataract :
● Opacification of the Y- sutures of the fetal nucleus
● Bilateral
● Symmetric
● Inherited in an Autosomal Dominant pattern
19.
Coronary :
● consistof a group of club- shaped cortical opacities that are
arranged around the equator of the lens like a crown, or
corona.
Cerulean :
● Also known as blue- dot cataracts
● small bluish opacities located in the lens cortex
● nonprogressive
● do not cause visual symptoms.
21.
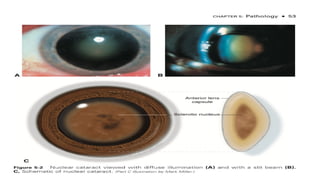
Nuclear :
● Opacitiesof the embryonic nucleus alone or of both
embryonic and fetal nuclei
● Bilateral
● Eyes with congenital nuclear cataracts tend to be
microphthalmic,
● They are at increased risk of developing aphakic glaucoma.
22.
Capsular
● lens epitheliumand anterior lens capsule
● differentiated from anterior polar cataracts by their
protrusion into the anterior chamber.
23.
Complete / Totalcataract :
● The red reflex is completely obscured
● Complete cataracts may be unilateral or bilateral,
● Profound visual impairment.
24.
Membranous
lens proteins areresorbed from either an intact or a
traumatized lens
the anterior and posterior lens capsules to fuse into
a dense white membrane
25.
Rubella :
● Maternalinfection with the rubella virus,
● RNA togavirus, can cause fetal damage,
● first trimester of pregnancy.
● pearly white nuclear opacifications.
● Sometimes the entire lens is opacified (complete cataract)
26.
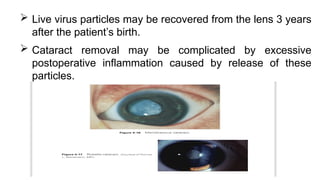
Live virusparticles may be recovered from the lens 3 years
after the patient’s birth.
Cataract removal may be complicated by excessive
postoperative inflammation caused by release of these
particles.
Age- Related LensChanges
As the lens ages,
As new layers of cortical fibers form concentrically
increases in mass and thickness and decreases in
accommodative power.
the lens nucleus compresses and hardens (a process
known as nuclear sclerosis).
29.
● Chemical modificationand proteolytic cleavage of
crystallins (lens proteins)
high- molecular- mass protein aggregates.
cause abrupt fluctuations in the local refractive
index of the lens,
scattering light and reducing transparency.
● Decreased concentrations of glutathione and
potassium and increased concentrations of sodium
30.
3 main typesof age- related cataracts:
(1) nuclear,
(2) cortical,
(3) posterior subcapsular.
32.
Nuclear Cataracts
Slowlyprogressive bilateral asymmetric.
Distance vision > near vision
Increase in the refractive index of the lens and a myopic
shift in refraction
Hyperopic or emmetropic eyes, the myopic shift enables
individuals to have improved distance vision or near vision
without the use of spectacles, a condition referred to as
second sight.
CORTICAL CATARCT
extensiveprotein oxidation and precipitation
A common symptom of cortical cataracts is glare from
intense focal light sources such as car headlights.
Monocular diplopia
37.
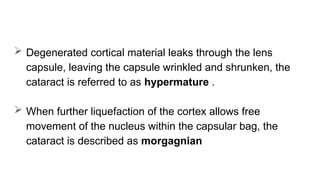
first visiblesigns of cortical cataract formation are vacuoles
and water clefts in the anterior or posterior cortex.
Wedge- shaped opacities form near the periphery of the
lens,
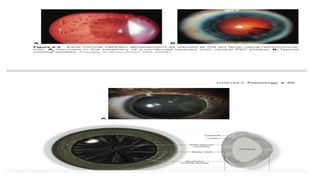
entire cortex, from the capsule to the nucleus,becomes
white and opaque, the cataract is said to be mature
38.
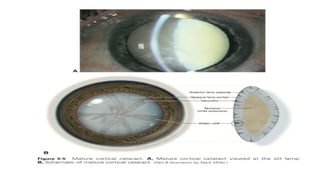
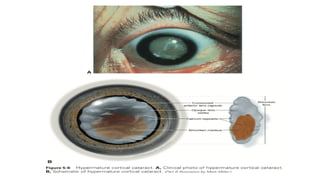
Degenerated corticalmaterial leaks through the lens
capsule, leaving the capsule wrinkled and shrunken, the
cataract is referred to as hypermature .
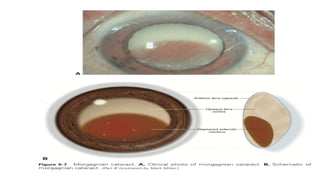
When further liquefaction of the cortex allows free
movement of the nucleus within the capsular bag, the
cataract is described as morgagnian
43.
