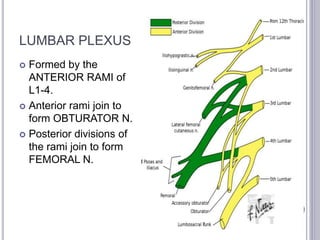
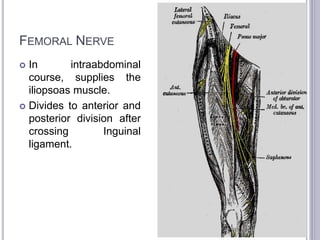
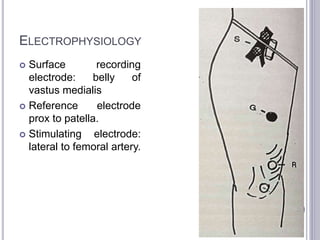
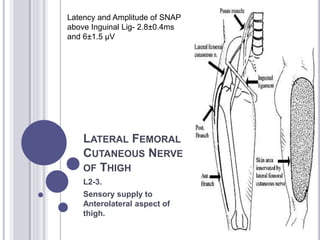
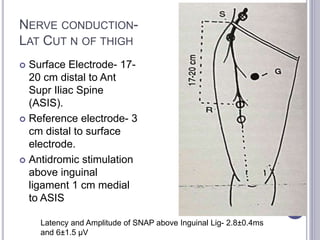
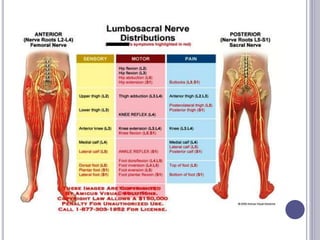
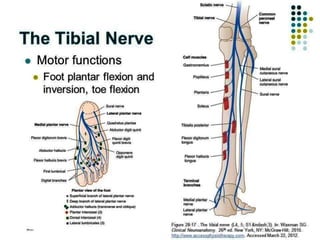
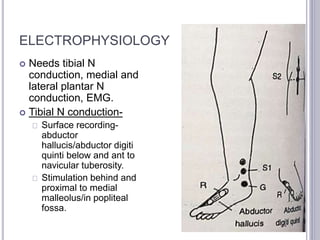
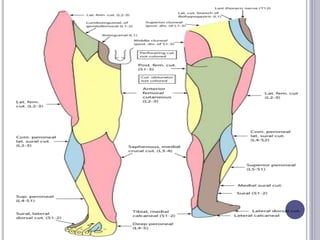
This document discusses the lumbar plexus and lower limb nerve conduction velocity (NCV), detailing the anatomy and clinical features associated with various neuropathies, including femoral, saphenous, lateral femoral cutaneous, sciatic, common peroneal, sural, and tibial nerves. It outlines symptoms, potential causes, and electrophysiological evaluation methods to diagnose conditions affecting these nerves, emphasizing the importance of nerve conduction studies and electromyography. Overall, the document provides a comprehensive overview of lower limb neuropathies and their diagnostic approaches.












































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