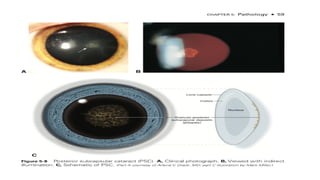
Posterior Subcapsular Cataracts:
Younger than those presenting with nuclear or cortical
cataracts.
First indication 1)subtle iridescent sheen in the posterior
cortical layer
2)granular opacities
3) a plaque like opacity of the posterior
subcapsular cortex
44.
Near vision> distance vision.
PSCs are associated with posterior migration of the lens
epithelial cells from the lens equator to the visual axis on
the inner surface of the posterior capsule.
47.
Drug- Induced LensChanges
Corticosteroids :
Long- term use of corticosteroids :
oral, topical,or inhaled corticosteroids
intraocular steroids,
slow release steroid repositories, subconjunctival and
Intravitreal implants
48.
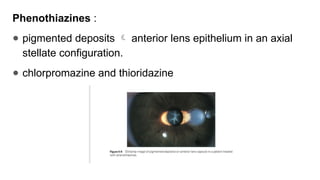
Phenothiazines :
● pigmenteddeposits anterior lens epithelium in an axial
stellate configuration.
● chlorpromazine and thioridazine
49.
Topical anticholinesterases :
small vacuoles within and posterior to the anterior lens
capsule and epithelium
cataract may progress to posterior cortical and nuclear
lens changes
Amiodarone :
Antiarrhythmic medication
50.
stellate pigmentdeposition in the anterior cortical axis
Amiodarone is also deposited in the corneal epithelium
(cornea verticillata) and can cause an optic neuropathy
.
51.
Statins :
concomitantuse of simvastatin and erythromycin,
Increases circulating statin levels, may be associated
with approximately a twofold increased risk of cataract.
Alves C, Mendes D, Batel Marques F. Statins and risk of cataracts: a systematic
review and metaanalysis of observational studies. Cardiovasc Ther.
2018;36(6):e12480
52.
Tamoxifen :
Antiestrogen
Used in the prevention and adjuvant treatment of breast
cancer,
PSC,
Crystalline maculopathy ,
Cystoid macular edema (CME)
53.
Trauma :
Mechanicalinjury
Physical forces radiation, chemicals, and electrical
current.
Contusion :
Vossius ring : pupillary ruff to be imprinted on the anterior
surface of the lens
54.
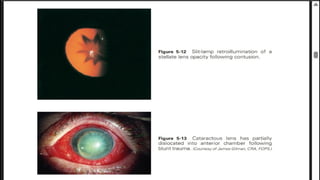
Traumatic cataract :
A stellate or rosette- shaped opacification (rosette
cataract),
Usually axial in location
Blunt trauma causes both dislocation and cataract
formation
56.
Symptoms andsigns of traumatic lens subluxation
Fluctuation of vision,
Impaired accommodation,
Monocular diplopia,
High astigmatism.
Iridodonesis
Phacodonesis is present.
Retroillumination dilated pupil may reveal the
zonular disruption
57.
Perforating or PenetratingInjury :
opacification of the cortex at the site of the rupture,
which usually progresses rapidly to complete opacification
59.
Intraocular Procedures
aftersurgery or following a longer period of healing.
Pars plana vitrectomy, especially with gas tamponade of the
retina,
A visually significant nuclear sclerotic cataract develops in
80%–100% of phakic eyes within 2 years of undergoing
vitrectomy.
Post vitrectomy cataracts are less common in patients younger
than 50 years
60.
Intravitreal injections direct trauma to the lens /
an adverse effect medications injected
Trabeculectomy :
The Collaborative Initial Glaucoma Treatment
Study found that glaucoma patients who were
initially treated with trabeculectomy were 8 times
more likely to need early cataract surgery than
those patients who were initially treated with
medications.
61.
Radiation
● 20 yearsafter exposure
● The first clinical signs of radiation-
1) Punctate opacities within the posterior capsule
2) Feathery anterior subcapsular opacities
62.
Infrared radiation :
1)The outer layers of the anterior lens capsule to
peel off as a single layer true exfoliation of the lens
capsule
2) Cortical cataract glassblower’s cataract
63.
Ultraviolet radiation :
Increased risk of cortical cataracts,
More frequently in men than women
American National Standards Institute (ANSI) requirements
aimed at reducing UV transmission. Using prescription
corrective lenses and nonprescription sunglasses decreases
UV exposure by more than 80%, and wearing a hat with a
brim decreases ocular sun exposure by 30%–50%
64.
Metallosis
Siderosis bulbi :
Iron molecules are deposited in the trabecular
meshwork, lens epithelium, iris, and retina
The epithelium and cortical fibers of the lens show a
yellowish tinge, followed by a rusty brown discoloration
Later manifestations : cortical cataract formation and
retinal dysfunction
66.
Chalcosis :
Depositscopper in DM, anterior lens capsule, other
intraocular basement membranes
Sunflower cataract : petal shaped deposition of yellow or
brown pigment in the lens capsule that radiates from the
anterior axial pole of the lens to the equator
Containing almost pure copper (more than 90%) can
cause a severe inflammatory reaction and intraocular
necrosis.
67.
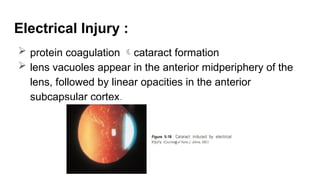
Electrical Injury :
protein coagulation cataract formation
lens vacuoles appear in the anterior midperiphery of the
lens, followed by linear opacities in the anterior
subcapsular cortex.
68.
Chemical Injuries :
Alkali injuries to the ocular surface often result in cataract
Alkali compounds penetrate the eye readily, causing an
increase in aqueous pH and a decrease in the level of
aqueous glucose and ascorbate
69.
Metabolic Cataract :
DiabetesMellitus :
Acute diabetic cataract or snowflake cataract, bilateral, subcapsular
Acute myopic shifts may indicate undiagnosed or poorly controlled
diabetes mellitus
accumulation of sorbitol within the lens
accompanying changes in hydration,
increased nonenzymatic glycosylation
of lens proteins,
greater oxidative stress.
from alterations in
lens metabolism
71.
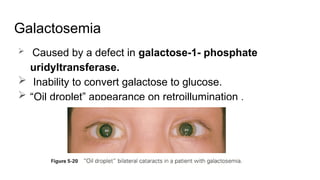
Galactosemia
Caused bya defect in galactose-1- phosphate
uridyltransferase.
Inability to convert galactose to glucose.
“Oil droplet” appearance on retroillumination .
72.
Hypocalcemia :
Bilateral,hypocalcemic (tetanic) cataracts are punctate
iridescent opacities in the anterior and posterior cortex.
lie beneath the lens capsule and are usually separated
from it by a zone of clear lens
73.
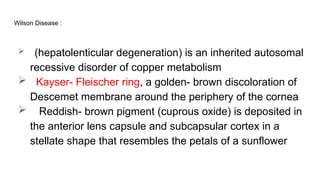
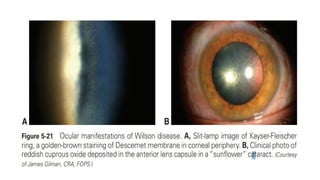
Wilson Disease :
(hepatolenticular degeneration) is an inherited autosomal
recessive disorder of copper metabolism
Kayser- Fleischer ring, a golden- brown discoloration of
Descemet membrane around the periphery of the cornea
Reddish- brown pigment (cuprous oxide) is deposited in
the anterior lens capsule and subcapsular cortex in a
stellate shape that resembles the petals of a sunflower
75.
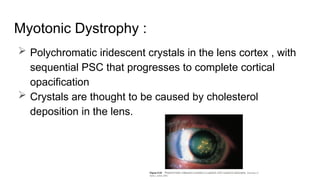
Myotonic Dystrophy :
Polychromatic iridescent crystals in the lens cortex , with
sequential PSC that progresses to complete cortical
opacification
Crystals are thought to be caused by cholesterol
deposition in the lens.
76.
Cataract Associated WithUveitis
Chronic uveitis or associated corticosteroid therapy
PSC develops, but anterior lens opacification may also
occur
Thickening of the anterior lens capsule,associated fibrous
pupillary membrane
Calcium deposits may be observed on the anterior
capsule
77.
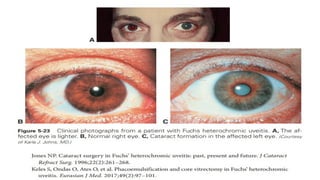
● Cortical cataractformation occurs in up to 70% of cases
of Fuchs heterochromic uveitis favorable prognosis
● Intraoperative anterior chamber hemorrhage at the time of
cataract surgery has been reported in approximately 8%–
25% of cases.
79.
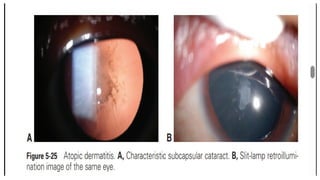
Cataract and AtopicDermatitis
Reported in 5%–38% of patients with Atopic dermatitis
Bilateral, and onset second to third decade of life,
Although cases in young children have been reported.
Anterior or posterior subcapsular opacities in the pupillary
area that resemble shieldlike plaques